Epidemiology and Prognostic Role of HPV Infection in Head and Neck Cancer: A Population‐Based Study of the SEER Database
Kangwen Guo, Jinmei Li, Haiyin Ye, Xiaoqiong Yi

TL;DR
This study analyzes data from the SEER database to explore how HPV infection affects the prognosis of head and neck cancer patients.
Contribution
The study provides population-based evidence on the prognostic impact of HPV in head and neck cancer using large-scale data.
Findings
HPV-positive head and neck cancer cases generally have better survival rates than HPV-negative cases.
HPV positivity is not associated with improved prognosis in nasopharyngeal carcinoma and gum-originating cancers.
Subgroup analysis confirmed better survival outcomes for HPV-positive patients across most categories.
Abstract
Head and neck cancer (HNC) comprises a heterogeneous group of malignancies with significant variation in epidemiology, clinical features, and treatment responses. However, large‐scale data on the clinical epidemiology of HNC and the prognostic impact of human papillomavirus (HPV) infection have not yet been reported. Data on HNC cases with known HPV status were obtained from the Surveillance, Epidemiology, and End Results (SEER) database. Clinical characteristics of HNC were summarized based on HPV status, primary site, and metastatic site. To elucidate the prognostic role of HPV status in HNC, we calculated the relative survival rate (RSR) and conducted Cox regression analysis following propensity score matching by HPV status. A total of 14,855 HNC cases were included in this study, comprising 10,128 HPV‐positive and 4727 HPV‐negative cases. Clinical characteristics varied based on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
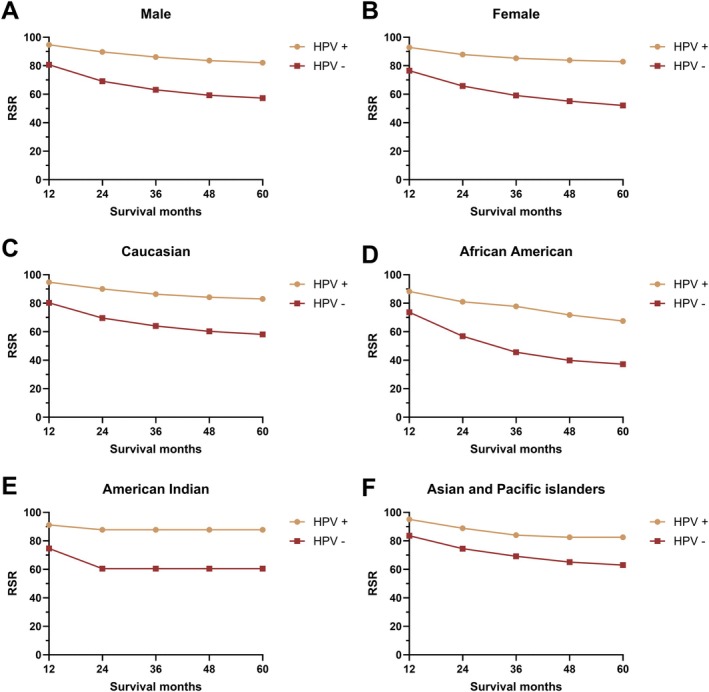 FIGURE 1
FIGURE 1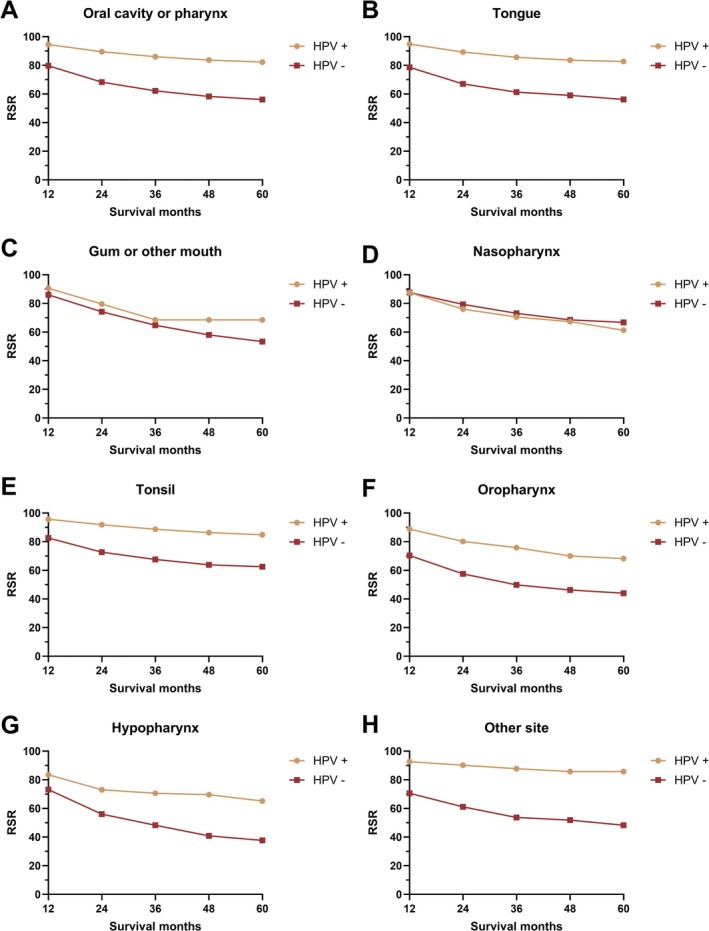 FIGURE 2
FIGURE 2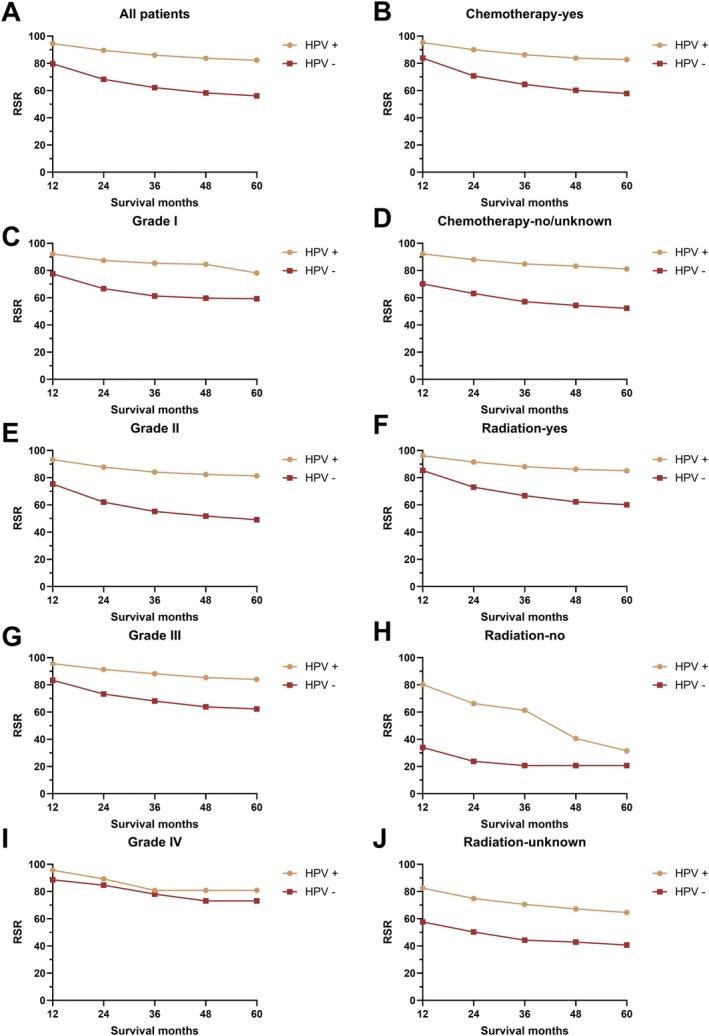 FIGURE 3
FIGURE 3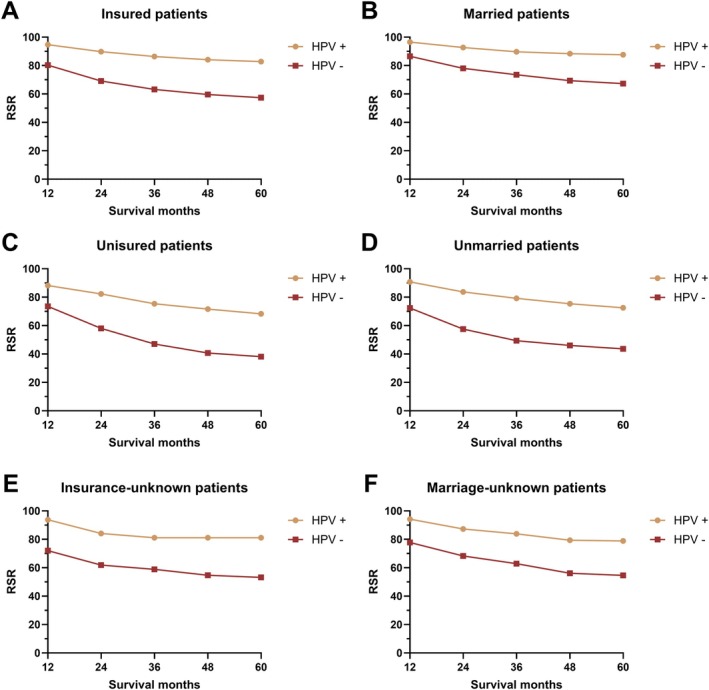 FIGURE 4
FIGURE 4| Categories | All cases | Original data | Matched data | ||||
|---|---|---|---|---|---|---|---|
| HPV (+) cases | HPV (−) cases |
| HPV (+) cases | HPV (−) cases |
| ||
| All cases | 14,855 | 10,128 | 4727 | 3550 | 3550 | ||
| Sex | < 0.001 | > 0.05 | |||||
| Male |
12,364 (83.2) |
8770 (86.6) |
3594 (76.0) |
2805 (79.0) |
2829 (79.7) | ||
| Age | < 0.001 | > 0.05 | |||||
| Mean (SD) |
53.93 (10.28) |
53.54 (9.6) |
54.77 (11.54) |
54.28 (10.76) |
54.42 (10.82) | ||
| 0–45 |
2779 (18.7) |
1917 (18.9) |
862 (18.2) |
690 (19.4) |
645 (18.2) | ||
| 46–60 |
8479 (57.1) |
6007 (59.3) |
2472 (52.3) |
1887 (53.2) |
1943 (54.7) | ||
| 61–75 |
3236 (21.8) |
2035 (20.1) |
1201 (25.4) |
865 (24.4) |
858 (24.2) | ||
| 75+ |
361 (2.4) |
169 (1.7) |
192 (4.1) |
108 (3.0) |
104 (2.9) | ||
| Race | < 0.001 | > 0.05 | |||||
| White |
12,682 (85.4) |
9073 (89.6) |
3609 (76.3) |
2890 (81.4) |
2909 (81.9) | ||
| AI |
121 (0.8) |
73 (0.7) |
48 (1.0) |
38 (1.1) |
32 (0.9) | ||
| API |
760 (5.1) |
336 (3.3) |
424 (9.0) |
222 (6.3) |
208 (5.9) | ||
| AA |
1189 (8.0) |
571 (5.6) |
618 (13.1) |
375 (10.6) |
375 (10.6) | ||
| Unknown |
103 (0.7) |
75 (0.7) |
28 (0.6) |
25 (0.7) |
26 (0.7) | ||
| Year of diagnosis | < 0.001 | > 0.05 | |||||
| 2010 |
901 (6.1) |
557 (5.5) |
344 (7.3) |
259 (7.3) |
257 (7.2) | ||
| 2011 |
1414 (9.5) |
827 (8.2) |
587 (12.4) |
402 (11.3) |
411 (11.6) | ||
| 2012 |
1788 (12.0) |
1127 (11.1) |
661 (14.0) |
474 (13.4) |
470 (13.2) | ||
| 2013 |
2240 (15.1) |
1510 (14.9) |
730 (15.4) |
549 (15.5) |
547 (15.4) | ||
| 2014 |
2585 (17.4) |
1794 (17.7) |
791 (16.7) |
587 (16.5) |
607 (17.1) | ||
| 2015 |
2765 (18.6) |
2005 (19.8) |
760 (16.1) |
593 (16.7) |
583 (16.4) | ||
| 2016 |
3162 (21.3) |
2308 (22.8) |
854 (18.1) |
686 (19.3) |
675 (19.0) | ||
| Site | < 0.001 | > 0.05 | |||||
| Gum and other mouth |
307 (2.1) |
64 (0.6) |
243 (5.1) |
64 (1.8) |
84 (2.4) | ||
| Hypopharynx |
811 (5.5) |
204 (2.0) |
607 (12.8) |
201 (5.7) |
224 (6.3) | ||
| Nasopharynx |
890 (6.0) |
285 (2.8) |
605 (12.8) |
278 (7.8) |
278 (7.8) | ||
| Oropharynx |
955 (6.4) |
543 (5.4) |
412 (8.7) |
330 (9.3) |
302 (8.5) | ||
| Other oral cavity and pharynx |
307 (2.1) |
157 (1.6) |
150 (3.2) |
104 (2.9) |
112 (3.2) | ||
| Tongue |
4935 (33.2) |
3662 (36.2) |
1273 (26.9) |
1139 (32.1) |
1180 (33.2) | ||
| Tonsil |
6650 (44.8) |
5213 (51.5) |
1437 (30.4) |
1434 (40.4) |
1370 (38.6) | ||
| Differentiation | < 0.001 | > 0.05 | |||||
| Grade I |
452 (3.0) |
213 (2.1) |
239 (5.1) |
152 (4.3) |
143 (4.0) | ||
| Grade II |
4254 (28.6) |
2589 (25.6) |
1665 (35.2) |
1174 (33.1) |
1204 (33.9) | ||
| Grade III |
6033 (40.6) |
4422 (43.7) |
1611 (34.1) |
1283 (36.1) |
1299 (36.6) | ||
| Grade IV |
370 (2.5) |
183 (1.8) |
187 (4.0) |
107 (3.0) |
98 (2.8) | ||
| Unknown |
3746 (25.2) |
2721 (26.9) |
1025 (21.7) |
834 (23.5) |
806 (22.7) | ||
| Surgery | < 0.001 | > 0.05 | |||||
| Surgery |
5047 (34.0) |
3773 (37.3) |
1274 (27.0) |
1111 (31.3) |
1066 (30.0) | ||
| Tumor destruction |
10 (0.1) |
5 (0.0) |
5 (0.1) |
4 (0.1) |
5 (0.1) | ||
| No |
9765 (65.7) |
6330 (62.5) |
3435 (72.7) |
2422 (68.2) |
2470 (69.6) | ||
| Unknown |
33 (0.2) |
20 (0.2) |
13 (0.3) |
13 (0.4) |
9 (0.3) | ||
| Radiotherapy | < 0.001 | > 0.05 | |||||
| Yes |
12,685 (85.4) |
8901 (87.9) |
3784 (80.1) |
2894 (81.5) |
2935 (82.7) | ||
| Refused |
176 (1.2) |
123 (1.2) |
53 (1.1) |
57 (1.6) |
39 (1.1) | ||
| Unknown |
1994 (13.4) |
1104 (10.9) |
890 (18.8) |
599 (16.9) |
576 (16.2) | ||
| Chemotherapy | < 0.001 | > 0.05 | |||||
| Yes |
10,560 (71.1) |
7325 (72.3) |
3235 (68.4) |
1131 (31.9) |
1063 (29.9) | ||
| Insurance | < 0.001 | > 0.05 | |||||
| Insured |
14,049 (94.6) |
9678 (95.6) |
4371 (92.5) |
3301 (93.0) |
3311 (93.3) | ||
| Uninsured |
529 (3.6) |
290 (2.9) |
239 (5.1) |
162 (4.6) |
156 (4.4) | ||
| Unknown |
277 (1.9) |
160 (1.6) |
117 (2.5) |
87 (2.5) |
83 (2.3) | ||
| Marriage | < 0.001 | > 0.05 | |||||
| Married |
8539 (57.5) |
6221 (61.4) |
2318 (49.0) |
1780 (50.1) |
1876 (52.8) | ||
| Unmarried |
5544 (37.3) |
3414 (33.7) |
2130 (45.1) |
1548 (43.6) |
1473 (41.5) | ||
| Unknown |
772 (5.2) |
493 (4.9) |
279 (5.9) |
222 (6.3) |
201 (5.7) | ||
| Lung metastasis | < 0.001 | > 0.05 | |||||
| NA |
2 (0.0) |
0 (0.0) |
2 (0.0) |
0 (0.0) |
1 (0.0) | ||
| No |
14,405 (97.0) |
9905 (97.8) |
4500 (95.2) |
3407 (96.0) |
3415 (96.2) | ||
| Unknown |
162 (1.1) |
96 (0.9) |
66 (1.4) |
60 (1.7) |
44 (1.2) | ||
| Yes |
286 (1.9) |
127 (1.3) |
159 (3.4) |
83 (2.3) |
90 (2.5) | ||
| Brain metastasis | < 0.001 | > 0.05 | |||||
| NA |
2 (0.0) | 0 |
2 (0.0) |
0 (0.0) |
1 (0.0) | ||
| No |
14,681 (98.8) |
10,036 (99.1) |
4645 (98.3) |
3490 (98.3) |
3493 (98.4) | ||
| Unknown |
144 (1.0) |
83 (0.8) |
61 (1.3) |
52 (1.5) |
43 (1.2) | ||
| Yes |
28 (0.2) |
9 (0.1) |
19 (0.4) |
8 (0.2) |
13 (0.4) | ||
| Liver metastasis | < 0.001 | > 0.05 | |||||
| NA |
2 (0.0) | 0 |
2 (0.0) |
0 (0.0) |
1 (0.0) | ||
| No |
14,591 (98.2) |
9989 (98.6) |
4602 (97.4) |
3459 (97.4) |
3473 (97.8) | ||
| Unknown |
140 (0.9) |
83 (0.8) |
57 (1.2) |
51 (1.4) |
39 (1.1) | ||
| Yes |
122 (0.8) |
56 (0.6) |
66 (1.4) |
40 (1.1) |
37 (1.0) | ||
| Bone metastasis | < 0.001 | > 0.05 | |||||
| NA |
3 (0.0) |
1 (0.0) |
2 (0.0) |
0 (0.0) |
1 (0.0) | ||
| No |
14,512 (97.7) |
9957 (98.3) |
4555 (96.4) |
3443 (97.0) |
3439 (96.9) | ||
| Unknown |
143 (1.0) |
79 (0.8) |
64 (1.4) |
49 (1.4) |
44 (1.2) | ||
| Yes |
197 (1.3) |
91 (0.9) |
106 (2.2) |
58 (1.6) |
66 (1.9) | ||
| T stage | < 0.001 | > 0.05 | |||||
| 0 |
64 (0.4) |
50 (0.5) |
14 (0.3) |
16 (0.5) |
10 (0.3) | ||
| 1 |
3502 (23.6) |
2582 (25.5) |
920 (19.5) |
710 (20.0) |
727 (20.5) | ||
| 2 |
4844 (32.6) |
3557 (35.1) |
1287 (27.2) |
1014 (28.6) |
1017 (28.6) | ||
| 3 |
2473 (16.6) |
1568 (15.5) |
905 (19.1) |
662 (18.6) |
651 (18.3) | ||
| 4 |
2320 (15.6) |
1327 (13.1) |
993 (21.0) |
674 (19.0) |
677 (19.1) | ||
| NA |
365 (2.5) |
189 (1.9) |
176 (3.7) |
120 (3.4) |
131 (3.7) | ||
| TX |
1287 (8.7) |
855 (8.4) |
432 (9.1) |
354 (10.0) |
337 (9.5) | ||
| N stage | < 0.001 | > 0.05 | |||||
| 0 |
2366 (15.9) |
1311 (12.9) |
1055 (22.3) |
683 (19.2) |
664 (18.7) | ||
| 1 |
2701 (18.2) |
1755 (17.3) |
946 (20.0) |
758 (21.4) |
703 (19.8) | ||
| 2 |
8505 (57.3) |
6310 (62.3) |
2195 (46.4) |
1728 (48.7) |
1814 (51.1) | ||
| 3 |
767 (5.2) |
477 (4.7) |
290 (6.1) |
211 (5.9) |
196 (5.5) | ||
| NA |
365 (2.5) |
189 (1.9) |
176 (3.7) |
120 (3.4) |
131 (3.7) | ||
| NX |
151 (1.0) |
86 (0.8) |
65 (1.4) |
50 (1.4) |
42 (1.2) | ||
| M stage | < 0.001 | > 0.05 | |||||
| 0 |
13,894 (93.5) |
9643 (95.2) |
4251 (89.9) |
3242 (91.3) |
3240 (91.3) | ||
| 1 |
596 (4.0) |
296 (2.9) |
300 (6.3) |
188 (5.3) |
179 (5.0) | ||
| NA |
365 (2.5) |
189 (1.9) |
176 (3.7) |
120 (3.4) |
131 (3.7) | ||
| Categories | Originated site |
| ||||||
|---|---|---|---|---|---|---|---|---|
| Tonsil | Gum and other mouth | Hypopharynx | Nasopharynx | Oropharynx | Other oral cavity and pharynx | Tongue | ||
| All cases | 6650 | 307 | 811 | 890 | 955 | 307 | 4935 | |
| HPV status | < 0.001 | |||||||
| Positive |
5213 (78.4) |
64 (20.8) |
204 (25.2) |
285 (32) |
543 (56.9) |
157 (51.1) |
3662 (74.2) | |
| Sex | ||||||||
| Male |
5568 (83.7) |
202 (65.8) |
660 (81.4) |
627 (70.4) |
770 (80.6) |
255 (83.1) |
4282 (86.8) | < 0.001 |
| Age | ||||||||
| Mean (SD) |
52.72 (9.57) |
56.57 (10.82) |
57.2 (10.06) |
48 (14.27) |
54.84 (10.19) |
55.26 (10.44) |
55.68 (9.66) | < 0.001 |
| 0–45 |
1452 (21.8) |
42 (13.7) |
86 (10.6) |
352 (39.6) |
147 (15.4) |
44 (14.3) |
656 (13.3) | < 0.001 |
| 46–60 |
3907 (58.8) |
165 (53.7) |
430 (53.0) |
377 (42.4) |
546 (57.2) |
176 (57.3) |
2878 (58.3) | |
| 61–75 |
1180 (17.7) |
83 (27) |
261 (32.2) |
144 (16.2) |
233 (24.4) |
77 (25.1) |
1258 (25.5) | |
| 75+ |
111 (1.7) |
17 (5.5) |
34 (4.2) |
17 (1.9) |
29 (3.0) |
10 (3.3) |
143 (2.9) | |
| Race | < 0.001 | |||||||
| White |
5846 (87.9) |
237 (77.2) |
640 (78.9) |
421 (47.3) |
793 (83) |
277 (90.2) |
4468 (90.5) | |
| AI |
45 (0.7) |
1 (0.3) |
12 (1.5) |
21 (2.4) |
8 (0.8) |
1 (0.3) |
33 (0.7) | |
| API |
208 (3.1) |
12 (3.9) |
53 (6.5) |
335 (37.6) |
28 (2.9) |
6 (2) |
118 (2.4) | |
| AA |
494 (7.4) |
53 (17.3) |
106 (13.1) |
101 (11.3) |
117 (12.3) |
23 (7.5) |
295 (6) | |
| Unknown |
57 (0.9) |
4 (1.3) |
0 (0) |
12 (1.3) |
9 (0.9) |
0 (0) |
21 (0.4) | |
| Year of diagnosis | 0.062 | |||||||
| 2010 |
428 (6.4) |
16 (5.2) |
46 (5.7) |
57 (6.4) |
57 (6) |
15 (4.9) |
282 (5.7) | |
| 2011 |
642 (9.7) |
23 (7.5) |
69 (8.5) |
99 (11.1) |
82 (8.6) |
36 (11.7) |
463 (9.4) | |
| 2012 |
819 (12.3) |
41 (13.4) |
113 (13.9) |
99 (11.1) |
97 (10.2) |
23 (7.5) |
596 (12.1) | |
| 2013 |
1027 (15.4) |
44 (14.3) |
123 (15.2) |
137 (15.4) |
148 (15.5) |
47 (15.3) |
714 (14.5) | |
| 2014 |
1153 (17.3) |
60 (19.5) |
137 (16.9) |
116 (13) |
180 (18.8) |
57 (18.6) |
882 (17.9) | |
| 2015 |
1215 (18.3) |
58 (18.9) |
140 (17.3) |
185 (20.8) |
173 (18.1) |
50 (16.3) |
944 (19.1) | |
| 2016 |
1366 (20.5) |
65 (21.2) |
183 (22.6) |
197 (22.1) |
218 (22.8) |
79 (25.7) |
1054 (21.4) | |
| Differentiation | < 0.001 | |||||||
| Grade I |
182 (2.7) |
30 (9.8) |
30 (3.7) |
10 (1.1) |
44 (4.6) |
10 (3.3) |
146 (3) | |
| Grade II |
2004 (30.1) |
137 (44.6) |
311 (38.3) |
74 (8.3) |
308 (32.3) |
68 (22.1) |
1352 (27.4) | |
| Grade III |
2960 (44.5) |
85 (27.7) |
285 (35.1) |
311 (34.9) |
294 (30.8) |
55 (17.9) |
2043 (41.4) | |
| Grade IV |
80 (1.2) |
3 (1) |
8 (1) |
209 (23.5) |
11 (1.2) |
2 (0.7) |
57 (1.2) | |
| Unknown |
1424 (21.4) |
52 (16.9) |
177 (21.8) |
286 (32.1) |
298 (31.2) |
172 (56) |
1337 (27.1) | |
| Surgery | < 0.001 | |||||||
| Surgery |
3241 (48.7) |
124 (40.4) |
153 (18.9) |
83 (9.3) |
249 (26.1) |
53 (17.3) |
1144 (23.2) | |
| Tumor destruction |
4 (0.1) |
1 (0.3) |
1 (0.1) |
0 (0) |
0 (0.0) |
1 (0.3) |
3 (0.1) | |
| No |
3392 (51.0) |
179 (58.3) |
655 (80.8) |
807 (90.7) |
704 (73.7) |
250 (81.4) |
3778 (76.6) | |
| Unknown |
13 (0.2) |
3 (1) |
2 (0.2) |
0 (0) |
2 (0.2) |
3 (1.0) |
10 (0.2) | |
| Radiotherapy | < 0.001 | |||||||
| Yes |
5738 (86.3) |
201 (65.5) |
657 (81) |
782 (87.9) |
775 (81.2) |
231 (75.2) |
4301 (87.2) | |
| Refused |
66 (1) |
6 (2) |
9 (1.1) |
5 (0.6) |
16 (1.7) |
1 (0.3) |
73 (1.5) | |
| Unknown |
846 (12.7) |
100 (32.6) |
145 (17.9) |
103 (11.6) |
164 (17.2) |
75 (24.4) |
561 (11.4) | |
| Chemotherapy | < 0.001 | |||||||
| No/unknown |
2051 (30.8) |
168 (54.7) |
229 (28.2) |
136 (15.3) |
296 (31) |
136 (44.3) |
1279 (25.9) | |
| Insurance | < 0.001 | |||||||
| Insured |
6274 (94.3) |
286 (93.2) |
763 (94.1) |
829 (93.1) |
883 (92.5) |
286 (93.2) |
4728 (95.8) | |
| Uninsured |
237 (3.6) |
12 (3.9) |
35 (4.3) |
45 (5.1) |
49 (5.1) |
14 (4.6) |
137 (2.8) | |
| Unknown |
139 (2.1) |
9 (2.9) |
13 (1.6) |
16 (1.8) |
23 (2.4) |
7 (2.3) |
70 (1.4) | |
| Marriage | < 0.001 | |||||||
| Married |
3903 (58.7) |
130 (42.3) |
355 (43.8) |
508 (57.1) |
454 (47.5) |
160 (52.1) |
3029 (61.4) | |
| Unmarried |
2394 (36) |
152 (49.5) |
403 (49.7) |
336 (37.8) |
434 (45.4) |
132 (43) |
1693 (34.3) | |
| Unknown |
353 (5.3) |
25 (8.1) |
53 (6.5) |
46 (5.2) |
67 (7) |
15 (4.9) |
213 (4.3) | |
| Lung metastasis | < 0.001 | |||||||
| NA |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
2 (0.7) |
0 (0) | |
| No |
6511 (97.9) |
295 (96.1) |
769 (94.8) |
841 (94.5) |
908 (95.1) |
286 (93.2) |
4795 (97.2) | |
| Unknown |
59 (0.9) |
5 (1.6) |
9 (1.1) |
15 (1.7) |
16 (1.7) |
14 (4.6) |
44 (0.9) | |
| Yes |
80 (1.2) |
7 (2.3) |
33 (4.1) |
34 (3.8) |
31 (3.2) |
5 (1.6) |
96 (1.9) | |
| Brain metastasis | < 0.001 | |||||||
| NA |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
2 (0.7) |
0 (0) | |
| No |
6585 (99) |
302 (98.4) |
799 (98.5) |
868 (97.5) |
937 (98.1) |
289 (94.1) |
4901 (99.3) | |
| Unknown |
56 (0.8) |
5 (1.6) |
10 (1.2) |
12 (1.3) |
15 (1.6) |
14 (4.6) |
32 (0.6) | |
| Yes |
9 (0.1) |
0 (0) |
2 (0.2) |
10 (1.1) |
3 (0.3) |
2 (0.7) |
2 (0) | |
| Liver metastasis | < 0.001 | |||||||
| NA |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
2 (0.7) |
0 (0) | |
| No |
6566 (98.7) |
299 (97.4) |
793 (97.8) |
851 (95.6) |
929 (97.3) |
286 (93.2) |
4867 (98.6) | |
| Unknown |
56 (0.8) |
4 (1.3) |
9 (1.1) |
11 (1.2) |
15 (1.6) |
13 (4.2) |
32 (0.6) | |
| Yes |
28 (0.4) |
4 (1.3) |
9 (1.1) |
28 (3.1) |
11 (1.2) |
6 (2) |
36 (0.7) | |
| Bone metastasis | < 0.001 | |||||||
| NA |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
3 (1) |
0 (0) | |
| No |
6535 (98.3) |
301 (98) |
784 (96.7) |
831 (93.4) |
929 (97.3) |
283 (92.2) |
4849 (98.3) | |
| Unknown |
56 (0.8) |
4 (1.3) |
16 (2) |
46 (5.2) |
14 (1.5) |
15 (4.9) |
30 (0.6) | |
| Yes |
59 (0.9) |
2 (0.7) |
11 (1.4) |
13 (1.5) |
12 (1.3) |
6 (2) |
56 (1.1) | |
| T stage | < 0.001 | |||||||
| 0 |
5 (0.1) |
0 (0) |
1 (0.1) |
6 (0.7) |
42 (4.4) |
0 (0) |
10 (0.2) | |
| 1 |
1774 (26.7) |
92 (30) |
79 (9.7) |
267 (30) |
137 (14.3) |
0 (0) |
1153 (23.4) | |
| 2 |
2522 (37.9) |
86 (28) |
262 (32.3) |
166 (18.7) |
183 (19.2) |
0 (0) |
1625 (32.9) | |
| 3 |
989 (14.9) |
49 (16) |
184 (22.7) |
181 (20.3) |
176 (18.4) |
0 (0) |
894 (18.1) | |
| 4 |
787 (11.8) |
54 (17.6) |
209 (25.8) |
222 (24.9) |
261 (27.3) |
0 (0) |
787 (15.9) | |
| NA |
20 (0.3) |
4 (1.3) |
3 (0.4) |
10 (1.1) |
6 (0.6) |
307 (100) |
15 (0.3) | |
| TX |
553 (8.3) |
22 (7.2) |
73 (9) |
38 (4.3) |
150 (15.7) |
0 (0) |
451 (9.1) | |
| N stage | < 0.001 | |||||||
| 0 |
1029 (15.5) |
149 (48.5) |
204 (25.2) |
178 (20) |
180 (18.8) |
0 (0) |
626 (12.7) | |
| 1 |
1239 (18.6) |
43 (14) |
135 (16.6) |
296 (33.3) |
157 (16.4) |
0 (0) |
831 (16.8) | |
| 2 |
3981 (59.9) |
96 (31.3) |
411 (50.7) |
273 (30.7) |
547 (57.3) |
0 (0) |
3197 (64.8) | |
| 3 |
306 (4.6) |
11 (3.6) |
48 (5.9) |
120 (13.5) |
53 (5.5) |
0 (0) |
229 (4.6) | |
| NA |
20 (0.3) |
4 (1.3) |
3 (0.4) |
10 (1.1) |
6 (0.6) |
307 (100) |
15 (0.3) | |
| NX |
75 (1.1) |
4 (1.3) |
10 (1.2) |
13 (1.5) |
12 (1.3) |
0 (0) |
37 (0.7) | |
| M stage | < 0.001 | |||||||
| 0 |
6436 (96.8) |
288 (93.8) |
753 (92.8) |
792 (89) |
895 (93.7) |
0 (0) |
4730 (95.8) | |
| 1 |
194 (2.9) |
15 (4.9) |
55 (6.8) |
88 (9.9) |
54 (5.7) |
0 (0) |
190 (3.9) | |
| NA |
20 (0.3) |
4 (1.3) |
3 (0.4) |
10 (1.1) |
6 (0.6) |
307 (100) |
15 (0.3) | |
| Categories | Bone metastasis | Brain metastasis | Liver metastasis | Lung metastasis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes |
| No | Yes |
| No | Yes |
| No | Yes |
| |
|
|
14,512 (98.66) |
197 (1.34) |
14,681 (99.81) |
28 (0.19) |
14,591 (99.17) |
122 (0.83) |
14,405 (98.05) |
286 (1.95) | ||||
| Sex | 0.505 | 0.922 | 1 | 0.031 | ||||||||
| Male |
12,083 (98.69) |
160 (1.31) |
12,219 (99.8) |
24 (0.2) |
12,144 (99.17) |
102 (0.83) |
12,002 (98.17) |
224 (1.83) | ||||
| Female |
2429 (98.5) |
37 (1.5) |
2462 (99.84) |
4 (0.16) |
2447 (99.19) |
20 (0.81) |
2403 (97.48) |
62 (2.52) | ||||
| Age | ||||||||||||
| Mean (SD) |
53.92 (10.22) |
53.23 (12.76) | 0.088 |
53.92 (10.26) |
49.86 (11.27) | 0.008 |
53.91 (10.26) |
53.80 (10.28) | 0.032 |
53.88 (10.25) |
55.28 (10.50) | < 0.001 |
| Age group | 0.002 | 0.005 | 0.008 | < 0.001 | ||||||||
| 0–45 |
2716 (98.55) |
40 (1.45) |
2751 (99.82) |
5 (0.18) |
2737 (99.2) |
22 (0.8) |
2715 (98.55) |
40 (1.45) | ||||
| 46–60 |
8310 (98.85) |
97 (1.15) |
8388 (99.76) |
20 (0.24) |
8334 (99.12) |
74 (0.88) |
8232 (98.02) |
166 (1.98) | ||||
| 61–75 |
3139 (98.25) |
56 (1.75) |
3191 (99.91) |
3 (0.09) |
3171 (99.25) |
24 (0.75) |
3119 (97.74) |
72 (2.26) | ||||
| 75+ |
347 (98.86) |
4 (1.14) |
351 (100) |
0 (0) |
349 (99.43) |
2 (0.57) |
339 (97.69) |
8 (2.31) | ||||
| Race | < 0.001 | 0.037 | < 0.001 | < 0.001 | ||||||||
| White |
12,435 (98.89) |
140 (1.11) |
12,553 (99.83) |
22 (0.17) |
12,487 (99.28) |
90 (0.72) |
12,347 (98.31) |
212 (1.69) | ||||
| AI |
118 (98.33) |
2 (1.67) |
120 (100) |
0 (0) |
119 (99.17) |
1 (0.83) |
118 (98.33) |
2 (1.67) | ||||
| API |
724 (96.66) |
25 (3.34) |
744 (99.33) |
5 (0.67) |
731 (97.34) |
20 (2.66) |
719 (96.12) |
29 (3.88) | ||||
| AA |
1150 (97.62) |
28 (2.38) |
1177 (99.92) |
1 (0.08) |
1167 (99.07) |
11 (0.93) |
1135 (96.43) |
42 (3.57) | ||||
| Unknown |
85 (97.7) |
2 (2.3) |
87 (100) |
0 (0) |
87 (100) |
0 (0) |
86 (98.85) |
1 (1.15) | ||||
| Year of Dx | 0.431 | 0.659 | 0.015 | 0.946 | ||||||||
| 2010 |
887 (99.11) |
8 (0.89) |
893 (99.78) |
2 (0.22) |
890 (99.44) |
5 (0.56) |
877 (97.99) |
18 (2.01) | ||||
| 2011 |
1374 (98.57) |
20 (1.43) |
1389 (99.64) |
5 (0.36) |
1381 (99.07) |
13 (0.93) |
1366 (98.13) |
26 (1.87) | ||||
| 2012 |
1748 (98.7) |
23 (1.3) |
1766 (99.77) |
4 (0.23) |
1760 (99.38) |
11 (0.62) |
1729 (97.85) |
38 (2.15) | ||||
| 2013 |
2186 (98.51) |
33 (1.49) |
2213 (99.82) |
4 (0.18) |
2206 (99.41) |
13 (0.59) |
2169 (97.83) |
48 (2.17) | ||||
| 2014 |
2529 (98.56) |
37 (1.44) |
2564 (99.88) |
3 (0.12) |
2544 (99.14) |
22 (0.86) |
2518 (98.21) |
46 (1.79) | ||||
| 2015 |
2718 (99.02) |
27 (0.98) |
2743 (99.89) |
3 (0.11) |
2732 (99.42) |
16 (0.58) |
2685 (98.03) |
54 (1.97) | ||||
| 2016 |
3070 (98.43) |
49 (1.57) |
3113 (99.78) |
7 (0.22) |
3078 (98.65) |
42 (1.35) |
3061 (98.2) |
56 (1.8) | ||||
| Site | < 0.001 | < 0.001 | < 0.001 | < 0.001 | ||||||||
| Gum and other mouth |
301 (99.34) |
2 (0.66) |
302 (100) |
0 (0) |
299 (98.68) |
4 (1.32) |
295 (97.68) |
7 (2.32) | ||||
| Hypopharynx |
784 (98) |
16 (2) |
799 (99.75) |
2 (0.25) |
793 (98.88) |
9 (1.12) |
769 (95.89) |
33 (4.11) | ||||
| Nasopharynx |
831 (94.75) |
46 (5.25) |
868 (98.86) |
10 (1.14) |
851 (96.81) |
28 (3.19) |
841 (96.11) |
34 (3.89) | ||||
| Oropharynx |
929 (98.72) |
12 (1.28) |
937 (99.68) |
3 (0.32) |
929 (98.83) |
11 (1.17) |
908 (96.7) |
31 (3.3) | ||||
| Other oral cavity and pharynx |
283 (97.92) |
6 (2.08) |
289 (99.31) |
2 (0.69) |
286 (97.95) |
6 (2.05) |
286 (98.28) |
5 (1.72) | ||||
| Tongue |
4849 (98.86) |
56 (1.14) |
4901 (99.96) |
2 (0.04) |
4867 (99.27) |
36 (0.73) |
4795 (98.04) |
96 (1.96) | ||||
| Tonsil |
6535 (99.11) |
59 (0.89) |
6585 (99.86) |
9 (0.14) |
6566 (99.58) |
28 (0.42) |
6511 (98.79) |
80 (1.21) | ||||
| Grade | < 0.001 | 0.132 | < 0.001 | 0.264 | ||||||||
| Grade I |
447 (99.78) |
1 (0.22) |
449 (100) |
0 (0) |
449 (100) |
0 (0) |
444 (99.11) |
4 (0.89) | ||||
| Grade II |
4170 (99.12) |
37 (0.88) |
4206 (99.9) |
4 (0.1) |
4193 (99.55) |
19 (0.45) |
4117 (98.02) |
83 (1.98) | ||||
| Grade III |
5902 (98.7) |
78 (1.3) |
5964 (99.8) |
12 (0.2) |
5925 (99.16) |
50 (0.84) |
5866 (98.19) |
108 (1.81) | ||||
| Grade IV |
352 (96.17) |
14 (3.83) |
366 (100) |
0 (0) |
358 (97.81) |
8 (2.19) |
358 (98.08) |
7 (1.92) | ||||
| Unknown |
3641 (98.19) |
67 (1.81) |
3696 (99.68) |
12 (0.32) |
3666 (98.79) |
45 (1.21) |
3620 (97.73) |
84 (2.27) | ||||
| Surgery | < 0.001 | 0.17 | < 0.001 | < 0.001 | ||||||||
| Surgery |
5005 (99.6) |
20 (0.4) |
5020 (99.92) |
4 (0.08) |
5017 (99.82) |
9 (0.18) |
4994 (99.42) |
29 (0.58) | ||||
| Tumor destruction |
10 (100) |
0 (0) |
10 (100) |
0 (0) |
10 (100) |
0 (0) |
10 (100) |
0 (0) | ||||
| No |
9475 (98.17) |
177 (1.83) |
9629 (99.75) |
24 (0.25) |
9543 (98.84) |
112 (1.16) |
9379 (97.33) |
257 (2.67) | ||||
| Unknown |
22 (100) |
0 (0) |
22 (100) |
0 (0) |
21 (95.45) |
1 (4.55) |
22 (100) |
0 (0) | ||||
| Radiation | < 0.001 | < 0.001 | < 0.001 | < 0.001 | ||||||||
| Yes |
12,499 (99.08) |
116 (0.92) |
12,599 (99.87) |
16 (0.13) |
12,561 (99.56) |
56 (0.44) |
12,442 (98.73) |
160 (1.27) | ||||
| Refused |
169 (98.26) |
3 (1.74) |
173 (100) |
0 (0) |
171 (99.42) |
1 (0.58) |
167 (97.66) |
4 (2.34) | ||||
| Unknown |
1844 (95.94) |
78 (4.06) |
1909 (99.38) |
12 (0.62) |
1859 (96.62) |
65 (3.38) |
1796 (93.64) |
122 (6.36) | ||||
| Chemotherapy | 0.444 | 0.296 | 0.092 | 0.487 | ||||||||
| Yes |
10,358 (98.61) |
146 (1.39) |
10,487 (99.84) |
17 (0.16) |
10,411 (99.09) |
96 (0.91) |
10,281 (98) |
210 (2) | ||||
| No |
4154 (98.79) |
51 (1.21) |
4194 (99.74) |
11 (0.26) |
4180 (99.38) |
26 (0.62) |
4124 (98.19) |
76 (1.81) | ||||
| Insurance | 0.485 | 0.457 | 0.318 | 0.081 | ||||||||
| Insured |
13,750 (98.69) |
183 (1.31) |
13,904 (99.8) |
28 (0.2) |
13,822 (99.17) |
115 (0.83) |
13,652 (98.11) |
263 (1.89) | ||||
| Uninsured |
517 (98.1) |
10 (1.9) |
528 (100) |
0 (0) |
525 (99.43) |
3 (0.57) |
510 (96.77) |
17 (3.23) | ||||
| Unknown |
245 (98.39) |
4 (1.61) |
249 (100) |
0 (0) |
244 (98.39) |
4 (1.61) |
243 (97.59) |
6 (2.41) | ||||
| Marriage | < 0.001 | 0.142 | 0.204 | < 0.001 | ||||||||
| Married |
8399 (99.01) |
84 (0.99) |
8476 (99.87) |
11 (0.13) |
8425 (99.27) |
62 (0.73) |
8349 (98.55) |
123 (1.45) | ||||
| Unmarried |
5385 (98.07) |
106 (1.93) |
5474 (99.73) |
15 (0.27) |
5438 (99) |
55 (1) |
5339 (97.3) |
148 (2.7) | ||||
| Unknown |
728 (99.05) |
7 (0.95) |
731 (99.73) |
2 (0.27) |
728 (99.32) |
5 (0.68) |
717 (97.95) |
15 (2.05) | ||||
| T stage | < 0.001 | < 0.001 | < 0.001 | < 0.001 | ||||||||
| 0 |
62 (96.88) |
2 (3.13) |
62 (96.88) |
2 (3.13) |
63 (98.44) |
1 (1.56) |
63 (98.44) |
1 (1.56) | ||||
| 1 |
3467 (99.31) |
24 (0.69) |
3489 (99.97) |
1 (0.03) |
3474 (99.46) |
19 (0.54) |
3468 (99.4) |
21 (0.6) | ||||
| 2 |
4783 (99.25) |
36 (0.75) |
4814 (99.92) |
4 (0.08) |
4791 (99.46) |
26 (0.54) |
4763 (98.9) |
53 (1.1) | ||||
| 3 |
2434 (98.62) |
34 (1.38) |
2462 (99.84) |
4 (0.16) |
2447 (99.07) |
23 (0.93) |
2381 (96.75) |
80 (3.25) | ||||
| 4 |
2247 (97.36) |
61 (2.64) |
2302 (99.65) |
8 (0.35) |
2280 (98.74) |
29 (1.26) |
2215 (96.26) |
86 (3.74) | ||||
| NA |
331 (97.93) |
7 (2.07) |
338 (99.41) |
2 (0.59) |
333 (97.94) |
7 (2.06) |
335 (98.53) |
5 (1.47) | ||||
| TX |
1188 (97.3) |
33 (2.7) |
1214 (99.43) |
7 (0.57) |
1203 (98.61) |
17 (1.39) |
1180 (96.72) |
40 (3.28) | ||||
| N stage | < 0.001 | < 0.001 | < 0.001 | < 0.001 | ||||||||
| 0 |
2341 (99.36) |
15 (0.64) |
2353 (99.83) |
4 (0.17) |
2350 (99.75) |
6 (0.25) |
2333 (99.19) |
19 (0.81) | ||||
| 1 |
2645 (98.55) |
39 (1.45) |
2671 (99.63) |
10 (0.37) |
2666 (99.37) |
17 (0.63) |
2640 (98.43) |
42 (1.57) | ||||
| 2 |
8366 (98.75) |
106 (1.25) |
8462 (99.88) |
10 (0.12) |
8405 (99.19) |
69 (0.81) |
8289 (97.96) |
173 (2.04) | ||||
| 3 |
733 (96.19) |
29 (3.81) |
762 (100) |
0 (0) |
745 (97.51) |
19 (2.49) |
717 (94.22) |
44 (5.78) | ||||
| NA |
331 (97.93) |
7 (2.07) |
338 (99.41) |
2 (0.59) |
333 (97.94) |
7 (2.06) |
335 (98.53) |
5 (1.47) | ||||
| NX |
96 (98.97) |
1 (1.03) |
95 (97.94) |
2 (2.06) |
92 (95.83) |
4 (4.17) |
91 (96.81) |
3 (3.19) | ||||
| Categories | Number | HR (95% CI) |
|
|---|---|---|---|
| All cases | 14,855 | ||
| Sex | |||
| Female | 2491 | Reference | |
| Male | 164 | 1.00 (0.91–1.09) | > 0.05 |
| Race | |||
| White | 12,682 | Reference | |
| AI | 121 | 1.24 (0.88–1.88) | > 0.05 |
| API | 760 | 0.87 (0.73–1.04) | > 0.05 |
| AA | 1189 | 1.25 (1.16–1.40) | < 0.0001 |
| Unknown | 103 | 0.23 (0.10–0.57) | < 0.001 |
| Age group | |||
| 0–44 | 2779 | Reference | |
| 45–59 | 8479 | 1.39 (1.25–1.56) | < 0.0001 |
| 60–75 | 3236 | 2.26 (2.00–2.56) | < 0.0001 |
| 75+ | 361 | 4.15 (3.46–4.98) | < 0.0001 |
| Year of diagnosis | |||
| 2010 | 901 | Reference | |
| 2011 | 1414 | 1.09 (0.94–1.28) | > 0.05 |
| 2012 | 1788 | 1.19 (1.02–1.39) | < 0.01 |
| 2013 | 2240 | 1.35 (1.16–1.57) | < 0.0001 |
| 2014 | 2585 | 1.31 (1.13–1.53) | < 0.0001 |
| 2015 | 2765 | 1.31 (1.11–1.54) | < 0.001 |
| 2016 | 3162 | 1.04 (0.85–1.28) | > 0.05 |
| Site | |||
| Tonsil | 6650 | Reference | |
| Gum and other mouth | 307 | 0.99 (0.80–1.23) | > 0.05 |
| Hypopharynx | 811 | 1.36 (1.19–1.55) | < 0.0001 |
| Nasopharynx | 890 | 0.98 (0.82–1.17) | > 0.05 |
| Oropharynx | 955 | 1.40 (1.23–1.60) | < 0.0001 |
| Other oral cavity and pharynx | 307 | 1.33 (0.49–3.67) | > 0.05 |
| Tongue | 4935 | 1.01 (0.92–1.10) | > 0.05 |
| Tonsil | 6650 | Reference | |
| Differentiation | |||
| Grade I | 452 | Reference | |
| Grade II | 4254 | 1.08 (0.89–1.31) | > 0.05 |
| Grade III | 6033 | 0.81 (0.67–0.99) | < 0.01 |
| Grade IV | 370 | 0.71 (0.52–0.99) | < 0.01 |
| Unknown | 3746 | 0.86 (0.70–1.05) | > 0.05 |
| Surgery | |||
| Surgery | 5047 | Reference | |
| Tumor destruction | 10 | 2.82 (0.70–11.33) | > 0.05 |
| NO | 9765 | 1.92 (1.74–2.12) | < 0.0001 |
| Unknown | 33 | 2.46 (1.25–4.86) | < 0.001 |
| Radiotherapy | |||
| Yes | 12,685 | Reference | |
| Refused | 176 | 3.76 (2.98–4.73) | < 0.0001 |
| Unknown | 1994 | 2.33 (2.12–2.57) | < 0.0001 |
| Chemotherapy | |||
| Yes | 10,560 | Reference | |
| No | 4295 | 1.46 (1.33–1.60) | < 0.0001 |
| Insurance | |||
| Insured | 14,049 | Reference | |
| Uninsured | 529 | 1.33 (1.14–1.55) | < 0.0001 |
| Unknown | 277 | 0.92 (0.71–1.18) | > 0.05 |
| Marriage | |||
| Married | 8539 | Reference | |
| Unmarried | 5544 | 1.60 (1.48–1.73) | < 0.0001 |
| Unknown | 772 | 1.20 (1.02–1.41) | < 0.01 |
| Lung metastasis | |||
| No | 14,405 | Reference | |
| Yes | 286 | 1.53 (1.23–1.91) | < 0.0001 |
| NA | 2 | 149,055.48 (0.00–0.00) | > 0.05 |
| Unknown | 162 | 1.64 (0.92–2.90) | > 0.05 |
| Brain metastasis | |||
| No | 14,681 | Reference | |
| Yes | 28 | 2.71 (1.70–4.30) | < 0.0001 |
| NA | 2 | NA | > 0.05 |
| Unknown | 144 | 2.37 (0.77–7.27) | > 0.05 |
| Liver metastasis | |||
| No | 14,591 | Reference | |
| Yes | 122 | 1.34 (1.02–1.75) | < 0.01 |
| NA | 2 | NA | > 0.05 |
| Unknown | 140 | 0.13 (0.04–0.41) | < 0.0001 |
| Bone metastasis | |||
| No | 14,512 | Reference | |
| Yes | 197 | 1.52 (1.20–1.92) | < 0.0001 |
| NA | 3 | 0.00 (0.00–0.00) | > 0.05 |
| Unknown | 143 | 2.40 (1.03–5.58) | < 0.01 |
| T stage | |||
| 0 | 64 | Reference | |
| 1 | 3502 | 0.99 (0.55–1.79) | > 0.05 |
| 2 | 4844 | 1.45 (0.81–2.60) | > 0.05 |
| 3 | 2473 | 2.29 (1.28–4.11) | < 0.001 |
| 4 | 20 | 3.38 (1.89–6.06) | < 0.0001 |
| NA | 365 | 1.96 (0.62–6.17) | > 0.05 |
| TX | 1287 | 1.50 (0.83–2.70) | > 0.05 |
| N stage | |||
| 0 | 66 | Reference | |
| 1 | 2701 | 1.33 (1.17–1.51) | < 0.0001 |
| 2 | 8505 | 1.51 (1.35–1.68) | < 0.0001 |
| 3 | 767 | 2.17 (1.85–2.55) | < 0.0001 |
| NA | 365 | NA | > 0.05 |
| NX | 151 | 1.21 (0.83–1.74) | > 0.05 |
| M stage | |||
| 0 | 13,894 | Reference | |
| 1 | 596 | 1.79 (1.46–2.20) | < 0.0001 |
| NA | 365 | NA | > 0.05 |
| HPV status | |||
| Negative | 4727 | Reference | |
| Positive | 10,128 | 0.50 (0.46–0.54) | < 0.0001 |
| Categories | Number | HR (95% CI) |
|
|---|---|---|---|
| Sex | |||
| Female | 1466 | 0.52 (0.42–0.63) | < 0.001 |
| Male | 5634 | 0.60 (0.54–0.66) | < 0.001 |
| Age | |||
| 0–45 | 1335 | 0.53 (0.41–0.68) | < 0.001 |
| 46–60 | 3830 | 0.54 (0.47–0.62) | < 0.001 |
| 61–75 | 1723 | 0.62 (0.53–0.74) | < 0.001 |
| 75+ | 212 | 0.83 (0.58–1.20) | > 0.05 |
| Race | |||
| White | 5799 | 0.58 (0.52–0.64) | < 0.001 |
| AI | 70 | 0.65 (0.25–1.72) | > 0.05 |
| API | 430 | 0.55 (0.36–0.84) | < 0.01 |
| AA | 750 | 0.55 (0.43–0.71) | < 0.001 |
| Unknown | 51 | 1.05 (0.07–16.87) | > 0.05 |
| Year of diagnosis | |||
| 2010 | 516 | 0.64 (0.48–0.86) | < 0.001 |
| 2011 | 813 | 0.60 (0.48–0.77) | < 0.001 |
| 2012 | 944 | 0.54 (0.43–0.67) | < 0.001 |
| 2013 | 1096 | 0.59 (0.48–0.73) | < 0.001 |
| 2014 | 1194 | 0.54 (0.44–0.67) | < 0.001 |
| 2015 | 1176 | 0.68 (0.52–0.87) | < 0.001 |
| 2016 | 1361 | 0.45 (0.31–0.67) | < 0.001 |
| Site | |||
| Gum and other mouth | 148 | 0.84 (0.43–1.64) | > 0.05 |
| Hypopharynx | 425 | 0.66 (0.47–0.93) | < 0.05 |
| Nasopharynx | 556 | 1.22 (0.85–1.75) | > 0.05 |
| Oropharynx | 632 | 0.69 (0.53–0.91) | < 0.01 |
| Other oral cavity and pharynx | 216 | 0.37 (0.21–0.66) | < 0.001 |
| Tongue | 2319 | 0.55 (0.47–0.64) | < 0.001 |
| Tonsil | 2804 | 0.50 (0.42–0.58) | < 0.001 |
| Differentiation | |||
| Grade I | 295 | 0.53 (0.32–0.87) | < 0.05 |
| Grade II | 2378 | 0.53 (0.45–0.62) | < 0.001 |
| Grade III | 2582 | 0.64 (0.54–0.75) | < 0.001 |
| Grade IV | 205 | 0.82 (0.44–1.53) | > 0.05 |
| Unknown | 1640 | 0.57 (0.47–0.69) | < 0.001 |
| Surgery | |||
| Surgery | 2177 | 0.54 (0.43–0.67) | < 0.001 |
| Tumor destruction | 9 | 1.00 (0.06–15.99) | > 0.05 |
| NO | 4892 | 0.59 (0.53–0.65) | < 0.001 |
| Unknown | 22 | 0.87 (0.12–6.21) | > 0.05 |
| Radiotherapy | |||
| Yes | 5829 | 0.54 (0.49–0.61) | < 0.001 |
| Refused | 96 | 0.43 (0.25–0.75) | < 0.01 |
| Unknown | 1175 | 0.65 (0.54–0.78) | < 0.001 |
| Chemotherapy | |||
| Yes | 4906 | 0.59 (0.53–0.66) | < 0.001 |
| No | 2194 | 0.55 (0.47–0.65) | < 0.001 |
| Insurance | |||
| Insured | 6612 | 0.59 (0.53–0.65) | < 0.001 |
| Uninsured | 318 | 0.46 (0.24–0.85) | < 0.001 |
| Unknown | 170 | 0.54 (0.38–0.77) | < 0.05 |
| Marriage | |||
| Married | 3656 | 0.57 (0.49–0.66) | < 0.001 |
| Unmarried | 3021 | 0.54 (0.48–0.61) | < 0.001 |
| Unknown | 423 | 0.73 (0.50–1.07) | > 0.05 |
| Lung metastasis | |||
| NA | 1 | 0.79 (0.55–1.13) | > 0.05 |
| No | 6822 | 0.56 (0.51–0.62) | < 0.001 |
| Unknown | 104 | 0.67 (0.35–1.30) | > 0.05 |
| Yes | 173 | 0.79 (0.55–1.13) | > 0.05 |
| Brain metastasis | |||
| NA | 1 | 1.35 (0.45–4.01) | > 0.05 |
| No | 6983 | 0.58 (0.53–0.63) | < 0.001 |
| Unknown | 95 | 0.72 (0.36–1.45) | > 0.05 |
| Yes | 21 | 1.35 (0.45–4.01) | > 0.05 |
| Liver metastasis | |||
| NA | 1 | 0.90 (0.50–1.59) | > 0.05 |
| No | 6932 | 0.57 (0.52–0.63) | < 0.001 |
| Unknown | 90 | 0.60 (0.28–1.28) | > 0.05 |
| Yes | 77 | 0.90 (0.50–1.59) | > 0.05 |
| Bone metastasis | |||
| NA | 1 | 0.80 (0.52–1.22) | > 0.05 |
| No | 6882 | 0.58 (0.52–0.63) | < 0.001 |
| Unknown | 93 | 0.64 (0.31–1.32) | > 0.05 |
| Yes | 124 | 0.80 (0.52–1.22) | > 0.05 |
| T stage | |||
| 0 | 26 | 1.25 (0.23–6.86) | > 0.05 |
| 1 | 1437 | 0.63 (0.47–0.84) | < 0.01 |
| 2 | 2031 | 0.48 (0.39–0.60) | < 0.001 |
| 3 | 1313 | 0.54 (0.44–0.65) | < 0.001 |
| 4 | 1351 | 0.67 (0.57–0.78) | < 0.001 |
| NA | 251 | 0.38 (0.21–0.67) | < 0.001 |
| TX | 691 | 0.50 (0.37–0.68) | < 0.001 |
| N stage | |||
| 0 | 1347 | 0.54 (0.42–0.69) | < 0.001 |
| 1 | 1461 | 0.61 (0.49–0.76) | < 0.001 |
| 2 | 3542 | 0.60 (0.53–0.68) | < 0.001 |
| 3 | 407 | 0.57 (0.41–0.80) | < 0.001 |
| NA | 251 | 0.38 (0.21–0.67) | < 0.001 |
| NX | 92 | 0.82 (0.38–1.76) | > 0.05 |
| M stage | |||
| 0 | 6482 | 0.56 (0.50–0.62) | < 0.001 |
| 1 | 367 | 0.74 (0.58–0.96) | < 0.05 |
| NA | 251 | 0.38 (0.21–0.67) | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Cervical Cancer and HPV Research · Biological Research and Disease Studies
Introduction
1
Head and neck cancer (HNC) encompasses a broad spectrum of heterogeneous cancer originating in the head and neck region, including cancers of the oral cavity, nasopharynx, oropharynx, larynx, hypopharynx, and other related sites, and each subtype within this group is associated with a unique etiology, epidemiological trends, and therapeutic approach [1]. Head and neck squamous cell carcinoma (HNSCC), the major histological type of HNC, is the sixth most common cancer worldwide [2, 3]. An estimated 59,600 new cases of cancer originating in the oral cavity and pharynx, along with 12,700 cancer‐related deaths, were estimated for 2025 [4]. According to estimates by the World Health Organization, 439,000 cases of mouth and oropharyngeal cancer are expected to occur in 2030 [5]. In terms of stage distribution, 29% of cases are classified as localized, 55% as regional, and 9% as distant in oral cavity and pharynx cancer [4]. Current HNC treatment options include surgery, radiotherapy, chemotherapy, targeted therapy, and immunotherapy, which vary on an individual basis and are normally determined by Multidisciplinary Team (MDT) discussion. For instance, surgeries represent a backbone for the treatment of early‐stage oral cavity cancers, whereas in advanced unresectable cases, chemoradiotherapy is preferred. Despite recent advancements like immunotherapy, long‐term survival remains low, with a 5‐year survival rate of 60.6% [5]. The five‐year survival rate for oral cavity and pharyngeal cancers varies by stage: 84% for localized cases, 65% for regional cases, and 39% for distant cases [6]. Survival disparities also exist among cancers originating from different sites, with 5‐year relative survival rates (RSRs) of 49.0% for the oral cavity, 54.8% for the oropharynx, 50.0% for the hypopharynx, and 63.4% for the larynx [5].
The epidemiological trend of HNC has shifted significantly due to the rising incidence of human papillomavirus (HPV)‐associated oropharyngeal cancer [7, 8]. In the USA, approximately 25,000 HPV‐related cancers are diagnosed annually, with HPV infection accounting for 90% of anal cancers and 65% of vaginal cancers [2, 9, 10, 11]. HPV has been detected in 23%–35% of HNSCC cases globally, with most arising from the oropharynx, where HPV positivity rates range between 45% and 90% [11, 12, 13]. While HPV has been well established as a driver of oropharyngeal cancer, its role in other HNC remains controversial. Interestingly, HPV‐positive and HPV‐negative diseases represent two distinct groups, differing in epidemiology, clinicopathological characteristics, and treatment response [14, 15]. HPV‐associated HNC generally presents with a limited T stage, a more advanced N stage, and an overall advanced stage [16]. Patients with HPV‐associated cases are typically younger, non‐smokers, male, of higher socioeconomic status, and Caucasian [17, 18, 19, 20]. A recent radiomic study indicates that HPV‐negative cancers are radiologically more aggressive, showing signs of invasion into the prevertebral fascia, posterior wall of the hypopharynx, and other structures [21]. Additionally, HPV‐related cases are associated with fewer comorbidities and greater sensitivity to chemotherapy and radiotherapy [1].
In the era of precision medicine, it is crucial to investigate the impact of HPV infection on HNC prognosis and to analyze its epidemiological trends using larger sample sizes. Such studies may provide valuable insights for bench research and clinical management. However, most previous studies relied on small samples rather than population‐based data, limiting their representativeness and generalizability. Additionally, regarding the metastatic patterns of HNC, prior research has primarily focused on metachronous metastasis, which develops during post‐treatment follow‐up [22, 23, 24, 25, 26, 27]. We hypothesize that a study based on a population‐based dataset may provide more solid evidence about revealing HNC epidemiology. This study aims to elaborate on the role of HPV in HNC prognosis using data from the Surveillance, Epidemiology, and End Results (SEER) database.
Materials and Methods
2
Case Inclusion
2.1
All cases in the current study were obtained from the SEER cancer registry, established by the National Cancer Institute in 1973 with the original nine registries: Connecticut, Detroit, Atlanta, San Francisco‐Oakland, Hawaii, Iowa, New Mexico, Seattle‐Puget Sound, and Utah. The registry later expanded to include 13 and subsequently 18 registries. The SEER database records clinicopathological and demographic information, including sex, age, year of diagnosis, tumor stage, survival time, survival status, and other relevant details [28]. Currently, the 18 SEER registries cover approximately 28% of the total U.S. population, representing the most comprehensive data resource for cancer epidemiological studies [29]. Data collection was performed using SEERStat version 8.3.2 [30]. Since HPV status first became available in 2010, only cases diagnosed after January 1, 2010, with definitive HPV status were included in this study. Multiple methodologies exist for ascertaining HPV status in the database. This field is reserved for HPV status confirmed through molecular techniques such as in situ hybridization (ISH), polymerase chain reaction (PCR), or reverse transcription PCR (RT‐PCR), which directly identify viral DNA or RNA, instead of surrogate markers like p16 [31]. To enhance study quality, only cases with active and complete follow‐up were enrolled. Cases diagnosed solely by autopsy or death certificate were excluded, and only cases confirmed by positive histology were included. All cases included were staged based on the AJCC seventh edition. Age was categorized into four groups: 0–45, 46–60, 61–75, and 75+. Race and tumor grade classifications adhered to the standardized definitions established by the SEER database, ensuring consistency with nationally recognized criteria [29]. Based on ICD‐O‐3 site codes, the primary regions were grouped as follows: gum and other mouth, hypopharynx, nasopharynx, oropharynx, other oral cavity and pharynx, tongue, and tonsil [32]. The following Histologic Type ICD‐O‐3 were used to identify solid tumors in the head and neck region (C000‐C148, C300‐C329, C410, C411, C442). Case ascertainment aligned with the SEER coding guidelines to ensure standardized tumor classification. The patient selection protocol was algorithmically executed within the SEERStat platform with predefined inclusion/exclusion criteria, consistent with established methodologies for SEER database analyses. Subsequent to data retrieval, the analytical exclusion involved implementation of propensity score matching, yielding a balanced cohort of 7100 cases (3550 matched pairs) derived from an initial population of 14,855 HNC cases.
Statistical Analyses
2.2
To clarify the impact of HPV infection on the prognosis of HNC patients, we calculated the RSRs, which are widely used to illustrate net survival directly attributable to the index cancer [33, 34, 35, 36, 37, 38, 39, 40]. RSR was calculated using the Ederer II methodology and the expected survival table: U.S. 1970–2015 by individual year (Caucasian, African American, Other [AI/API], Ages 0–99, and all races for Other Unspecified 1991+ and Unknown). Specifically, RSRs were determined by dividing the observed survival (percentage of HNC patients alive at a given time point) by the expected survival (percentage of the general population alive at the same time point). Differences in all‐cause survival were evaluated using the Kaplan–Meier method with log‐rank tests for comparison. To improve comparability between HPV‐positive and HPV‐negative patients, we performed propensity score matching based on HPV status using the nearest neighbor method with a caliper of 0.01 and a ratio of 1:1. Adjustments were made for age group, sex, year of diagnosis, race, primary site, grade, surgery, radiation, chemotherapy, insurance status, marital status, and T, N, and M stages [41]. For survival analysis, the observation period spanned from the date of diagnosis to December 2021, with administrative censoring applied at the study endpoint to ensure uniform follow‐up. The risk factors for all‐cause mortality were assessed using univariate Cox regression and subsequently multivariate Cox regression, with respective 95% confidence intervals for both regression analyses [42]. Only risk factors demonstrating statistically significant prognostic value in univariate Cox regression were incorporated into the multivariate analysis. To validate the proportional hazards assumption essential for Cox regression modeling, the Schoenfeld residuals test was performed by the survival package in R. The results confirmed no significant violations of the proportional hazards assumption, supporting the appropriateness of the Cox model for this analysis. The statistical tests include the t‐test or Mann–Whitney U test, as appropriate, for continuous variables; ANOVA for multi‐group comparisons of continuous variables; and Cox regression for survival modeling. All statistical analyses were conducted using the survival and MatchIt packages in R version 3.3.3 [43, 44, 45]. A two‐tailed p value less than 0.05 was defined as significant.
Results
3
Baseline Characteristics
3.1
A total of 14,855 HNC cases were included in this study, comprising 10,128 HPV‐positive and 4727 HPV‐negative cases (Table 1). Significant differences were observed between HPV‐positive and HPV‐negative patients in terms of sex, age, race, year of diagnosis, site, differentiation level, surgery, radiotherapy, chemotherapy, insurance status, marital status, lung metastasis, brain metastasis, liver metastasis, bone metastasis, T stage, N stage, and M stage (p < 0.001). After propensity score matching at a 1:1 ratio, 3550 HPV‐positive and 3550 HPV‐negative patients were matched, with no significant differences in the aforementioned clinicopathological factors (Table 1).
Baseline characteristics by primary site were also summarized (Table 2). Surgery was more prevalent in cancers originating from the tonsil (48.7%) and gum and other mouth (40.4%) compared to other HNC types. Radiotherapy was widely adopted for HNC management, with rates ranging from 65.5% to 87.9%. Notably, nasopharyngeal cancer distinguished itself with the youngest mean age at diagnosis (48 years), higher prevalence among Asian or Pacific Islanders, and a higher incidence of lung, liver, and bone metastases at diagnosis. Cancers originating from the gum and other mouth were characterized by a higher percentage of female cases, greater prevalence among African American patients, and a higher incidence of N0 stage cases.
Regarding the metastatic patterns of HNC, lung, liver, and bone were the most common sites for metastasis, with crude incidences of 2%, 1%, and 1%, respectively (Table 3). Female HNC patients exhibited a higher propensity for metastasis, particularly to the bone and lung, compared to males. Asian and Pacific Islanders had the highest risk of metastatic disease, including bone, brain, liver, and lung metastases. Additionally, African American patients were found to have a higher risk of lung metastasis (4%).
In terms of socioeconomic factors, uninsured patients were at a higher risk of metastasis to the bone, brain, liver, and lung compared to insured patients. Similarly, unmarried patients were associated with a higher risk of metastasis, particularly to the bone and lung. By primary site, nasopharyngeal cancer had the highest risk of all types of metastasis, followed by hypopharyngeal cancer.
Survival Analyses for HNC
3.2
To further demonstrate the net prognostic impact of HPV infection on HNC patients, RSRs were calculated across clinicopathological factors. HPV infection was associated with a favorable prognosis in all patients, regardless of sex, race, and primary site, including cancers of the oral cavity, pharynx, tongue, tonsil, oropharynx, hypopharynx, and other oral cavity and pharynx regions (Figures 1, 2, 3). However, this prognosis‐stratifying effect was absent in cancers originating in the gum, other mouth regions, and nasopharynx (Figure 2C,D).
The relative survival rate of head and neck cancer by HPV status by sex (A, B) and race (C–F).
The relative survival rate of head and neck cancer by HPV status by originated site (A–H).
Subgroup analyses by differentiation grade revealed HPV status as a significant prognostic factor in grade I–III tumors but not in grade IV disease (Figure 3C,E,G,I). HPV status further demonstrated consistent prognostic stratification across all categories of radiation therapy, chemotherapy, insurance status, and marital status (Figures 3B,D,F,H,J and 4). To identify independent prognostic factors for HNC patients, multivariate Cox regression analyses were performed (Table 4). Significant factors associated with prognosis included race, age, year of diagnosis, primary site, differentiation grade, surgical status, radiotherapy status, chemotherapy status, insurance status, marital status, synchronous lung, brain, liver, and bone metastasis, T stage, N stage, M stage, and HPV status. Specifically, the hazard ratio (HR) for all‐cause mortality was 1.25 (1.13–1.40) for African American patients, with Caucasian patients as the reference group. HR increased with age: 1.39 (1.25–1.60) for ages 45–59, 2.26 (2.00–2.56) for ages 60–75, and 4.15 (3.46–4.98) for patients over 75 years. Patients diagnosed between 2012 and 2015 had a higher risk of death compared to those diagnosed in 2010. Hypopharyngeal and oropharyngeal cancers showed significantly higher mortality risks compared to tonsil cancer (Table 4).
The relative survival rate of head and neck cancer by HPV status in all patients (A), by differentiation level (C, E, G, I), chemotherapy status (B, D), and radiotherapy status (F, H, J).
The relative survival rate of head and neck cancer by HPV status by insurance status (A, C, E) and marital status (B, D, F).
Grade III and IV tumors were associated with lower mortality risks, with HRs of 0.81 (0.67–0.99) and 0.71 (0.52–0.99), respectively. Patients without surgery had a higher risk of death (HR = 1.92 (1.74–2.12)) compared to those who underwent surgery. Refusal of radiotherapy or chemotherapy was linked to significantly higher risks of death (HR = 3.76 (2.98–4.73) and HR = 1.46 (1.33–1.60), respectively). Uninsured and unmarried patients had elevated mortality risks (HR = 1.33 (1.14–1.55) and HR = 1.60 (1.48–1.73), respectively) compared to their insured or married counterparts. Synchronous metastases to the lung, brain, liver, and bone were also associated with higher risks of death, with HRs of 1.53 (1.23–1.91), 2.706 (1.70–4.30), 1.34 (1.02–1.75), and 1.52 (1.20–1.92), respectively, compared to non‐metastatic patients. Advanced T, N, and M stages were linked to increased mortality risk. Positive HPV status was associated with a significantly lower risk of death (HR = 0.50 (0.46–0.54)) compared to HPV‐negative patients.
To further clarify HPV's role in HNC, propensity score matching was used to match cases by HPV status, followed by univariate Cox regression analyses in various subgroups (Table 5). Consistently lower mortality risks in HPV‐positive patients were observed across most subgroups, confirming the favorable prognostic role of HPV in HNC cases.
Discussion
4
The current study demonstrated the clinical characteristics of HNC based on HPV status, primary site, and metastatic patterns, as well as the survival implications of HPV in HNC. To the best of our knowledge, this is the first population‐based study providing representative and generalizable data. The novelty and impact of this study lie in its comprehensive analysis of HNC epidemiology using a population‐based dataset. To further mitigate confounding biases when elaborating on the prognostic role of HPV, we implemented propensity score matching, enhancing the robustness of our findings.
HNC represents a heterogeneous group of diseases, with 75% associated with smoking and alcohol exposure, and 25% related to HPV infection [8, 46]. HPV‐positive and HPV‐negative HNC represent two distinct disease types in terms of natural history and clinicopathological characteristics. HPV‐infected patients tend to be younger than their non‐infected counterparts, suggesting that HPV may accelerate the carcinogenesis process. Furthermore, HNC patients with HPV infection are less likely to have tobacco or alcohol exposure, indicating that HPV can promote carcinogenesis independently of these factors [30]. Most cancers originating from the gum, hypopharynx, and nasopharynx are HPV‐negative, whereas the majority of tongue and tonsil cancers are HPV‐positive, suggesting differences in the etiology of various HNC types. The higher HPV positivity among Caucasian patients (89.6%) may be attributed to the higher prevalence of HPV infection in these populations (71.5%) compared to African Americans (66.2%) [32]. The association between socioeconomic status (e.g., income, education), race, tobacco exposure, sexual behavior, and HPV prevalence in HNC may be explained through multifactorial mechanisms [47]. Despite the more advanced N stage in HPV‐positive HNC patients, these patients exhibit a lower incidence of M1 disease and metastasis to the lung, brain, liver, or bone, though the underlying mechanism remains unknown. The prognostic value of HPV infection is limited in cancers originating from the gum, other mouth tissues, and nasopharynx, as revealed by both RSRs and Cox regression analyses after propensity score matching. Although the specific molecular events driving the better prognosis in HPV‐infected patients remain unclear, there is a growing trend toward advocating de‐intensified treatment to reduce post‐treatment toxicity without compromising cancer control. The eighth edition of the AJCC staging system introduces a unique classification for HPV‐positive squamous oropharyngeal cancer, resulting in downstaging for 92% of cases and increasing the proportion of stage I patients from 3% to 64% [48]. However, the recommended treatment protocol by stage based on this novel staging system has not yet been published. In line with the modification of the staging system, de‐intensified treatment strategies are under exploration, particularly for HPV‐positive patients with a lower risk of recurrence, such as those with a smoking history of less than 10 pack‐years and non‐T4 disease [17, 49, 50, 51, 52]. However, robust evidence supporting de‐escalation remains lacking to date. The clinical community expects multicenter randomized controlled trials to clarify which patients are most likely to benefit from such strategies. The baseline characteristics of patients in the current study differ slightly from those in another study based on the NCDB, which can be attributed to the differing inclusion criteria [53]. Regarding the clinical testing of HPV, a recent study highlights critical limitations of relying solely on p16 as a surrogate for HPV status in oropharyngeal cancer [54]. The notable discordance between p16 and HPV nucleic acid status—particularly in regions with low HPV‐attributable fractions—underscores the prognostic heterogeneity masked by p16 alone. Patients with discordant results (p16+/HPV− or p16−/HPV+) exhibited intermediate survival outcomes, distinct from both HPV‐driven and HPV‐negative tumors. These findings advocate for mandatory dual testing where HPV status informs therapeutic decisions, ensuring accurate risk stratification and tailored treatment, especially in low‐HPV‐prevalence populations. In the multivariate Cox regression, we observed counterintuitive hazard ratios for grade and year of diagnosis. This phenomenon may be attributed to residual confounding, where unmeasured or inadequately adjusted covariates exhibit stronger prognostic associations than tumor grade and year of diagnosis. Such paradoxical findings are consistent with a prior report [55]. In terms of metastasis in HNC, the current study primarily focuses on synchronous metastasis, which may provide valuable data for clinical screening at initial diagnosis. Historical studies published in the 1990s reported metastasis rates of 10%–17% in HNC, a figure notably higher than that observed in our study [56, 57, 58]. This counterintuitively higher incidence of metastasis in earlier studies, despite less‐developed methods for detecting metastasis, may be attributed to delayed diagnosis at that time. Different cancer types exhibit varying metastatic potentials, likely influenced by intrinsic tumor biology. For instance, while oropharyngeal cancer generally presents with a more advanced N stage compared to hypopharyngeal cancer, the incidence of metastasis is higher in hypopharyngeal cancer (6.8% vs. 5.7%). The lungs are the most common site of metachronous metastasis in HNC, followed by bone and liver, consistent with previous publications [59, 60]. Advanced stage grouping, increasing N classification, node positivity, extranodal extension, and HPV negativity are factors associated with the development of distant metastases, independent of any changes in treatment paradigms [23]. Thus, the most effective way to reduce the incidence of distant metastases is to diagnose HNSCC at earlier stages [23]. Nasopharyngeal cancer had the highest percentage of M1 disease (9.9%), followed by hypopharyngeal cancer (6.8%), consistent with a previous study based on the National Cancer Data Base in the USA [53].
Despite novel findings, the current study should be interpreted in the context of its limitations. First, only patients with definite HPV status were included, as the percentages of unknown HPV status were 77.16%, 65.51%, 56.28%, 49.50%, 43.80%, 39.79%, and 33.25% across calendar years. As a result, the epidemiological trends reported here may be biased, particularly in the earlier periods with limited patient enrollment. Due to incomplete HPV information, HPV‐based incidence of HNC could not be reported. However, to the best of our knowledge, SEER data remain the most comprehensive publicly available resource, and future studies with more detailed data may provide further insights into this topic. Second, HPV subtypes were not available in the current dataset, preventing comparisons based on HPV subtypes. Third, caution should be exercised when applying these findings to predict epidemiological trends outside the USA. Fourth, this SEER‐based study may be subject to bias due to potential misclassification or under‐registration in the SEER database.
In conclusion, the current study, based on a large population‐based database, provides generalizable epidemiological data on HNC in terms of HPV status, primary site, and metastatic patterns, as well as the prognostic impact of HPV infection. Analyzing the baseline characteristics of HNC enhances our understanding of the disparities among different HNC subtypes, which may help tailor clinical decision‐making and improve the design of clinical trials for each subtype. Furthermore, clarifying the prognostic role of HPV in HNC may reveal the epidemiological link between HNC pathogenesis and HPV infection, facilitating further bench studies on the role of HPV in HNC.
Author Contributions
Study design: Kangwen Guo and Xiaoqiong Yi. Data collection: Kangwen Guo, Jinmei Li, Haiyin Ye, and Xiaoqiong Yi. Statistical analyses: Kangwen Guo, Jinmei Li, Haiyin Ye, and Xiaoqiong Yi. Manuscript drafting: Kangwen Guo, Haiyin Ye, and Jinmei Li. Manuscript revision: Kangwen Guo and Xiaoqiong Yi.
Ethics Statement
This retrospective study utilized fully anonymized, pre‐existing data from the SEER database, with no identifiable patient information. Ethical approval was waived in accordance with national regulations and the Declaration of Helsinki, which exempts studies involving anonymized data from formal ethics review when the research poses no risk to participants.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. Lo Nigro , N. Denaro , A. Merlotti , and M. Merlano , “Head and Neck Cancer: Improving Outcomes With a Multidisciplinary Approach,” Cancer Management and Research 9 (2017): 363–371.28860859 10.2147/CMAR.S 115761 PMC 5571817 · doi ↗ · pubmed ↗
- 2S. Begum , D. F. Cao , M. Gillison , M. Zahurak , and W. H. Westra , “Tissue Distribution of Human Papillomavirus 16 DNA Integration in Patients With Tonsillar Carcinoma,” Clinical Cancer Research 11, no. 16 (2005): 5694–5699.16115905 10.1158/1078-0432.CCR-05-0587 · doi ↗ · pubmed ↗
- 3F. Ciardiello and G. Tortora , “A Novel Approach in the Treatment of Cancer: Targeting the Epidermal Growth Factor Receptor,” Clinical Cancer Research 7, no. 10 (2001): 2958–2970.11595683 · pubmed ↗
- 4R. L. Siegel , T. B. Kratzer , A. N. Giaquinto , H. Sung , and A. Jemal , “Cancer Statistics, 2025,” CA: A Cancer Journal for Clinicians 75, no. 1 (2025): 10–45.39817679 10.3322/caac.21871 PMC 11745215 · doi ↗ · pubmed ↗
- 5G. Cadoni , L. Giraldi , L. Petrelli , et al., “Prognostic Factors in Head and Neck Cancer: A 10‐Year Retrospective Analysis in a Single‐Institution in Italy,” Acta Otorhinolaryngologica Italica 37, no. 6 (2017): 458–466.28663597 10.14639/0392-100X-1246 PMC 5782422 · doi ↗ · pubmed ↗
- 6R. L. Siegel , K. D. Miller , and A. Jemal , “Cancer Statistics, 2019,” CA: A Cancer Journal for Clinicians 69, no. 1 (2019): 7–34.30620402 10.3322/caac.21551 · doi ↗ · pubmed ↗
- 7D. P. Zandberg , R. Bhargava , S. Badin , and K. J. Cullen , “The Role of Human Papillomavirus in Nongenital Cancers,” CA: A Cancer Journal for Clinicians 63, no. 1 (2013): 57–81.23258613 10.3322/caac.21167 · doi ↗ · pubmed ↗
- 8A. K. Chaturvedi , E. A. Engels , R. M. Pfeiffer , et al., “Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States,” Journal of Clinical Oncology 29, no. 32 (2011): 4294–4301.21969503 10.1200/JCO.2011.36.4596 PMC 3221528 · doi ↗ · pubmed ↗