Optimizing Management of Testicular Torsion at Bronglais General Hospital: Assessing the Testicular Workup for Ischemia and Suspected Torsion (TWIST) Score and Ultrasound for Effective Time Intervention
Sami E Mohammed, Samy R Mohamed, Michael Aniah, Mohamed A Ali, Arinze Chukwuonwe, Subhiksha Kanagaraj

TL;DR
This study examines how testicular torsion is managed at a UK hospital, aiming to improve diagnosis and reduce delays in treatment.
Contribution
The study introduces a local protocol to streamline testicular torsion management and highlights gaps in using diagnostic tools like the TWIST score and ultrasound.
Findings
Only 38% of patients with suspected testicular torsion had confirmed cases.
The TWIST score was used in just 6% of cases, and ultrasound in 9%.
A local protocol was developed to improve timely intervention and reduce delays.
Abstract
Background: Testicular torsion (TT) is a urological emergency requiring timely surgical intervention to prevent testicular loss. Different assessment approaches were suggested to improve overall patient outcomes, as the Testicular Workup for Ischemia and Suspected Torsion (TWIST) score, which has been integrated with ultrasound findings to enhance diagnostic accuracy in suspected cases of testicular torsion. Additionally, Doppler ultrasound is recommended in accordance with recently updated national and international guidelines. Methodology: This is a retrospective study conducted at Bronglais General Hospital (BGH), Aberystwyth, United Kingdom, from January 2019 to January 2024 of patients who had undergone scrotal exploration for suspected TT. A total of 34 patients were included in the study. Objective: The study aims to review the management of all patients who present to BGH with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
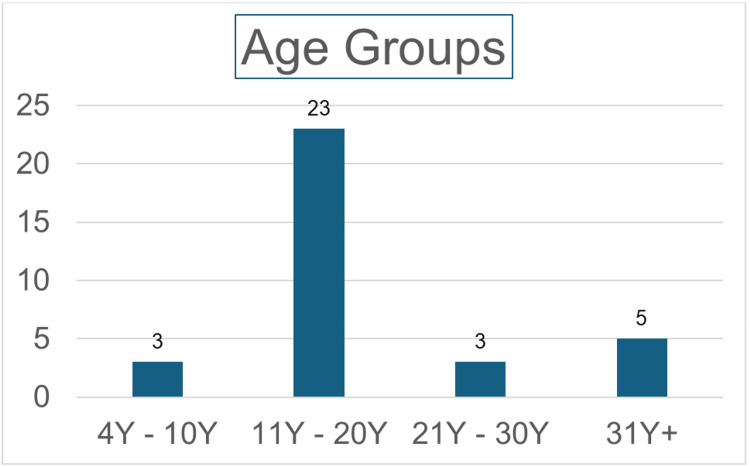 Figure 1
Figure 1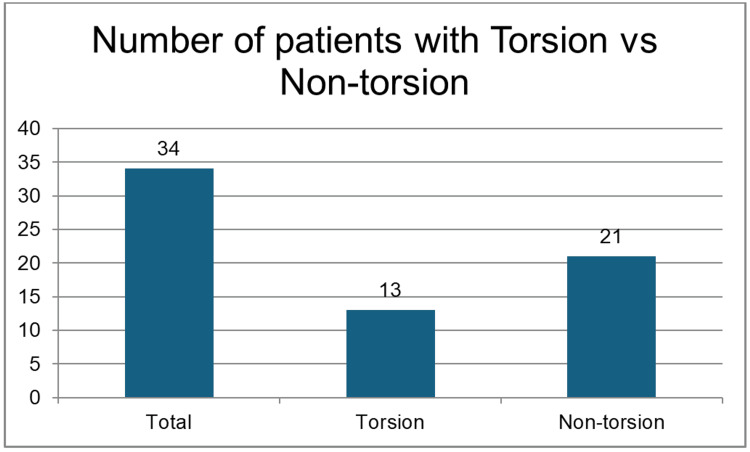 Figure 2
Figure 2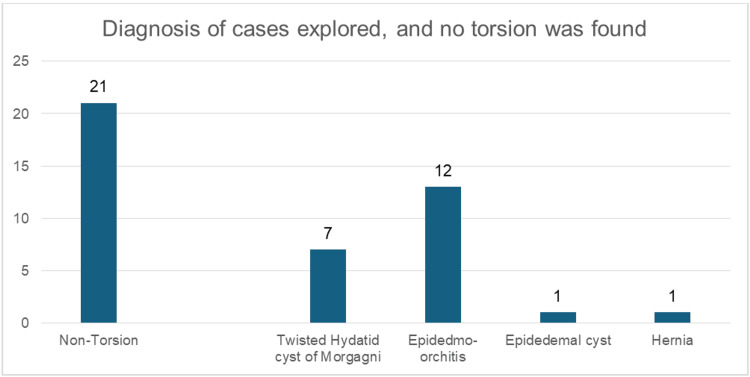 Figure 3
Figure 3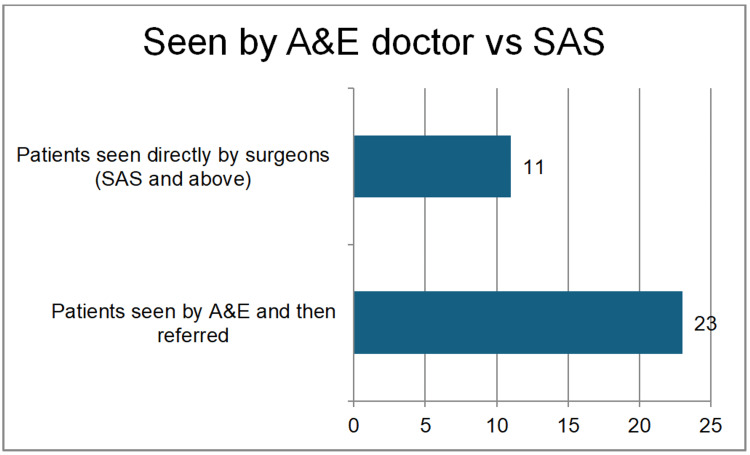 Figure 4
Figure 4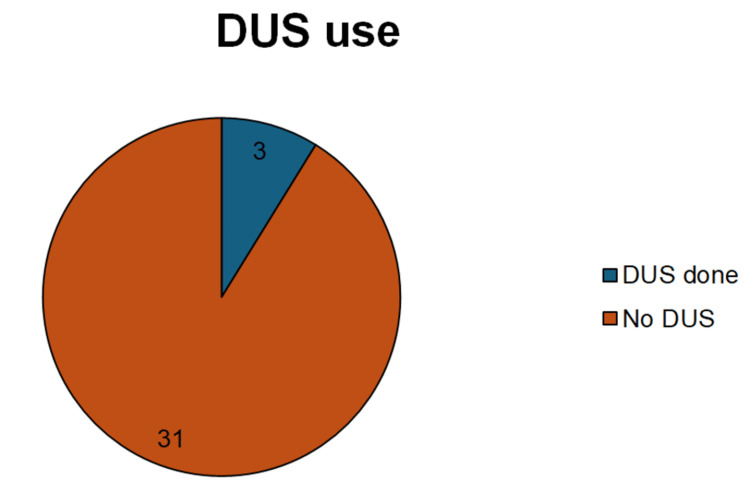 Figure 5
Figure 5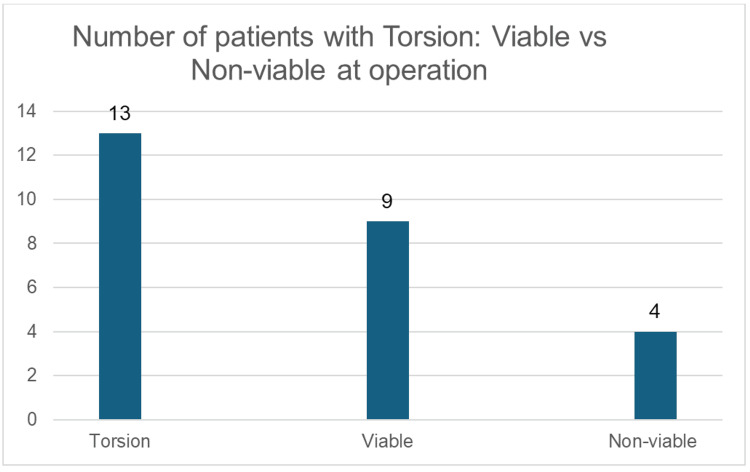 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Male Reproductive Health Studies · Intraperitoneal and Appendiceal Malignancies
Introduction
Testicular torsion (TT) is a urological emergency requiring timely surgical intervention to prevent testicular loss. Management relied on clinical judgement, with the earliest surgical exploration being the approach to minimise ischaemic loss [1]. However, relatively new tools for assessing risk, such as the Testicular Workup for Ischemia and Suspected Torsion (TWIST) score and Doppler scrotal ultrasound (DUS), have improved the accuracy of diagnosis of TT, leading to accelerated scrotal explorations and ensuring that cases get treated on time [2,3].
Challenges persist in balancing rapid expert surgical referral with diagnostic precision on suspected TT. This study looks at how things are done now by reviewing past cases and suggests a better process that combines the assessment by more expert doctors and careful use of ultrasound to achieve better results [4].
This article was previously presented as a meeting abstract at the 2025 Association of Surgeons of Great Britain and Ireland (ASGBI) International Surgical Congress EICC, Edinburgh, Scotland, on May 13, 2025 [5].
Materials and methods
Study design and setting
This retrospective cohort study was conducted at Bronglais General Hospital (BGH), a rural district general hospital in Aberystwyth, United Kingdom. The study reviewed all male patients who underwent scrotal exploration for suspected TT between January 2019 and January 2024.
Study population and sample size
A total of 34 patients were identified from the hospital's information department using procedural codes for scrotal exploration. All patients who underwent surgery for suspected TT within the study period were included. There were no exclusion criteria.
Data collection and study measures
Data were collected retrospectively from patients' records, including operation notes, clinic letters, and nursing charts. The primary data points collected were patient demographics, clinical presentation (including symptoms and signs), and documentation of the TWIST score. The TWIST score is a clinical tool used to assess the likelihood of testicular torsion in cases of acute scrotal pain. The TWIST score (range 0-7) comprises hard testis (2 points), testicular swelling (2 points), nausea and vomiting (1 point), high-riding testis (1 point), and absent cremasteric reflex (1 point) [2]. Patients were classified into three groups: 1. Low risk (0-2 points): Unlikely torsion; consider alternative diagnoses. 2. Intermediate risk (3-4 points): Ambiguous cases; ultrasound recommended. 3. High risk (5-7 points): There is a high probability of torsion, needing immediate surgery without prior imaging [6]. Additionally, the findings of DUS include time points from arrival to decision-to-operate and to surgery, intraoperative findings (viability of the testis), and the final diagnosis.
The primary outcome was to assess the management of suspected TT against national guidelines (Getting It Right First Time (GIRFT) [7], National Confidential Enquiry into Patient Outcome and Death (NCEPOD)) [8] to develop a local protocol. Secondary outcomes included the diagnostic accuracy of scrotal exploration (confirmed TT vs. alternative diagnoses) and an analysis of causes for delayed intervention.
Ethical considerations
This study is a retrospective clinical audit; therefore, formal ethical approval was not required as per institutional policy. Patient consent is not needed for the same reason. All data were anonymised during collection and analysis to maintain patient confidentiality.
Statistical analysis
Data analysed by using IBM SPSS Statistics for Windows, version 21 (released 2012; IBM Corp., Armonk, New York, United States). Descriptive statistics (graphs, tables, percentages) are used to summarise the data. No adjustments were applied for multiple comparisons due to the observational nature of the study.
Results
Thirty-four patients underwent scrotal exploration from January 2019 to January 2024 at BGH; 67.64% (n=23) were in the age group of 11 to 20 years (Figure 1).
The distribution of patients as per their age groupy: years
Diagnostic accuracy
Only 38% (n=13) had confirmed TT, while 62% (n=21) had alternative diagnoses (twisted hydatid: n=7, 33%; epididymo-orchitis: n=12, 57%; epididymal cyst: n=1, 4.7%; hernia: n=1, 4.7% (Figures 2, 3)).
Distribution of patients as per their condition: torsion vs. non-torsion
Diagnosis of cases explored, and no torsion was found
Only 9% (n=3) underwent surgery within the ideal one-hour window post decision, 35% (n=12) lacked documentation of critical time points (e.g., decision-to-operation), patients were seen by accident and emergency (A&E) doctors first (n=23) 67.6%, and directly referred to the surgical on-call team (n=11) 32% (Figure 4).
Patients reviewed by A&E doctors and referred vs. direct review by the surgical teamA&E: accident and emergency; SAS: staff grade associate specialist
Underutilisation of diagnostic tools, as the TWIST score was documented in only 6% (n=3) cases. DUS was performed in only 9% (n=3) of cases (Figure 5).
Number of patients who had DUS vs. no DUS doneDUS: Doppler scrotal ultrasound
These findings highlight inefficiencies in risk stratification and delays in definitive management, showing the importance of a standardised protocol. Among patients who had confirmed torsion (n=13), the testis was viable in (n=9) 69% and non-viable in (n=4) 31% of the patients (Figure 6).
Number of patients with torsion: viable vs non-viable at operation
Discussion
Barbosa et al. introduced the TWIST score for acute scrotal pain in 2013 [6]. Despite its efficacy, our study revealed low usage (6%) of the TWIST score at BGH, suggesting missed opportunities to reduce unnecessary explorations. The studies validated the TWIST score, showing a negative predictive value (NPV) of 98.5% for low-risk scores, effectively excluding TT. High-risk scores (≥5) correlate strongly with torsion, justifying urgent surgery [9, 10].
At BGH, only 9% (n=3) of patients underwent DUS, showing either underuse or systemic barriers (e.g., limited availability). Liang et al. concluded that DUS has a sensitivity of 100% and a specificity of 97.9% for detecting torsion [11]. Current evidence supports avoiding ultrasound in high-risk (TWIST ≥5) cases to prevent treatment delays [12]. Reserving ultrasound for intermediate-risk (TWIST 3-4) or equivocal presentations [13]. Gopal et al. reported that the use of DUS in low-risk and intermediate-risk patients was accurate in 95% of patients presenting with acute scrotum to exclude TT, and the use of the TWIST score with DUS led to a plummet in the annual cost to £93,000 less in one hospital [14].
The study findings are consistent with the NCEPOD’s guidelines (2024) [8], which emphasise surgery within four hours of symptom onset to salvage viability. European Association of Urology (EAU) guidelines (2023) [15] recommend selective ultrasound use, particularly if the presentation to hospital is more than six hours after the onset of symptoms, and the TORSAFUF (TOrsion of the Right or SAmenatic Fun / Ultrasound Factors) study (n=2922) supports ultrasound safety, but clinical suspicion is more important than DUS [16].
As per GIRFT children and young people, the TT pathway reported that patients with suspicion of TT should be assessed by the surgical on-call team within one hour of arrival at A&E and should be operated on within 60 minutes of the decision to operate. A TWIST score of 5 or more warrants scrotal exploration if the onset of pain is less than 48 hours, and if the TWIST score is below 5, it does not rule out TT. Ultrasound is advised if the scrotal pain’s duration is more than 48 hours, or if the pain is less than 48 hours, it’s only used to support the TT diagnosis without delaying surgical intervention, but in neonates, an ultrasound is used to exclude other differential diagnoses. After orchidopexy or orchidectomy, the patients will need urological follow-up to assess testicular atrophy and to discuss prosthesis implantation later. Effective education tools and resources for patients, parents, and schools will raise awareness of TT and the importance of early reporting to health facilities, which would improve management outcomes [7].
At BGH, delays in surgical intervention and low TWIST/ultrasound use suggest systemic gaps. Implementing a structured pathway could reduce unnecessary surgeries (currently 62% non-torsion explorations). Prioritise urgent interventions for high-risk cases. And improve documentation and compliance with guidelines.
The proposed pathway for management of patients with scrotal pain and suspected of TT at BGH to improve care is as follows: 1. Initial assessment: Rapid TWIST scoring by emergency clinicians; high-risk (≥5 points): Immediate surgical referral without imaging; intermediate-risk (3-4 points): Expedited ultrasound (if available); proceed to surgery if positive/equivocal; and low-risk (≤2 points): Consider alternative diagnoses (e.g., infection); ultrasound if symptoms persist. 2. Operational improvements: mandate TWIST scoring for all acute scrotum presentations, fast-track surgical referrals for high-risk cases, strict time tracking starting from arrival to accident and emergency, surgeon review, prompt operative intervention, and staff training on TT recognition and documentation.
The study has several limitations, as its retrospective design relies on medical records, which may introduce documentation biases or incomplete data. The small sample size (n = 34) from a single rural centre study makes it susceptible to selection bias. Additionally, potential confounding factors, such as variations in clinician experience or resource availability during out-of-hours periods, were not fully controlled.
Conclusions
Integrating the TWIST score into initial assessments at BGH can improve the accuracy of TT diagnosis and reduce delays. Ultrasound can be selectively used as an adjunct in intermediate-risk cases, ideally to avoid unnecessary explorations, but in our rural setting, getting a sonographer isn’t always feasible for out-of-hours ultrasound; it’s better to have the surgical team assess urgently, deciding on exploration without delay. In order to avoid prolonging time-to-surgery, it is important to emphasise the importance of developing a standard protocol, staff education, and improved documentation for improving outcomes in this time-sensitive condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management of acute scrotum in children: a 25-year single center experience on 558 pediatric patients Can J Urol PogorelićZ MustapićK JukićM 85948601232016 http://pubmed.ncbi.nlm.nih.gov/27995859/27995859 · pubmed ↗
- 2Development and initial validation of a scoring system to diagnose testicular torsion in children J Urol Barbosa JA Tiseo BC Barayan GA 1859186418920132310380010.1016/j.juro.2012.10.056 · doi ↗ · pubmed ↗
- 3Diagnosing testicular torsion before urological consultation and imaging: validation of the twist score J Urol Sheth KR Keays M Grimsby GM 1870187619520162683583310.1016/j.juro.2016.01.101 · doi ↗ · pubmed ↗
- 4Management of the acute scrotum in children ANZ J Surg Corbett HJ Simpson ET 2262287220021207145810.1046/j.1445-2197.2002.02355.x · doi ↗ · pubmed ↗
- 5Ttp 7.14 audit of management of testicular torsion in a rural general hospital BJS Mohammed S Mohamed SR Aniah M Kanagraj S Stolarchuk T 1122025 https://doi.org/10.1093/bjs/znaf 166.307
- 6Prospective validation of clinical score for males presenting with an acute scrotum Acad Emerg Med Frohlich LC Paydar-Darian N Cilento BG Jr Lee LK 147414822420172883389610.1111/acem.13295 · doi ↗ · pubmed ↗
- 7GIRFT children and young people: Testicular torsion pathway (Version 2)GIRFT children and young people: testicular torsion pathway NHS England London, United Kingdom NHS England 2025 https://gettingitrightfirsttime.co.uk/wp-content/uploads/2025/10/Paediatric-testicular-torsion-pathway-guide-FINAL-V 2-October-2025.pdf
- 8Testicular torsion 2024 https://www.ncepod.org.uk/2024 testiculartorsion.html