Complete Resection of Mucinous Liver Cyst Initially Masked as a Hydatid Cyst
Ricardo Cruzalegui, Amanda Humpire, Juan Nuñez Ju, Erick Vasquez, Cecilia Yeren

TL;DR
A rare liver tumor initially mistaken for a hydatid cyst was completely removed in two surgeries to prevent future complications.
Contribution
The paper presents a case of two-stage complete resection for a mucinous liver cyst with malignant potential.
Findings
MCN-L is a rare liver tumor occurring in less than 5% of cystic liver tumors.
Complete surgical resection is the optimal treatment to prevent malignancy and recurrence.
The case highlights the importance of accurate diagnosis and staged surgical approaches.
Abstract
Hepatic cystic mucinous neoplasm is a low-prevalence tumor with malignant potential. Due to its infrequent presentation, it is often misdiagnosed and inadequately treated. The purpose of the present work is to report a case, review the corresponding literature, determine the most optimal surgical treatment option, and contrast it with what has been performed. A 53-year-old female patient with upper hemiabdomen pain and elevated serum liver enzyme levels. Computed tomography revealed a multilocular cystic liver tumor measuring 52 mm × 63 mm between segments 4 and 5. The patient underwent a first surgery, laparoscopic unroofing. The anatomopathological result was mucinous cystic neoplasm (MCN-L) without malignancy. With the result, a second surgery was scheduled to complete the resection of the remaining cyst, and an open left hepatectomy was performed. MCN-L of the liver is an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
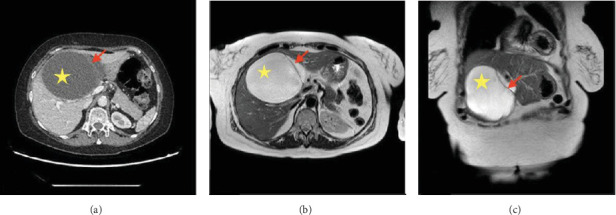 Figure 1
Figure 1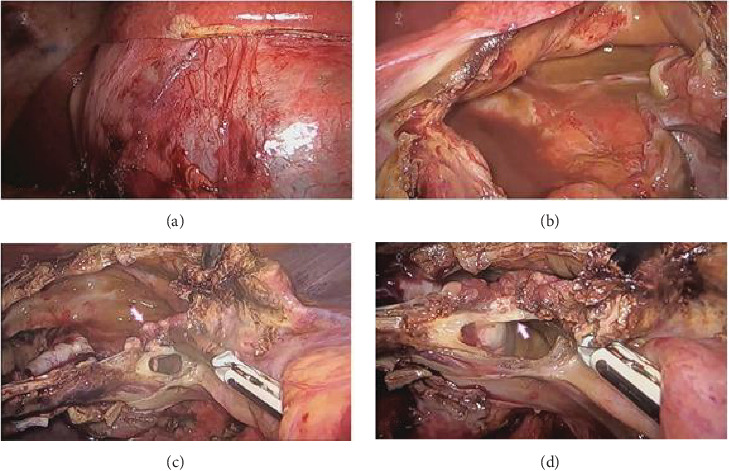 Figure 2
Figure 2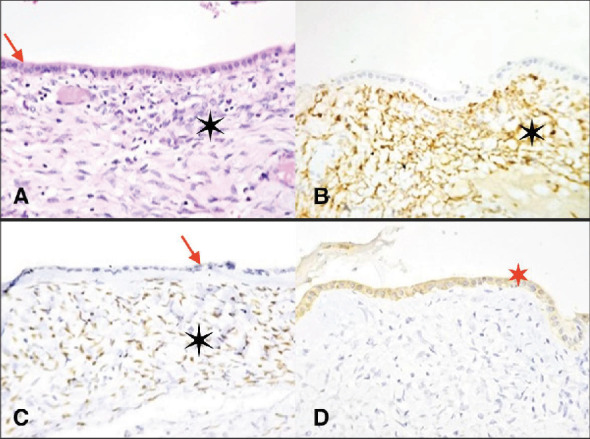 Figure 3
Figure 3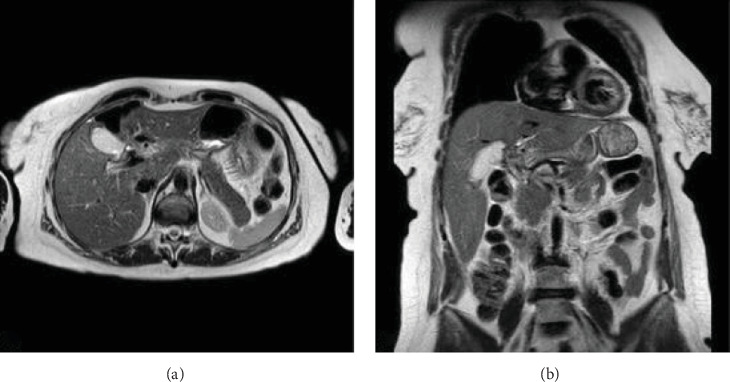 Figure 4
Figure 4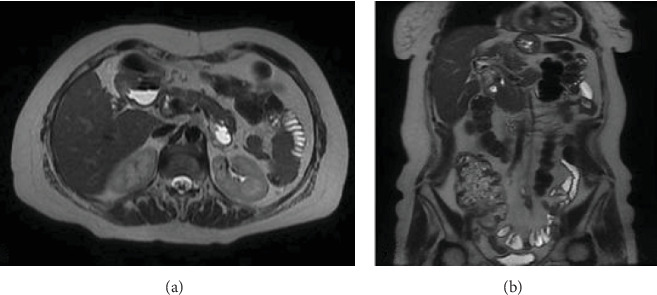 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Genetic and Kidney Cyst Diseases · Congenital Anomalies and Fetal Surgery
1. Introduction
Hepatic cysts are the most frequent lesions of the liver, with a prevalence of approximately 20% of the population. Of these, only 5% correspond to cystic mucinous neoplasms [1]. The World Health Organization (WHO) has classified mucin-producing bile duct tumors into two distinct entities: hepatic mucinous cystic neoplasm (MCN-L) and intraductal papillary mucinous neoplasm of the bile duct (IPMN-B) [2], neoplasms that were initially called cystadenoma or cystadenocarcinoma [3].
MCN-L, first described in 1958 as a multilocular cystic lesion [4], is an infrequent presenting tumor, occurring mainly in middle-aged women [5]. It is defined as an epithelial neoplasm composed of a monolayer of mucin-producing cubic or columnar epithelium associated with ovarian-type stroma, which has no communication with the bile ducts [6]. Due to the scarce literature on this condition, misdiagnosis in the preoperative period is common; a better prognosis is obtained when surgical resection is complete (with up to 100% survival at 5 years) [3]. We present the clinical case of a patient with hepatic MCN-L treated in the hepatobiliary surgery service of our hospital.
2. Presentation of the Case
A 53-year-old female patient presented with an episode of abdominal pain of moderate intensity in the right upper quadrant with no previous trigger during the 3 months before hospitalization. On physical examination, the abdomen was soft, depressible, without masses, and not painful on palpation. In the laboratory, there were alterations in serum levels of liver enzymes: gamma-glutamyl transpeptidase 151 U/L (VN: 0–30), alkaline phosphatase 899 U/L (VN: 30–120 U/L), alanine transaminase 55 U/L (VN: 0–50), and aspartate transaminase 66 U/L (0–45). However, serum bilirubin level was in the normal range (0.4 mg/dL), as well as carcinoembryonic antigen (2 U/mL), CA 19.9 (2 U/mL) and alpha-fetoprotein (1.5 U/mL) values. No antibodies against Echinococcus were detected.
A previous abdominal ultrasound performed at the reference hospital describes a cystic, heterogeneous liver lesion that does not cause dilatation of the intrahepatic bile duct.
An abdominal CT scan revealed the presence of a 62 mm × 53 mm multilocular cystic tumor located between segments 4 and 5 of the liver (Figure 1). Magnetic resonance imaging showed the presence of a hyperintense cystic tumor in T1 with a septum and high signal intensity in the diffusion sequence, in the location already described, being considered a hepatic hydatid cyst (Figure 1). Computed tomography and magnetic resonance imaging did not reveal dilatation of the intrahepatic bile ducts or communication between the tumor and the bile ducts.
Based on these findings, a preoperative diagnosis of hepatic hydatidosis vs. hepatic cyst was made, and laparoscopic unroofing was performed, which was chosen because of the high prevalence of hydatid disease in our population [7] and the patient's epidemiological history. In our institution we opt for parenchymal-sparing surgery in benign pathology.
During surgery, a cyst located between segments 4 and 5, with a thick white wall, partially protruding from the hepatic surface, with serous liquid content (Figures 2A,B) and the presence of a septum inside (Figures 2C,D); intraoperative cholangiography did not show any communication with the biliary tract. There was no spillage of the cystic content into the cavity, and intraoperative blood loss was scarce. The patient was discharged on the fourth day of surgery without postoperative complications.
The anatomic pathology result was reported as fibrous-looking tissue and the presence of cystic formations of serous content measuring 10 cm × 8.5 cm × 0.7 cm, with no signs of malignancy. Positive immunohistochemistry for estrogen and progesterone receptors confirmed an ovarian-type stroma. Histologically, the tumor was diagnosed as an intrahepatic mucinous cyst (Figure 3).
With this result, the patient was scheduled to complete the resection of the remaining mucinous cyst (Figure 4). Open left hepatectomy with lymphadenectomy was performed, where the remaining cyst wall was identified as adhered to the hepatic pedicle and enlarged lymph nodes of lymph node groups number 8 and 12. Intraoperative blood loss was 150 cc, and the patient was discharged on the fifth day of surgery without complications.
He is currently undergoing outpatient controls, with no signs of recurrence of the cystic lesion (Figure 5). However, he has presented variable alterations in the values of alkaline phosphatase and gamma-glutamyl transpeptidase without presenting stenosis of the main biliary tract in the control images.
3. Discussion
Mucinous tumors originate in organs such as the ovary or pancreas, being rare in the presentation in the liver [5], so it is scarcely reported in the literature.
MCN-L of the liver is clearly defined as an epithelial neoplasm lined with cubic or columnar cells, cyst-forming, mucin-producing, having no communication with the bile ducts, associated with an ovarian-type stroma, and expressing progesterone and estrogen receptors. It has been demonstrated that it generally occurs in women between 28 and 75 years [4]. When invasive cancer is present, the levels of tumor markers CA 19.9 and CEA in the cyst fluid are usually elevated [8].
MCN-L is known to have the potential for malignant transformation. It is classified as low, intermediate, high grade, and associated invasive carcinoma. Making a definitive diagnosis preoperatively is often difficult. In clinical practice, it should be differentiated from liver cyst, bile duct cyst, endometriosis cyst, hepatic echinococcosis, papillary bile duct tumor, and hepatic abscess, these being differential diagnoses. The main characteristic that distinguishes MCN-L is that it has no communication with the intrahepatic bile ducts, presents ovarian-type stroma, and occurs in middle-aged female patients.
In general, MCN-L presents as a low-density mass with internal septa that shows enhancement with intravenous contrast on CT. On T2-weighted MRI, MCN-L presents as a multilocular cystic mass containing fluid with varying signal intensities in the different loculi [9].
Mucinous tumors of the liver are often misdiagnosed and inadequately treated, with the possibility of disease recurrence or possible malignant transformation [10, 11]. The prognosis is good if the resection is complete [12].
Preoperative needle biopsy is challenging due to the lack of solid tissue in hepatic cystic lesions. When malignant degeneration is suspected, the most appropriate treatment is complete resection, strictly following oncologic criteria [13, 14].
In the present case, it was decided to complete the resection by performing an open left hepatectomy in a second surgical intervention after the positive histological study for mucinous neoplasm of the liver.
4. Conclusion
We present a case of L-CNM with complete resection in two stages because this tumor, although benign, has a high potential for malignancy and recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aziz H. Hamad A. Afyouni S. Kamel I. R. Pawlik T. M. Management of Mucinous Cystic Neoplasms of the Liver Journal of Gastrointestinal Surgery 20232791963197010.1007/s 11605-023-05709-637221388 · doi ↗ · pubmed ↗
- 2Nakanuma Y. Curado M.-P. Franceschi S. WHO Classification of Tumours of the Digestive System 2010 WH Op. 4
- 3Wittekind C. Fischer H. P. Ponchon T. Hamilton S. R. Aaltonen A. L. Bile Duct Cystadenoma and Cystadenocarcinoma WHO Classification of Tumours. Pathology and Genetics of Tumours of the Digestive System 20002 IARC press
- 4Edmondson H. A. Tumors of the Liver and Intrahepatic Bile Ducts: Atlas of Tumors Pathology, Sect VII, Fascicle 25 1958 Armed Forces Institute of Pathology
- 5Zen Y. Pedica F. Patcha V. R. Mucinous Cystic Neoplasms of the Liver: A Clinicopathological Study and Comparison With Intraductal Papillary Neoplasms of the Bile Duct Modern Pathology 20112481079108910.1038/modpathol.2011.712-s 2.0-7996102441621516077 · doi ↗ · pubmed ↗
- 6Kubota K. Nakanuma Y. Kondo F. Clinicopathological Features and Prognosis of Mucin-Producing Bile Duct Tumor and Mucinous Cystic Tumor of the Liver: A Multi-Institutional Study by the Japan Biliary Association Journal of Hepato-Biliary-Pancreatic Sciences 201421317618510.1002/jhbp.232-s 2.0-8489039518023908126 · doi ↗ · pubmed ↗
- 7Vanessa G. Hernan F. Revista Peruana de Medicina Experimental y Salud Publica 262193197
- 8Koffron A. Rao S. Ferrario M. Abecassis M. Intrahepatic Biliary Cystadenoma: Role of Cyst Fluid Analysis and Surgical Management in the Laparoscopic Era 200413692693610.1016/j.surg.2004.06.03115467680 · doi ↗ · pubmed ↗