Biochemical Pseudoprogression in Pancreatic Cancer During Chemotherapy: A Case Report
Abdolhakim Mohamed, Kevin T Dao, Stanley Kim

TL;DR
A pancreatic cancer patient showed biochemical pseudoprogression during chemotherapy, where rising CA 19-9 levels did not reflect worsening disease, highlighting the need to consider clinical improvement alongside biomarkers.
Contribution
This is the first reported case of biochemical pseudoprogression in pancreatic cancer treated with chemotherapy.
Findings
CA 19-9 levels rose significantly during treatment but were followed by a decline and plateau.
The patient experienced clinical improvement despite elevated biomarker levels.
The case highlights the importance of integrating clinical status with biomarker interpretation.
Abstract
Pancreatic ductal adenocarcinoma (PDAC) is a highly lethal malignancy, most often diagnosed at an advanced stage, with limited treatment options and poor outcomes. CA 19-9 is the most commonly used biomarker to support the diagnosis and for treatment monitoring of PDAC, but rising levels during treatment usually suggest disease progression. Pseudoprogression, a transient increase in tumor burden or biomarker levels followed by subsequent improvement, has been described in glioblastoma and in cancers treated with immune checkpoint inhibitors (ICIs), but to our knowledge, it has not previously been reported in pancreatic cancer treated with cytotoxic chemotherapy. We describe a 52-year-old man with metastatic PDAC who was treated with FOLFOX due to underlying cardiac comorbidities. Despite rising CA 19-9 levels from 2,344 U/mL at baseline to more than 90,000 U/mL after two months of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
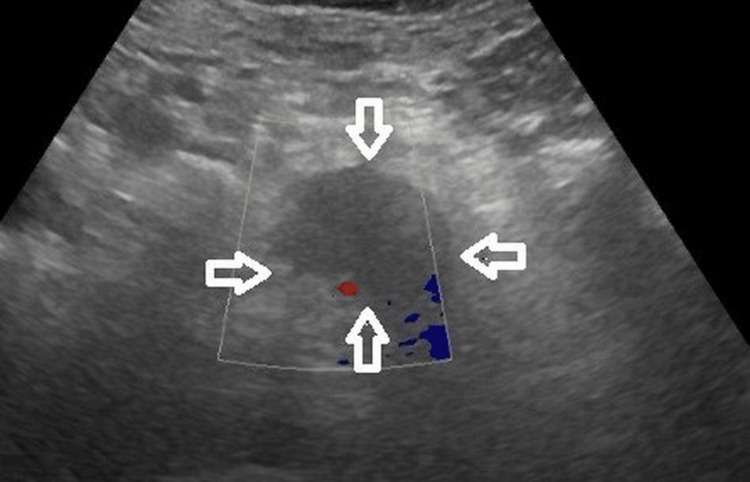 Figure 1
Figure 1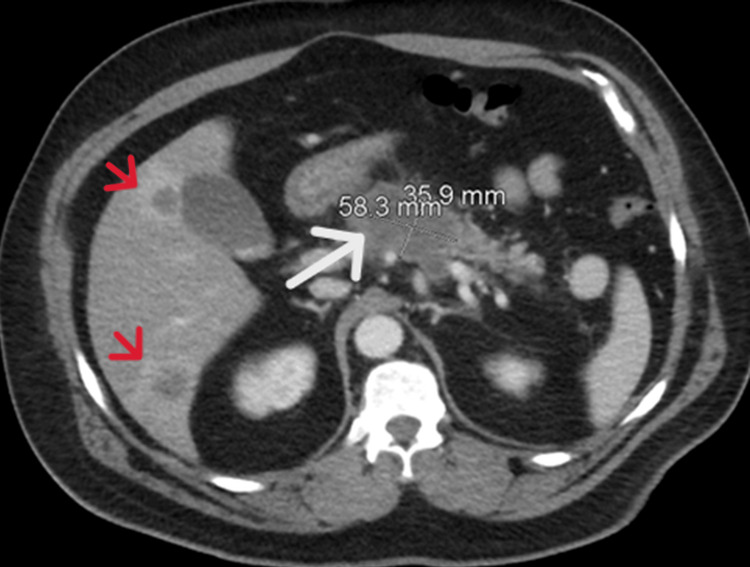 Figure 2
Figure 2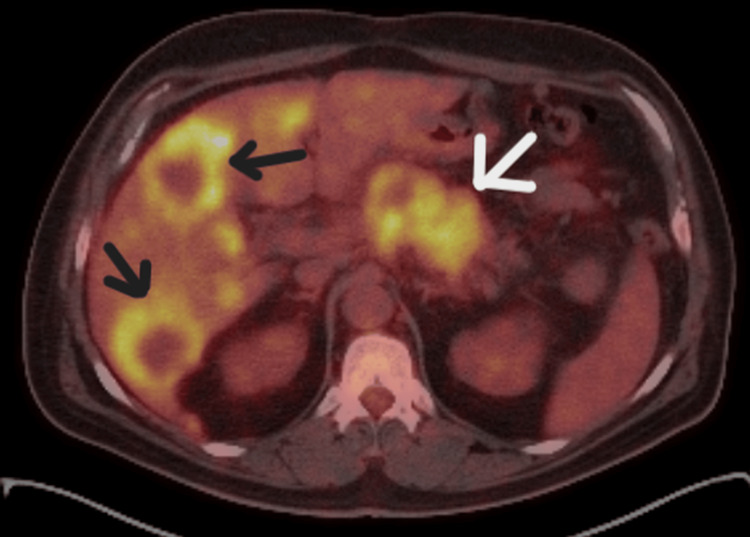 Figure 3
Figure 3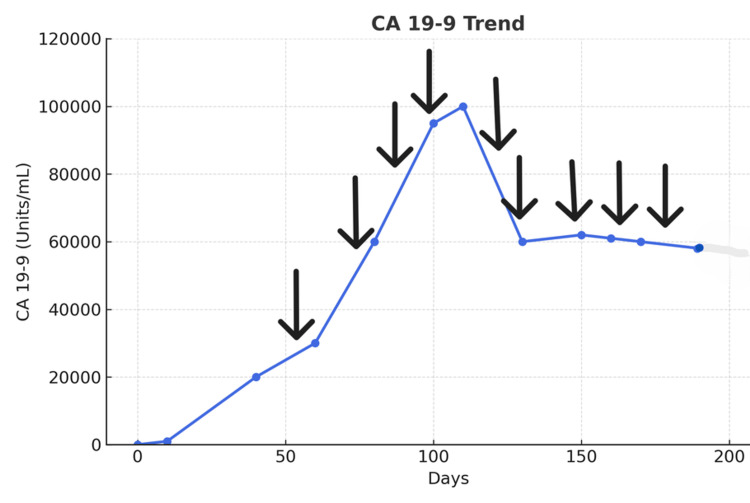 Figure 4
Figure 4| Day | CA 19-9 (Normal: <34 U/L) | FOLFOX Chemotherapy |
| 1 | 2,344 | - |
| 21 | 4,057 | - |
| 63 | - | Cycle 1 |
| 70 | 25,452 | - |
| 74 | - | Cycle 2 |
| 80 | 31,084 | - |
| 88 | - | Cycle 3 |
| 90 | 58,560 | - |
| 94 | 51,393 | - |
| 102 | - | Cycle 4 |
| 108 | 91,083 | - |
| 115 | 98,646 | - |
| 116 | - | Cycle 5 |
| 122 | 96,233 | - |
| 135 | - | Cycle 6 |
| 138 | 59,263 | - |
| 143 | 60,309 | - |
| 149 | - | Cycle 7 |
| 157 | 61,818 | - |
| 163 | - | Cycle 8 |
| 171 | 66,172 | - |
| 177 | - | Cycle 9 |
| 185 | 62,673 | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cancer Immunotherapy and Biomarkers · Inflammatory Biomarkers in Disease Prognosis
Introduction
Pancreatic ductal adenocarcinoma (PDAC) accounts for the majority (90%) of pancreatic neoplasms. Its incidence is rising at a rate of 0.5% to 1.0% per year, and pancreatic cancer is projected to become the second-leading cause of cancer death in the U.S. by 2030. Most patients with pancreatic cancer are diagnosed at an advanced stage that is not amenable to curative surgery [1]. For patients with metastatic disease, systemic chemotherapy with modified FOLFIRINOX (fluorouracil, oxaliplatin, leucovorin, and irinotecan) or a combination of paclitaxel and gemcitabine is the first-line therapy. Milder but still effective FOLFOX is often used as a second-line therapy when patients fail paclitaxel and gemcitabine [2]. CA 19-9 is the most commonly used biomarker to support the diagnosis, and CA 19-9 levels during and after chemotherapy can predict a patient’s response to treatment [3]. However, as CA 19-9 is a sialylated Lewis blood group antigen, approximately 6% of the White population and 22% of the Black population in the U.S., who are Lewis antigen-negative, do not produce CA 19-9, even if they have advanced pancreatic cancer [3].
Pseudoprogression is defined as an objective response following initial progression with the same treatment [4], which is clinically manifested as a temporary increase in specific biochemical markers or tumor size during therapy, mimicking true disease progression without indicating a worsening condition. Pseudoprogression has been observed in various cancers treated with immune checkpoint inhibitor (ICI) immunotherapy, mostly in melanoma [4-6]. For instance, prostate-specific antigen (PSA) levels may temporarily rise in prostate cancer patients after starting immunotherapy [5]. However, pseudoprogression has not been seen in metastatic colorectal or pancreatic cancer treated with immunotherapy in clinical studies, nor has it been reported in pancreatic cancer treated with cytotoxic chemotherapy [6]. We present a unique case of biochemical pseudoprogression of metastatic PDAC during active chemotherapy, mimicking actual disease progression.
Case presentation
A 52-year-old Hispanic male with a history of hypertension, type 2 diabetes mellitus, hyperlipidemia, coronary artery disease with stent placements, and obstructive sleep apnea presented to the Emergency Department (ED) with left upper quadrant abdominal pain lasting one week. The pain was rated as 7 out of 10, radiating to the epigastric region and mid-back, and accompanied by abdominal bloating and nausea. He denied vomiting, weight loss, severe weakness, diarrhea, or fever. On physical examination, vital signs were normal. The patient had no jaundice. The left upper abdomen was mildly tender without a palpable mass, and the rest of the physical exam was unremarkable. Laboratory test results showed a normal complete blood count, a normal metabolic panel, slightly elevated alkaline phosphatase (147 units/L), normal alanine transaminase and aspartate aminotransferase, and a normal bilirubin level. Abdominal ultrasound depicted a hypoechoic pancreatic mass in the head and body of the pancreas, measuring 5.8 × 3.7 × 3.9 cm (Figure 1).
Abdominal ultrasound (US) depicting a hypoechoic pancreatic mass in the head and body of the pancreas (arrows), measuring 5.8 × 3.7 × 3.9 cm
A computed tomography (CT) scan of the abdomen and pelvis with contrast revealed a hypodense pancreatic mass, with multiple enhancing low-density liver lesions (Figure 2).
Computed tomography (CT) scan of the abdomen with contrast, revealing a hypodense pancreatic mass (white arrow) and multiple enhancing low-density liver lesions (red arrows)
Positron emission tomography (PET)/CT showed a mass in the head and body of the pancreas, and hypermetabolic lesions in both liver lobes (Figure 3) and periaortic lymph nodes.
Positron emission tomography/computed tomography (PET/CT) scan showing a hypermetabolic pancreatic tumor (white arrow) and metastatic liver lesions (black arrows)
An ultrasound-guided needle biopsy of the hepatic lesion confirmed PDAC with focal squamous differentiation. After discussing options with the patient, chemotherapy was started. Due to his extensive cardiac history, the patient was initiated on FOLFOX every two weeks. CA 19-9 levels were monitored throughout treatment to assess response (Table 1).
The initial CA 19-9 measurement (Day 1) was 2,344 units/mL (normal <37 units/mL), and levels gradually increased to 25,452 units/mL by the first chemotherapy cycle (Day 70). Despite chemotherapy, CA 19-9 levels continued to rise (Figure 2). After four cycles (two months into treatment), CA 19-9 levels exceeded 90,000 units/mL. Without other conditions that could elevate CA 19-9, such as gallstones, cholangitis, or hepatitis, and with bilirubin levels within normal limits, a decision had to be made whether to change chemotherapy, as rising CA 19-9 levels usually indicate disease progression. However, the patient reported no abdominal pain and felt generally better, despite the increased CA 19-9 levels. He had more energy and regained appetite and body weight. Pseudoprogression was therefore suspected, and the same FOLFOX chemotherapy was continued. After the sixth cycle (three months after initiation), CA 19-9 levels began to decrease. After the seventh cycle, CA 19-9 dropped to 59,265 units/mL and plateaued around 60,000 units/mL (Figure 4). The patient was able to resume activities such as fishing and shared his catch with other cancer patients.
Biochemical pseudoprogression: the CA 19-9 levels continued rising even after four cycles of chemotherapy
Discussion
Pseudoprogression occurs when imaging or biomarker assessments suggest tumor progression, despite stable or improving cancer status [4]. It was first described in glioblastoma patients treated with radiation and temozolomide chemotherapy [7], but is more commonly associated with ICI immunotherapies that can induce inflammatory responses mimicking disease progression [4].
Pseudoprogression has been described in various tumors, primarily melanoma, as well as non-small cell lung cancer, renal cancer, urothelial cancer, and head and neck squamous cell cancer [4-7], with an incidence of about 8.8%, depending on cancer type. However, pseudoprogression has not been documented in pancreatic cancer cases [4-6,8,9].
The molecular mechanism is not fully understood, but immune cell infiltration, cytokine release, and subsequent inflammation may contribute to temporary tumor swelling [4,9]. In experimental pancreatic cancer models, stimulation of tumor-associated stroma has been suggested as a mechanism, making the tumor area appear more prominent [10].
Biochemical pseudoprogression may differ, potentially caused by cancer cell destruction from chemotherapy, releasing tumor markers into the bloodstream. If the tumor marker has a long half-life, levels may remain high, giving the impression of progression, even if the cancer is responding to treatment. However, the half-life of CA 19-9 is relatively short, around one day [11].
Pseudoprogression presents challenges in cancer treatment, complicating assessment of treatment response and potentially leading to premature treatment changes in patients who are actually improving. Conventional imaging may not always distinguish inflammatory changes from tumor growth, though functional magnetic resonance imaging (MRI) and PET may help identify pseudoprogression [12,13]. For instance, 18F-fluciclovine PET has been useful in detecting pseudoprogression in glioblastoma [14], whereas conventional 18F-FDG PET/CT has limitations [15].
Most patients with pseudoprogression have a good performance status and are paucisymptomatic [4]. In our patient, abdominal pain subsided, and physical performance improved, supporting pseudoprogression as a consideration.
Conclusions
This case highlights a rare example of biochemical pseudoprogression in PDAC, where CA 19-9 levels initially increased during FOLFOX chemotherapy, but subsequently declined with ongoing treatment. Clinical improvement, despite rising tumor markers, underscores the importance of interpreting CA 19-9 trends within the broader clinical context to avoid prematurely misclassifying treatment response as true disease progression.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pancreatic cancer: a review JAMA Park W Chawla A O'Reilly EM 85186232620213454708210.1001/jama.2021.13027 PMC 9363152 · doi ↗ · pubmed ↗
- 2FOLFOX as second-line chemotherapy in patients with pretreated metastatic pancreatic cancer from the FIRGEM study BMC Cancer Zaanan A Trouilloud I Markoutsaki T 4411420142492986510.1186/1471-2407-14-441PMC 4075567 · doi ↗ · pubmed ↗
- 3The clinical utility of CA 19-9 in pancreatic adenocarcinoma: diagnostic and prognostic updates Curr Mol Med Poruk KE Gay DZ Brown K 3403511320132333100610.2174/1566524011313030003 PMC 4419808 · doi ↗ · pubmed ↗
- 4Pseudoprogression and hyperprogression as new forms of response to immunotherapy Bio Drugs Frelaut M du Rusquec P de Moura A Le Tourneau C Borcoman E 4634763420203239441510.1007/s 40259-020-00425-y · doi ↗ · pubmed ↗
- 5Dramatic response to pembrolizumab after pseudoprogression in a patient with advanced metastatic castration-resistant prostate cancer IJU Case Rep Kageyama T Soga N Sekito S 442445520223634118110.1002/iju 5.12508 PMC 9626308 · doi ↗ · pubmed ↗
- 6Evaluating for pseudoprogression in colorectal and pancreatic tumors treated with immunotherapy J Immunother Parseghian CM Patnana M Bhosale P 2842914120182966857110.1097/CJI.0000000000000222 PMC 6028046 · doi ↗ · pubmed ↗
- 7Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas Lancet Oncol Brandsma D Stalpers L Taal W Sminia P van den Bent MJ 453461920081845285610.1016/S 1470-2045(08)70125-6 · doi ↗ · pubmed ↗
- 8Pseudoprogression in advanced non-small cell lung cancer treated with combination chemoimmunotherapy: a case report J Med Case Rep Gonugunta AS von Itzstein MS Gerber DE 2891620223587168510.1186/s 13256-022-03485-6PMC 9310470 · doi ↗ · pubmed ↗