Cerebral Vasospasm as a Delayed Complication Following Glioblastoma Resection
Andrew C. Pickles, John T. Tsiang, Shiau-Sing Ciecierska, Ronak H. Jani, Joseph C. Serrone, Brandon J. Bond, Jigisha P. Thakkar, Vikram C. Prabhu

TL;DR
A patient developed cerebral vasospasm after glioblastoma surgery, showing it can occur similarly to post-subarachnoid hemorrhage vasospasm.
Contribution
Reports a rare case of cerebral vasospasm following glioblastoma resection and highlights its management.
Findings
Cerebral vasospasm occurred 8 days after glioblastoma resection with neurological deficits.
Treatment with intra-arterial CCB and induced hypertension resolved most deficits.
Early recognition and intervention are critical to prevent permanent cerebral ischemia.
Abstract
Postoperative cerebral vasospasm is usually triggered by vasoactive metabolic blood products in the subarachnoid space but is rarely reported following resection of intrinsic diffuse lobar neoplasms such as malignant gliomas. This 34-year-old right-handed Caucasian lady underwent an uneventful resection of a right mesial temporal lobe glioblastoma with no postoperative neurological deficits. Eight days after her index surgery, she presented with left-sided hemiparesis and dysarthria and was found to have right M1 narrowing, consistent with cerebral vasospasm. Intra-arterial calcium channel blocker (CCB) administration and induced hypertension were started to treat the cerebral vasospasm and resulted in resolution of most of her neurological deficits. At 2 months postresection, she was noted to be without neurological deficits and able to proceed with appropriate adjuvant therapies for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
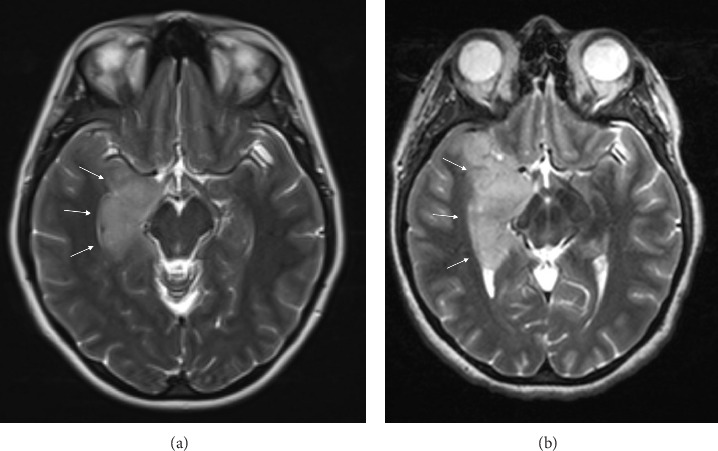 Figure 1
Figure 1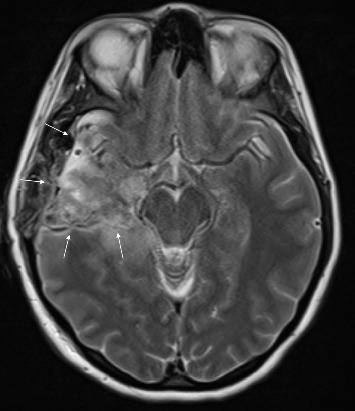 Figure 2
Figure 2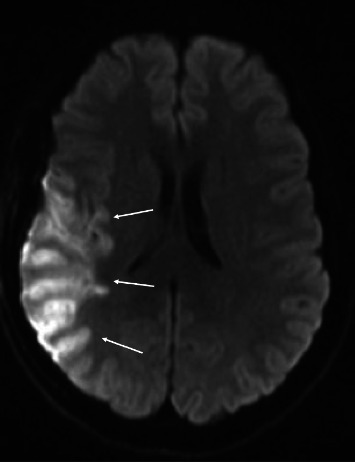 Figure 3
Figure 3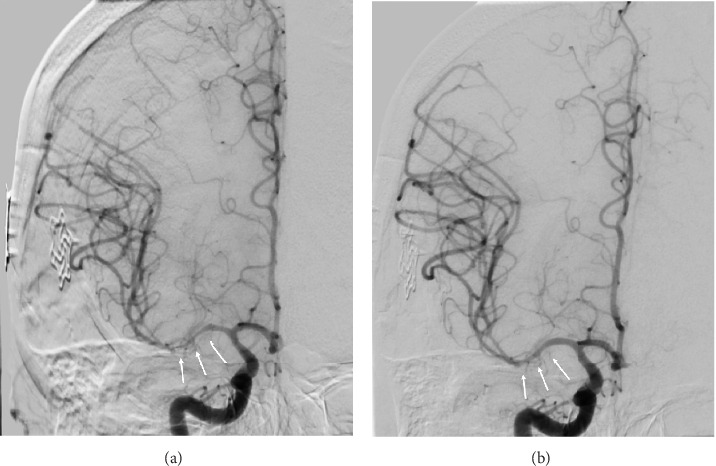 Figure 4
Figure 4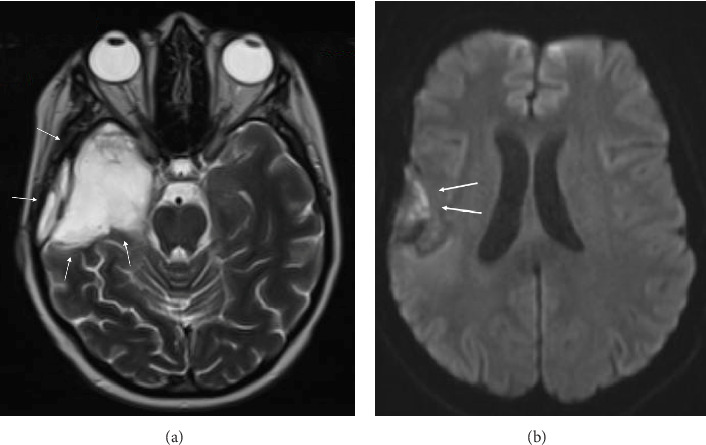 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological Complications and Syndromes · Intracranial Aneurysms: Treatment and Complications · Brain Metastases and Treatment
1. Introduction
Glioblastoma multiforme (GBM) is the most common primary malignant brain tumor in adults [1]. The standard of care involves maximal safe resection followed by concurrent radiation and temozolomide (TMZ), maintenance TMZ, and tumor treatment fields as per the Stupp protocol [2–7]. Surgical resection of malignant gliomas usually targets the contrast-enhancing portion of the tumor, but there is growing evidence that maximal safe resection of the nonenhancing T2/FLAIR hyperintense component of the tumor may also have a salutary effect on overall survival [8, 9]. Surgical adjuncts such as the use of 5-ALA or sodium fluorescein are employed to aid with tumor visualization along with the use of intraoperative neuronavigation and ultrasound; some centers have access to intraoperative magnetic resonance imaging (MRI) as well [10]. These tumors can violate the pial boundaries and encase or involve major cerebral arterial vessels.
Cerebral vasospasm is most commonly encountered in clinical practice following spontaneous aneurysmal subarachnoid hemorrhage (SAH) and is postulated to be caused by the breakdown of vasoactive metabolic blood products in the subarachnoid space [11]. It has also been reported following resection of cranial base tumors, as these frequently extend into the basal cisterns involving the major arteries or their branches and perforators [12–15]. In these cases, factors associated with a higher likelihood of postresection cerebral vasospasm are reported to be vessel encasement, vessel narrowing, tumor size, hypothalamic dysregulation, and subarachnoid blood in the resection cavity [16–18]. Treatment for cerebral vasospasm and its sequelae initially involves administration of nimodipine, establishment of euvolemia, and systemic hypertensive therapy. Endovascular treatment includes intra-arterial (IA) calcium channel blockers (CCBs) and balloon angioplasty [19–22].
We report a case of cerebral vasospasm following resection of a mesial temporal lobe glioblastoma that presented in a manner similar to cerebral vasospasm following aneurysmal SAH and was treated successfully using similar principles as would be employed in the setting of post-SAH cerebral vasospasm. Our intent is to draw attention to this rare phenomenon that may complicate the recovery of a patient following glioblastoma resection and to provide an effective treatment algorithm that may mitigate any neurological deficits and facilitate the use of adjuvant therapies.
2. Case Presentation
This 34-year-old female presented with a generalized tonic–clonic seizure and was found to have a right mesial temporal lobe T2/FLAIR hyperintense lesion (Figure 1(a)) without associated contrast enhancement. She was started on levetiracetam and referred to our facility. Three months later, her MRI revealed a significant increase in the area of T2/FLAIR hyperintensity (Figure 1(b)).
She underwent a right temporal craniotomy and resection of the tumor. The surgical margins extended to the floor of the middle cranial fossa inferiorly, temporal pole anteriorly, and to the pia adjacent to the brainstem. In some areas, minor violations of the pia mater allowed blood products to enter into the basal cisterns and subarachnoid space. Copious saline irrigation was employed to wash out these blood products from the subarachnoid space and basal cisterns. The right superior cerebellar artery, posterior cerebral artery, and middle cerebral artery (MCA) were visualized and carefully protected with cotton patties. At the conclusion of the operation, the resection bed was gently lined with hemostatic product, the bone flap was replaced, and the scalp was closed appropriately. No intraoperative complications were encountered during the procedure. The patient awoke from anesthesia without any apparent deficits, and a routine postoperative MRI demonstrated a small residual T2 abnormality in the right posterior hippocampus (Figure 2).
The patient was discharged home 4 days after index surgery after an uneventful hospital stay. Pathology demonstrated an IDH wild-type, MGMT unmethylated GBM.
Eight days after surgery, the patient presented with a sudden onset of left facial droop, left sided hemiparesis, and dysarthria. A CT angiogram demonstrated right M1 narrowing with decreased distal MCA opacification along the right parietal lobe. No large vessel occlusion (LVO) was noted. An MRI revealed diffusion restriction of the right MCA territory (Figure 3).
The patient's left-sided hemiparesis then self-resolved, with only a trace left upper extremity drift and left sided facial weakness remaining. Given the suspicion for vasospasm, the patient was allowed permissive hypertension to a systolic blood pressure < 180 mm Hg. A diagnostic cerebral angiogram (DCA) was performed on postoperative day (POD) nine noting severe vasospasm noted in the right M1 and proximal M2 (Figure 4(a)). 20 mg of IA verapamil and 10 mg IA nicardipine were injected in the right internal carotid artery (ICA), resulting in significant improvement in vessel caliber (Figure 4(b)).
After the procedure, her systolic blood pressure was maintained between 140–150 mm Hg for the duration of her hospital admission with norepinephrine. The patient was also started on oral nimodipine 60 mg every 4 hours for 7 days to promote vessel patency. Bedside transcranial Doppler (TCD) ultrasound obtained the next day demonstrated elevated Lindegaard ratios [23], suggesting that the patient was still in vasospasm, and she was taken back to the endovascular suite for a repeat DCA. The patient was again noted to have severe vasospasm of the right M1, and 20 mg IA verapamil and 10 mg IA nicardipine were administered to the right ICA with restoration of vessel caliber. Continued TCD velocity elevations suggested persistent vasospasm but the patient refused further treatment after the second intervention. Her neurological exam steadily improved and she was discharged home 10 days after her index admission.
At 2-week follow-up, the patient had full strength in her left hemibody with subtle left-sided facial weakness. She was started on the Stupp protocol for treatment of her GBM 1 month after her initial resection. At 3 months postresection, she had no focal neurologic deficits and was tolerating chemoradiation treatment well. MRI obtained demonstrated no recurrence of the lesion on both T1-weighted postcontrast and T2-weighted sequences (Figure 5(a)) and resolution of DWI abnormalities (Figure 5(b)).
3. Discussion
Although postresection perilesional ischemia is frequently noted following a malignant glioma resection, cerebral vasospasm is rare. Prior anecdotal reports suggest peri-Sylvian tumor resections may be at higher risk for vasospasm, particularly if there is surgical entry into the basal cisterns and Sylvian fissure, or contamination of these regions with blood products [24]. This may have been the pathophysiology of the vasospasm noted in our case. Research from SAH-induced vasospasm suggests that the breakdown of blood products in the subarachnoid space may produce vasoactive metabolites that activate calcium-dependent and independent channels that contribute to vasospasm [11].
A PubMed search was performed using the phrases “Glioma AND Vasospasm” and “Glioblastoma AND Vasospasm” on November 20, 2024. A total of 29 articles were identified. Twenty-six articles were excluded because they did not contain subject matter relevant to GBM resection complicated by cerebral vasospasm or were not available in English text. One article was excluded due to postoperative Streptococcus oralis meningitis preceding the development of vasospasm after GBM resection [25]. Two articles were included in our analysis detailing two patients with GBM resection complicated by cerebral vasospasm (Table 1).
In our review of the literature and present case, two of the three patients were female, and the mean age was 49.9 years (range 35–63). All three cases involved GBMs of the temporal lobe with two tumors also involving the insula. In the two cases reported in the prior literature, there was no description of blood in the basal cisterns. All three cases noted expected postoperative brain edema on routine imaging. In the two cases reported in prior literature, the surgeons had placed carmustine wafers in the resection cavity. Carmustine wafers were not used in our present case. In all three cases, vessels affected by vasospasm were noted to either be displaced or encased by the GBM; however, no direct vessel injury was noted during any of the procedures. Average time to symptomatic vasospasm was 9.3 days postoperatively (range 8–12 days). Two of the three cases were treated in the endovascular suite with IA CCBs, and in three cases, nimodipine was continued for several days postangiography. One case of vasospasm resulted in permanent left upper extremity plegia and left lower extremity paresis, while another resulted in severe hemiparesis even after rehabilitation. Our case demonstrated recovery with minimal persistent deficits.
Placement of carmustine wafers (Gliadel, Azurity Pharmaceuticals, Inc., Woburn, MA, USA) in the resection cavity is also purported to contribute to arterial vasospasm. However, they were not employed in our case, and we have not experienced vasospasm in other cases in which these wafers were deployed in the resection cavity. One theory proffered is that carmustine has vasoactive properties that may be responsible for vasospasm, especially in instances where large cerebral vessels are in close proximity to the resection cavity [21, 26]. Cerebral edema and a cytotoxic inflammatory marker release may also contribute to vasospasm. Cerebral vasospasm following skull base tumor resection is described in approximately 2% of patients generally associated with meningioma resections [15]. However, arterial vasospasm has also been reported following pituitary adenoma resections, and more rarely vestibular schwannomas [22, 27], particularly in patients with thick subarachnoid blood or intraparenchymal hemorrhage following surgery. Larger lesions with parasellar extension are at an even higher risk for vasospasm following surgical resection.
Similar to post-SAH vasospasm, the average time of onset of symptoms related to vasospasm following glioma resection appears to be 8–12 days following surgery, and the clinical deficits reflect the arterial territory involved. Hence, once other possible etiologies for a new-onset neurological deficit > 1 week out from surgery, such as seizures, infection, or hematoma formation, have been ruled out with appropriate imaging studies and electroencephalography, it is advisable to evaluate the cerebral vasculature for possible vasospasm. TCD, cerebrovascular perfusion studies (i.e., CT perfusion), CT or MR angiography, and catheter angiography of the cerebral vessels allow recognition of vasospasm [28–30]. Initial imaging should follow clinical stroke guidelines, by first employing a noncontrast CT scan to rule out hemorrhage, followed by a CT perfusion scan to identify areas with reduced blood flow, and CT angiography to rule out LVO [28]. If CT angiography is equivocal, MR angiography may be employed due to its greater sensitivity detecting subtle ischemic changes and identifying the ischemic core [29]. CT and MR perfusion studies are especially useful for identifying penumbra [30], or salvageable tissue surrounding the irreversibly damaged ischemic core, the extent of which may help guide treatment and prognostic discussions. TCD is a noninvasive means of monitoring for vasospasm and response to therapies [23, 31]; TCD velocities have a sensitivity and specificity of 69.2% and 84.4%, respectively, and by Lindegaard ratios, the sensitivity and specificity are 76.9% and 87.4%, respectively [23, 31]. However, while TCDs can be used to determine resolution of vasospasm, they should be supplemented by careful clinical examinations and cerebral perfusion studies or catheter angiography, if needed. In all three cases, there were focal vessel vasospasms with localizing symptoms. There were no reports of distal or diffuse vasospasm, which can most often be observed after SAH [11].
It is important for clinicians to recognize the signs of postoperative vasospasm, however rare the clinical entity may be. Prompt recognition allows for early institution of therapies; IA CCBs supplemented by intravenous or oral CCBs were effective in the case reported here. A delay in recognition of cerebral vasospasm and timely institution of vasodilatory therapies may result in permanent deficits that further complicate and negatively impact adjuvant therapies for the malignant glioma [32–35]. Endovascular DCA with intervention allows recognition of the vasospasm and administration of IA CCBs; in some instances, angioplasty of the vasospastic vessel may also be performed [36]. Systemic vasodilating CCBs may also be administered [36]. In our case, oral nimodipine was only administered for 7 days due to issues with hypotension following administration, symptomatic improvement, and a desire to wean the patient off vasopressors prior to discharge. However, the typical duration of therapy is 60 mg every 4 h for 21 days, based on recommendations for reducing vasospasm in SAH after ruptured cerebral aneurysms [37].
This represents a hybrid approach to treatment that combines systemic treatment traditionally used for SAH-induced vasospasm, with endovascular interventions targeted toward restoring focal flow deficits. To prophylactically treat vasospasm, some providers are borrowing techniques from aneurysm surgeries, including irrigating intraoperatively with dilute vasodilator, or lining the resection cavities with papaverine-soaked gel foam [38]. It is unclear at this time the efficacy of these techniques. Postoperative cerebral vasospasm may follow uncomplicated surgical resection of a malignant glioma. The timeline of clinical presentation and the radiographic studies reveal a similar semiology as noted with post-SAH vasospasm. Prompt recognition and treatment of symptomatic vasospasm is essential to restore vessel caliber and prevent irreversible delayed cerebral ischemia, morbidity, and/or mortality and also allows resumption or continuation of adjuvant therapies for the primary brain tumor.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Omuro A. De Angelis L. M. Glioblastoma and Other Malignant Gliomas: A Clinical Review JAMA 2013310171842185010.1001/jama.2013.2803192-s 2.0-8488710262324193082 · doi ↗ · pubmed ↗
- 2Annavarapu S. Gogate A. Pham T. Davies K. Singh P. Robert N. Treatment Patterns and Outcomes for Patients With Newly Diagnosed Glioblastoma Multiforme: A Retrospective Cohort Study CNS Oncology 202110310.2217/cns-2021-0007 PMC 846175434378977 · doi ↗ · pubmed ↗
- 3Bonosi L. Marrone S. Benigno U. E. Maximal Safe Resection in Glioblastoma Surgery: a Systematic Review of Advanced Intraoperative image-guided Techniques Brain Sciences 2023132 p. 21610.3390/brainsci 13020216 PMC 995458936831759 · doi ↗ · pubmed ↗
- 4Lakomy R. Kazda T. Selingerova I. Real-World Evidence in Glioblastoma: Stupp’s Regimen After a Decade Frontiers Oncology 202010 p. 84010.3389/fonc.2020.00840 PMC 734805832719739 · doi ↗ · pubmed ↗
- 5Omuro A. Brandes A. A. Carpentier A. F. Radiotherapy Combined With Nivolumab or Temozolomide for Newly Diagnosed Glioblastoma With Unmethylated MGMT Promoter: an International Randomized Phase III Trial Neuro-Oncology 202325112313410.1093/neuonc/noac 09935419607 PMC 9825306 · doi ↗ · pubmed ↗
- 6Stupp R. Mason W. P. van den Bent M. J. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma New England Journal of Medicine 20053521098799610.1056/nejmoa 0433302-s 2.0-2004436616315758009 · doi ↗ · pubmed ↗
- 7Stupp R. Taillibert S. Kanner A. Effect of tumor-treating Fields plus Maintenance Temozolomide Vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma: A Randomized Clinical Trial JAMA 2017318232306231610.1001/jama.2017.187182-s 2.0-8504003396229260225 PMC 5820703 · doi ↗ · pubmed ↗
- 8Karschnia P. Vogelbaum M. A. van den Bent M. Evidence-Based Recommendations on Categories for Extent of Resection in Diffuse Glioma European Journal of Cancer 2021149233310.1016/j.ejca.2021.03.00233819718 · doi ↗ · pubmed ↗