Bowel Necrosis in Leptospirosis: A Case Series of a Rare Complication
Nalaka Herath, Sampath Hemachandra, Malaka Ranaweera, Asanka Sakalasooriya, Kosala Weerakoon, Shamila De Silva

TL;DR
This paper reports two cases of severe leptospirosis complicated by rare bowel necrosis, highlighting the importance of early recognition of gastrointestinal symptoms.
Contribution
The novelty lies in documenting rare gastrointestinal complications, specifically bowel necrosis, in severe leptospirosis cases.
Findings
Severe leptospirosis can lead to terminal ileal and colonic necrosis.
Gastrointestinal symptoms in leptospirosis may indicate severe disease requiring urgent intervention.
Despite aggressive treatment, patients with bowel necrosis in leptospirosis may have fatal outcomes.
Abstract
Leptospirosis, a globally prevalent zoonotic disease, exhibits diverse clinical manifestations, often with severe multiorgan involvement. Gastrointestinal complications are uncommon, but their potential severity and impact on patient outcomes warrant attention. We present two cases of severe leptospirosis complicated by terminal ileal and colonic necrosis. Two patients presented with acute febrile illness, severe myalgia, oliguria, and hypotension. Both had occupational exposure to paddy fields, a known risk factor for leptospirosis. Based on clinical presentation and laboratory findings (acute kidney injury, myocarditis, and acute severe pulmonary hemorrhagic syndrome), a diagnosis of severe leptospirosis was established. Development of proximal bowel obstruction and melena in the third week of illness indicated severe gastrointestinal involvement. Both patients received intensive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
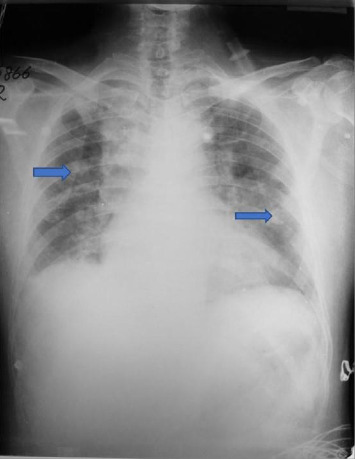 Figure 1
Figure 1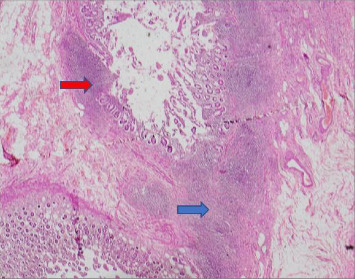 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeptospirosis research and findings · Brucella: diagnosis, epidemiology, treatment · Syphilis Diagnosis and Treatment
1. Introduction
Leptospirosis is the most common zoonotic disease across the globe caused by pathogenic spirochete Leptospira interrogans [1]. Human infection occurs through direct or indirect contact with urine of infected animals including pets, livestock, or wild/feral animals. Spread of infection is seasonal and occurs mostly during rainy seasons in the tropics [1, 2]. Sri Lanka is a tropical country reporting many cases of leptospirosis annually, with frequent outbreaks from different parts of the island [3].
Clinical presentations of leptospirosis range from a mild flu-like illness to multiorgan involvement. Organ involvement depends on the type and virulence of Leptospira and host susceptibility and varies widely, with hematological and renal involvement being the commonest [4]. Gastrointestinal involvement in leptospirosis is uncommon and includes pancreatitis, acalculous cholecystitis, and peritonitis [5–8]. We describe two rare cases of terminal ileal and proximal colonic necrosis following severe leptospirosis.
2. Case 1
A 55-year-old previously healthy man presented with fever, diarrhea, nausea, vomiting, myalgia, and dyspnea for three days after working in paddy fields. On admission, he was conscious, with low blood pressure (94/63 mmHg) and tachycardia (pulse rate 145 beats/min). There were bibasal lung crepitations, and urine output was only 10 mL over 4 hours. Admission blood tests indicated leucopenia and severe thrombocytopenia (Table 1).
After crystalloid fluid resuscitation noradrenaline was initiated to maintain blood pressure, intravenous ceftriaxone was commenced, and the patient was transferred to the medical intensive care unit (ICU). Due to severity of leptospirosis, intravenous methylprednisolone was administered for 3 days, and multiple platelet transfusions were given to correct thrombocytopenia. As oliguria persisted, intermittent hemodialysis was initiated. Dopamine was added due to persistent hypotension.
Chest radiograph indicated severe pulmonary hemorrhagic syndrome (Figure 1). Echocardiogram showed hypokinetic anterior wall motion and moderate mitral and tricuspid regurgitation. The patient was electively intubated and ventilated due to respiratory acidosis and hypoxia. Despite treatment, thrombocytopenia and abnormal liver function tests persisted (Table 1). Therapeutic plasma exchange was performed, and meropenem was commenced.
By Day 8, the patient was stable and afebrile, allowing for gradual withdrawal of inotropes. Leptospira microscopic agglutination test (MAT) became positive with a high titer. Blood picture showed low-grade hemolysis with a few red cell fragments.
On Day 21, the patient experienced fresh rectal bleeding. Upper gastroesophageal endoscopy revealed multiple gastric erosions, and colonoscopy revealed features of ischemic colitis. Blood and fresh frozen plasma were transfused, and intravenous proton pump inhibitor infusion was commenced. Exploratory laparotomy revealed extensive bowel necrosis from terminal ileum to the hepatic flexure with perforation and abscess formation of posterior wall of the ascending colon. Histopathology of affected areas confirmed these changes (Figure 2). There was no evidence of vasculitis in the rest of the peritoneal viscera. Standard right hemicolectomy and elective tracheostomy were performed.
On postoperative Day 1, the patient became unstable with hypotension and severe acidosis. Intact exteriorized bowel ends which had looked healthy at surgery showed features of ischemic necrosis. Since the patient's condition was unstable, further surgical exploration was abandoned. He succumbed on Day 27 of illness due to multiorgan failure.
3. Case 2
A 52-year-old man with Type 2 diabetes presented with fever, arthralgia, and myalgia for three days after working in paddy fields. On admission, he was febrile, icteric, dyspneic, and hypotensive (blood pressure 93/60 mmHg), with bibasal lung crepitations. He had not urinated for over 6 hours.
Initial tests indicated neutrophilic leukocytosis, severe thrombocytopenia, and elevated liver enzymes and serum creatinine (Table 2). Arterial blood gas analysis showed hypoxemia and metabolic acidosis with a lactate level of 7.1 mmol/L. Chest radiograph suggested severe pulmonary hemorrhagic syndrome. Leptospira MAT was positive at a titer of 1 : 640.
After fluid resuscitation noradrenaline was initiated, the patient was transferred to the ICU. He was electively intubated due to severe hypoxemia. Intravenous ceftriaxone was commenced. Renal replacement therapy by continuous venovenous hemodiafiltration was commenced, and multiple platelet concentrates were given to correct thrombocytopenia. Once stabilized, intermittent hemodialysis was initiated.
On Day 13, the patient developed blood-stained nasogastric aspirate and significant anemia. Upper gastrointestinal endoscopy revealed gastric erosions. Anemia was corrected with multiple blood transfusions. The patient was gradually improving by this time with no fever and minimum ventilator support until Day 15, when abdominal tenderness and sluggish bowel sounds were detected. There was intolerance of nasogastric feeds and melena. The abdomen was distended, and an anteroposterior radiograph (Figure 3) showed dilated multiple small bowel loops, a collapsed large bowel but no free gas in the peritoneal cavity. An ultrasound scan confirmed small bowel obstruction. The patient was hemodynamically unstable for contrast-enhanced abdominal computed tomography scan or for any surgical intervention. He succumbed on Day 21 of illness.
4. Discussion
Bowel perforation due to leptospirosis is a rare complication [5–9]. We describe two fatal cases of leptospirosis associated with bowel necrosis causing perforation. The clinical presentation of these two patients was complex, as they both developed multiple organ-related complications. Both patients presented with hypotension requiring inotropes and acute kidney injury requiring renal replacement therapy for more than 2 weeks. Both patients developed severe pulmonary hemorrhagic syndrome and acute myocarditis. All complications were managed in the ICU, and both patients were slowly recovering when bowel ischemia developed as a late complication in the third week of illness.
Colorectal manifestations are rare in leptospirosis [5, 9] and can be easily missed due to the complexity of cases. Gastrointestinal involvement is diverse, ranging from ulcers to necrosis and perforation with peritoneal sepsis [5–9]. These severe complications are attributed to the inherent pathogenicity of different strains as well as host immunopathological responses, while the exact pathophysiology is not fully described. Bowel ischemia and perforation may be due to complex interactions of various tissue-injuring factors, namely, hemolysis, endotoxins, and lipase [5–8]. Vasculitis of capillaries may contribute to ischemia and necrosis [4, 5]. Hemorrhagic complications may also occur secondary to disease activity, coagulopathy, and thrombocytopenia [10, 11]. Prolonged hypotension and the use of inotropes may contribute to ongoing ischemic necrosis.
Bowel ischemia and necrosis due to leptospirosis are not a common case for a surgeon since it is an extremely rare condition. Especially in a healthy individual without prior risk factors for mesenteric ischemia, the diagnosis itself is challenging. Since no real data are available to predict which leptospirosis patient would develop gut ischemia, to decide early surgical intervention is extremely difficult.
Mesenteric vasculitis, a rare condition, can be challenging to diagnose due to nonspecific symptoms and the rarity of the disease. However, it might be useful to do CT angiogram/CECT abdomen and pelvis, in patients with presentations like these two cases, when such patients are not improving with conventional treatment for leptospirosis and are showing unorthodox clinical features such as bowel obstruction or gut ischemia.
Both our patients had lower gastrointestinal bleeding indicative of severe terminal ileal and colonic involvement with leptospirosis during the convalescent period. This could be related to Leptospira antigen-associated vasculoendothelial damage. [12]. This may also be due to prolonged hypotension causing bowel ischemia, as the third week of illness is too late for direct invasion of Leptospira and immune-related complications. Although watershed areas of the intestines are the splenic flexure and rectosigmoid junction, the first patient had ischemic necrosis in the terminal ileum, cecum, and proximal colon, which are generally considered to have good blood supply.
Bowel necrosis was confirmed in Case 1, but it was not possible to histologically confirm the same in Case 2. This is a limitation of this case series. However, bowel necrosis was strongly suspected in Case 2 based on clinical deterioration and signs of intestinal obstruction.
5. Conclusion
Bowel necrosis following severe leptospirosis carries a poor prognosis. Specific mechanisms of pathogenesis are unclear. Severe gastrointestinal complications may be attributed to the inherent pathogenicity of different strains or host immunopathological responses. Prolonged hypotension and the use of inotropes may contribute to ongoing bowel ischemia and necrosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Karpagam K. B. Ganesh B. Leptospirosis: A Neglected Tropical Zoonotic Infection of Public Health Importance-An Updated Review European Journal of Clinical Microbiology & Infectious Diseases 202039583584610.1007/s 10096-019-03797-431898795 · doi ↗ · pubmed ↗
- 2Hacker K. P. Sacramento G. A. Cruz J. S. Influence of Rainfall on Leptospira Infection and Disease in a Tropical Urban Setting, Brazil Emerging Infectious Diseases 202026231131410.3201/eid 2602.19010231961288 PMC 6986844 · doi ↗ · pubmed ↗
- 3Warnasekara J. Srimantha S. M. Agampodi S. B. Estimating the Burden of Leptospirosis: Global Lessons From Sri Lanka BMJ Global Health 2021610 p. e 00694610.1136/bmjgh-2021-006946 PMC 855213434706880 · doi ↗ · pubmed ↗
- 4De Brito T. Silva A. M. G. Abreu P. A. E. Pathology and Pathogenesis of Human Leptospirosis: A Commented Review Revista do Instituto de Medicina Tropical de São Paulo 2018600 p. e 2310.1590/s 1678-99462018600232-s 2.0-85047815546 PMC 597555729846473 · doi ↗ · pubmed ↗
- 5Zamri Z. Shaker A. H. Razman J. Leptospirosis Complicating With Acute Large Bowel Gangrene: A Case Report Clinica Terapeutica 2012163539940023099969 · pubmed ↗
- 6Mazhar M. Kao J. J. Bolger D. T. A 23 Year-Old Man With Leptospirosis and Acute Abdominal Pain Hawai’i Journal of Medicine & Public Health 2016751029129427738562 PMC 5056631 · pubmed ↗
- 7Maier A. Kaeser R. Thimme R. Boettler T. Acute Pancreatitis and Vasoplegic Shock Associated With Leptospirosis – A Case Report and Review of the Literature BMC Infectious Diseases 2019191 p. 39510.1186/s 12879-019-4040-12-s 2.0-85065526236 PMC 650705131068145 · doi ↗ · pubmed ↗
- 8Herath N. J. Kamburapola C. J. Agampodi S. B. Severe Leptospirosis and Pancreatitis; A Case Series From a Leptospirosis Outbreak in Anuradhapura District, Sri Lanka BMC Infectious Diseases 2016161 p. 64410.1186/s 12879-016-2010-42-s 2.0-84996587706 PMC 510010727821124 · doi ↗ · pubmed ↗