Optimizing Venous Thromboembolism Prophylaxis in Achilles Tendon Rupture: A Systematic Review of Current Evidence and Protocol Recommendations
Mohamed Hashem, Mohamed Elbeshbeshy, Mohamed Khalafallah, Yousif A Othman, Ahmed Al-Saqili, Ahmed A Ghobashy

TL;DR
This review examines how to best prevent blood clots in patients with Achilles tendon ruptures, suggesting personalized strategies based on risk levels.
Contribution
The study provides a systematic review and protocol recommendations for VTE prophylaxis tailored to Achilles tendon rupture patients.
Findings
High-risk patients benefit from pharmacological prophylaxis like LMWH or rivaroxaban for at least 28 days.
Low-risk patients can manage VTE risks through early mobilization and mechanical prophylaxis.
Individualized monitoring and risk assessment tools like TRiP(cast) score are crucial for effective prophylaxis.
Abstract
The Achilles tendon plays a vital role in maintaining normal gait and locomotion. The incidence of Achilles tendon rupture (ATR) has been increasing, mainly due to the rising popularity of recreational sports. This review assesses anticoagulation efficacy in preventing venous thromboembolism (VTEs) during ATR treatment and aims to establish an evidence-based prophylaxis protocol. Initially, a comprehensive search across PubMed, Scopus, Web of Science (WoS), and the Cochrane Library databases, and the citation analysis identified studies on VTE prophylaxis in patients with acute or chronic ATR. We summarized results qualitatively, focusing on VTE prevention, complications, and clinical outcomes while considering study quality, bias, and confounders in our analysis. Eight studies, involving 1199 patients with ATR, were analyzed for the efficacy of various VTE prophylaxis strategies. Risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
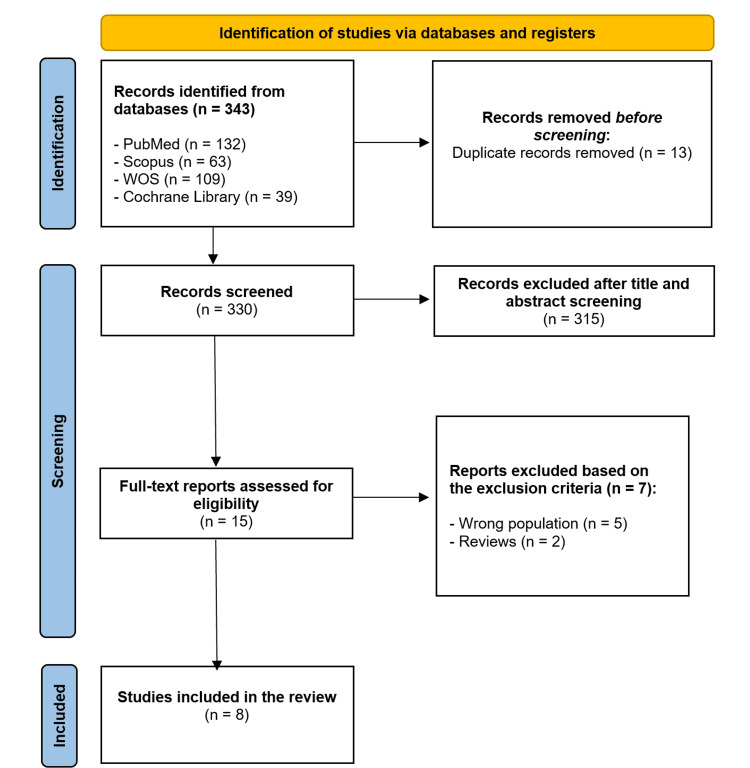 Figure 1
Figure 1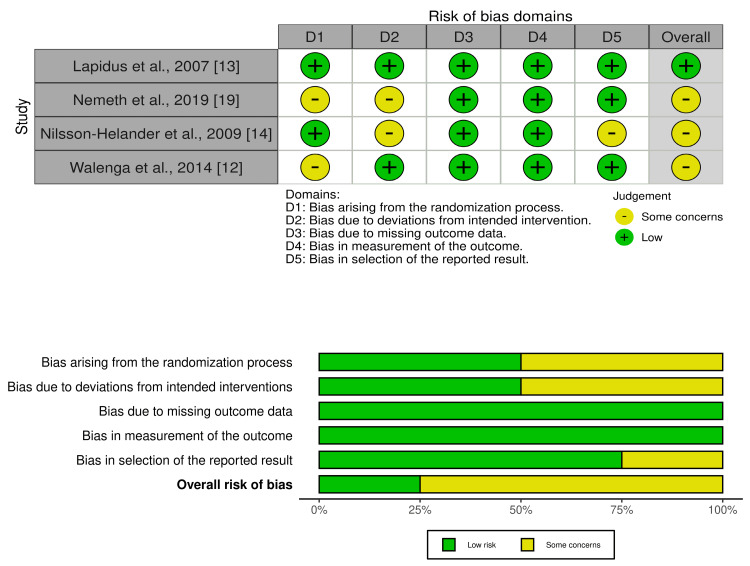 Figure 2
Figure 2| Author, year published | Design | Country | ATR Population | Prophylactic anticoagulation, Duration | No of ATR | Follow-up Duration | VTE risk (incidence/group size) | VTE screening | Findings |
| Blanco et al., 2017 [ | Prospective cohort study | UK | ATR managed with a functional walker boot protocol and FWB for eight weeks. | LMWH (dalteparin) until the end of immobilization | 283 | Six weeks | 4.9% (14/283) | Symptomatic only | Low overall incidence of VTE in foot and ankle trauma (3.5%). No statistically significant difference in VTE incidence among the ATR group compared to surgically or conservatively managed ankle fracture groups (4.9% vs. 3% vs. 2.2% respectively; p=.197). However, VTE occurred significantly earlier following acute ATR vs. ankle fractures (16.1 vs. 35.5 days, p=.002). VTE incidence in high-risk patients despite receiving LMWH varied between 33% (one in three high-risk patients) in the ATR group, 14.3% (1/7) in the CAF group, and 0% (0/4) in the SAF group. |
| Çolak et al., 2020 [ | Retrospective cohort study | Turkey | Surgically managed ATR | LMWH (enoxaparin, 4000 U) for 20 days postoperatively | 238 | 12 weeks | 9.2% (22/238) | Symptomatic only | 18 DVTs and four PEs. Risk factors were age >40 years and BMI >30 kg/m2. Hence, the recommendation for routine VTE prophylaxis in acute ATR. |
| Lapidus et al., 2007 [ | RCT | Sweden | Surgically repaired ATR – postoperative: a) Placebo | Six weeks postoperatively (both groups) | 91 | Six weeks | 36% (16/44) | Duplex US at three and six weeks for all patients | High incidence of VTE following surgical repair of ATR. VTE prophylaxis using dalteparin was not statistically protective compared to placebo (p=.8). |
| b) LMWH (dalteparin 5000 U) | 34% (16/47) | ||||||||
| Lee et al., 2023 [ | Retrospective cohort study | UK | Patients ≥18 years old with acute ATR: a) EWB | LMWH (Tinzaparin) for four weeks (both groups) | 296 | Nine weeks | 1.3% (2/69) | Symptomatic only | Relatively lower VTE incidence in EWB vs. NWB groups, but was not statistically significant (p=.33). |
| b) NWB | 2.9% (3/227) | ||||||||
| Nemeth et al., 2019 [ | Validation RCT | Netherlands | Acute ATR: a) Surgical repair | LMWH (nadroparin or dalteparin) till the end of immobilization | 94 | 12 weeks | 19% (4/21) | Symptomatic only | The relative risk of VTE following surgical repair versus conservative treatment was 3.45. In an adjusted analysis, the relative risk was 8.2 (95% CI: 2.8–24.1). |
| b) Cast immobilization | 5.5% (4/73) | ||||||||
| Nilsson-Helander et al., 2009 [ | RCT | Sweden | Unilateral ATR in patients 16–65 years old if randomisation and treatment were started within 72 hours from the initial injury: a) Surgically-managed | Macrodex | 95 | Eight weeks | 28.6% (14/49) | Duplex US at eight weeks for all patients | High overall VTE incidence of 34% (32/95) with no statistically significant difference between the groups (p=.217). Three of the 32 patients experienced non-fatal PE in addition to DVTs. In the higher risk subgroup (n=7), prophylactic anticoagulation (dalteparin) resulted in a lower VTE incidence of 14% (one VTE event in the seven patients). |
| b) Non-surgical in a below-knee cast for two weeks, followed by a functional brace for 6 weeks. | LMWH (based on surgeon’s preference) | 39.1% (18/46) | |||||||
| Saragas et al., 2017 [ | Prospective cohort study | South Africa | ATR repair followed by NWB in a below-knee cast for ≥ 4 weeks in patients >18 years old | Rivaroxaban 10 mg OD for 4 weeks | 28 | One year | 3.6% (1/28) | Symptomatic only | The only incident occurred at five weeks; however, the patient admitted to being non-compliant with taking his rivaroxaban. |
| Walenga et al., 2014 [ | Validation study of a previous RCT | Denmark | ATR requiring functional (ambulatory) immobilization in a plaster cast or brace | LMWH (reviparin) vs placebo for 5-6 weeks | 74 | 35-42 days | 12.2% (9/74) | Ascending phlebography at the time of brace removal in all patients | Six events in the placebo group vs. three events in the reviparin group |
| Author, year published | Groups | Participants (N) | Mean age, years (SD) | Male, n (%) | Body mass index, kg/m2 (SD) | Smoking, n (%) | Diabetes mellitus, n (%) | History of venous thromboembolism, n (%) | Side rupture, n (%) | |
| Right | Left | |||||||||
| Lapidus et al., 2007 [ | LMWH dalteparin | 52 | 37 (8) | 41 (79) | 26 (3) | 9 (17.31) | 0 | 0 | NA | NA |
| Placebo | 53 | 42 (9) | 42 (79) | 26 (3) | 8 (15.09) | 0 | 0 | NA | NA | |
| Nemeth et al., 2019 [ | LMWH | 719 | 46.5 (16.5) | 347 (48.3) | 26.0 (4.4) | 188 (28.4) | NA | NA | NA | NA |
| No treatment | 716 | 45.6 (16.4) | 369 (51.5) | 25.7 (4.4) | 178 (24.9) | NA | NA | NA | NA | |
| Nilsson-Helander et al., 2009 [ | ATR, Marcodex or LMWH | 95 | 42.25 (7.86) | 79 (83.15) | NA | NA | 0 | NA | NA | NA |
| Walenga et al., 2014 [ | LMWH (reviparin) | 217 | 46.33 (13.43) | 112 (52) | 25.33 (3.73) | 79 (36) | 5 (2) | 5 (2) | NA | NA |
| Placebo | 221 | 46.67 (14.18) | 114 (52) | 26 (2.98) | 103 (47) | 5 (2) | 5 (2) | NA | NA | |
| Author, year published | Groups | Participant (N) | Mean age, years (SD) | Male, n (%) | Body mass index, kg/m2 (SD) | Smoking, n (%) | Diabetes mellitus, n (%) | History of venous thromboembolism, n (%) | Side rupture, n (%) | |
| Right | Left | |||||||||
| Lapidus et al., 2007 [ | LMWH dalteparin | 52 | 37 (8) | 41 (79) | 26 (3) | 9 (17.31) | 0 | 0 | NA | NA |
| Placebo | 53 | 42 (9) | 42 (79) | 26 (3) | 8 (15.09) | 0 | 0 | NA | NA | |
| Nemeth et al., 2019 [ | LMWH | 719 | 46.5 (16.5) | 347 (48.3) | 26.0 (4.4) | 188 (28.4) | NA | NA | NA | NA |
| No treatment | 716 | 45.6 (16.4) | 369 (51.5) | 25.7 (4.4) | 178 (24.9) | NA | NA | NA | NA | |
| Nilsson-Helander et al., 2009 [ | ATR, Marcodex or LMWH | 95 | 42.25 (7.86) | 79 (83.15) | NA | NA | 0 | NA | NA | NA |
| Walenga et al., 2014 [ | LMWH (reviparin) | 217 | 46.33 (13.43) | 112 (52) | 25.33 (3.73) | 79 (36) | 5 (2) | 5 (2) | NA | NA |
| Placebo | 221 | 46.67 (14.18) | 114 (52) | 26 (2.98) | 103 (47) | 5 (2) | 5 (2) | NA | NA | |
| Author, year published | Groups | Participant (N) | Mean age, years (SD) | Male, n (%) | Body mass index, kg/m2 (SD) | Use of steroids, n (%) | Smoking, n (%) | Diabetes mellitus, n (%) | History of venous thromboembolism, n (%) | Side rupture, n (%) | |
| Right | Left | ||||||||||
| Saragas et al., 2017 [ | Hindfoot arthrodesis | 22 | 50.9 (11.542) | 75 (52.82) | 29 (7.363) | NA | 14 (9.9) | NA | 0 | NA | NA |
| Mid-foot arthrodesis | 19 | ||||||||||
| Acquired flat-foot correction | 18 | ||||||||||
| Achilles tendon rupture repair | 17 | ||||||||||
| Ankle arthrodesis + tibiotalocalcaneal arthrodesis | 16 | ||||||||||
| Achilles tendon debridement and repair | 11 | ||||||||||
| Tendon (other than Achilles tendon) debridement/repair | 7 | ||||||||||
| Total ankle replacement | 7 | ||||||||||
| Lateral ligament reconstruction | 5 | ||||||||||
| Dwyer calcaneal osteotomy | 4 | ||||||||||
| Ankle fracture ORIF | 4 | ||||||||||
| OATS | 2 | ||||||||||
| Lisfranc ORIF | 2 | ||||||||||
| Jones fracture ORIF | 2 | ||||||||||
| Gastrocnemius recession | 2 | ||||||||||
| Dislocating peroneal tendons | 2 | ||||||||||
| Tendon transfers | 1 | ||||||||||
| Non-union tibia (revision) | 1 | ||||||||||
| Author, year published | Selection | Comparability | Outcomes | Total scores | |
| Blanco et al., 2017 [ | 4 | 2 | 3 | 9 - Good | |
| Colak et al., 2020 [ | 3 | 2 | 3 | 8 - Good | |
| Lee et al., 2023 [ | 4 | 2 | 2 | 8 - Good | |
| Saragas et al., 2017 [ | 2 | 0 | 2 | 4 - Fair | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Tendon Structure and Treatment · Diagnosis and Treatment of Venous Diseases
Introduction and background
The Achilles tendon is the largest and most robust tendon in the human body. It connects the calf muscles to the calcaneus bone and plays a crucial role in locomotion, including walking, running, jumping, and ascending stairs [1].
The incidence of Achilles tendon injury has been increasing, mainly due to the rising popularity of recreational sports, which has led to a higher prevalence of Achilles tendon rupture (ATR). The overall incidence of ATR in the general population is approximately 31 cases per 100,000 individuals annually, though this rate may be higher in specific populations and regions [2]. The male-to-female incidence ratio is approximately 5.5:1, with over 80% of ruptures occurring during recreational sports [3].
Management options for ATR include surgical intervention followed by immobilization with a brace or plaster cast, as well as conservative treatment involving immobilization alone [4-6]. A significant complication associated with ATR treatment is venous thromboembolism (VTE), a well-documented cause of morbidity and mortality in lower limb surgery and prolonged immobilization [4,7,8]. VTEs account for about 10% of all hospital deaths [8,9]. Reported rates of deep vein thrombosis (DVT) following ATR treatment range from 0.43% to 34%, while pulmonary embolism (PE) rates vary from 0% to 3% [10,11].
Previous studies have suggested the use of low molecular weight heparin (LMWH) as prophylaxis to reduce the incidence of VTE events following temporary lower limb immobilization [6,12]. However, findings across studies have been inconsistent, and there is currently no consensus on the necessity or efficacy of prophylactic therapy following ATR, especially in the lower risk group [4,7,13,14].
Therefore, this systematic review aims to evaluate the efficacy and safety of anticoagulation therapy in preventing VTEs in patients undergoing ATR treatment and to establish an evidence-based protocol for using prophylactic anticoagulants in patients with ATR.
Review
Methods
This systematic review was conducted by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [15]. The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD420251108036).
Literature Search and Study Selection
A comprehensive literature search was performed across multiple databases, including PubMed, Scopus, Web of Science (WoS), and the Cochrane Library, to identify relevant studies published within the past 20 years. A tailored search strategy was developed for each database, as detailed in Appendix A. Duplicate records were removed using EndNote (Clarivate, Philadelphia, PA) [16], and both prospective and retrospective citation analyses were conducted through manual searches.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (a) involved patients diagnosed with acute or chronic ATR; (b) reported on VTE prophylaxis strategies and associated clinical outcomes; (c) consisted of clinical trials or well-designed observational studies; and (d) were published in English with full-text availability. Studies were excluded if they met any of the following criteria: (a) published in languages other than English; (b) assessed as low quality based on study design or methodological limitations; or (c) consisted of cross-sectional studies, case series, case reports, review articles, cadaveric studies, or conference abstracts.
Study Selection Process
We conducted the study selection in two stages. First, we screened titles and abstracts, and then we evaluated full texts for eligibility. Two reviewers performed each stage independently and resolved any disagreements through discussion with the supervising author.
Data Extraction
Data extraction was performed independently by two authors using standardized spreadsheets. The following variables were collected from each included study: study design, country of study, population characteristics, VTE prophylaxis regimen, total sample size, follow-up duration, key findings, mean age, proportion of male participants, body mass index (BMI), smoking status, prevalence of diabetes mellitus, history of VTE, and site of rupture.
Quality Assessment
The risk of bias for each included study was assessed by two independent reviewers using appropriate tools based on the study design. Randomized controlled trials (RCTs) were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool [17]. Cohort studies were assessed using the Newcastle-Ottawa Scale (NOS) [18]. Any disagreements in quality assessment were resolved through discussion between the reviewers or by the senior author.
Narrative Synthesis
A narrative synthesis was conducted to integrate and interpret the findings from the included studies. The synthesis followed a structured approach, evaluating study characteristics, methodological quality, and primary outcome measures. Findings were grouped based on study design, patient demographics, and the type of VTE prophylaxis implemented. Patterns, similarities, and differences across studies were identified to provide a comprehensive overview of the current evidence. Where applicable, results were qualitatively summarized, with emphasis on trends in VTE prevention strategies, complication rates, and clinical outcomes. The synthesis considered study quality, potential biases, and confounding factors. Notable differences among studies (such as variations in follow-up duration, intervention methods, and patient populations) were also highlighted.
Results
The initial search retrieved 343 studies. After removing 13 duplicates, we screened the titles and abstracts of 330 studies. Then, we excluded 315 articles, and only 15 studies were screened for eligibility. Finally, we included eight studies consisting of four clinical trials and four cohort studies (Figure 1).
A PRISMA flowchart of the study selection processPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WoS: Web of Science
Characteristics of the Included Studies
The included studies encompassed a total of 4,701 patients, of whom 1,199 were diagnosed with ATR. The studies were conducted across various countries, including the United Kingdom, Turkey, and South Africa. Follow-up durations ranged from 35 days to 12 months. A range of prophylactic anticoagulation regimens was employed, including LMWH formulations such as dalteparin, tinzaparin, nadroparin, and reviparin, as well as rivaroxaban and macrodex (Tables 1-4).
Risk of Bias Assessment
Regarding the RCTs, one study had a low risk of bias [13], and the other three studies were rated as "some concerns" (Figure 2) [12,14,19].
Risk of bias assessment of the included RCTsRCTs: randomized controlled trials
The four included non-randomised studies were classified as illustrated in Table 5.
Discussion
This systematic review synthesized data from eight studies evaluating VTE prophylaxis in patients with ATR, spanning both surgical and non-surgical management. The studies varied in design, pharmacologic agents, duration of treatment, and patient populations, which limits direct comparability but provides a comprehensive view of current prophylactic strategies and their outcomes.
Prophylactic Agent Efficacy
LMWH was the most commonly studied pharmacologic agent. Blanco et al. [4] and Lee et al. [7] reported low VTE incidences of 4.9% and 1.7%, respectively, with LMWH prophylaxis administered for 28 days or during immobilization, with no significant bleeding complications noted. Similarly, Walenga et al. [12] reported an overall VTE risk of 12% (nine VTEs in 74 ATR patients). Among them, three (33.3%) were in the reviparin group vs. six (66.7%) in the placebo cohort, suggesting a possible reduction in events with LMWH.
In contrast, Lapidus et al. [13] and Nilsson-Helander et al. [14] found no significant difference in VTE incidence between dalteparin and placebo groups (approximately 34% vs. 36%), raising questions about the routine use of LMWH for all ATR patients. Likewise, Nemeth et al. [19] reported no statistically significant benefit of LMWH in preventing VTE among cast-immobilized or surgically repaired ATR patients, further questioning its utility in low-risk or non-surgical cases.
Saragas et al. [20] evaluated rivaroxaban in 28 post-surgical ATR patients. They reported only one symptomatic VTE (3.6%) occurring in a patient who admitted non-compliance, suggesting favorable outcomes with direct oral anticoagulants (DOACs) if adherence is maintained.
Duration of Prophylaxis
Prophylaxis duration varied across studies from 20 days to six weeks. Blanco et al. [4], Lee et al. [7], and Walenga et al. [12] administered LMWH or reviparin for 28-42 days, reporting reduced VTE rates. Similarly, Saragas et al. [20] employed rivaroxaban for four to six weeks with a low VTE incidence. However, Nemeth et al. [19] used a 28-day LMWH regimen, and Çolak et al. [6] used a 20-day enoxaparin regimen but still reported an 8.5% and 9.1% VTE rate, respectively, suggesting that duration alone may be insufficient without appropriate risk stratification. Nilsson-Helander et al. [14] left prophylaxis duration to the surgeon’s discretion, which may have contributed to inconsistent outcomes.
Risk Factors and Surgical Impact
Surgical intervention and prolonged immobilization were consistently associated with higher VTE risk. Nemeth et al. [19] identified surgical repair as conferring an 8.2-fold increased VTE risk (relative risk (RR) 8.2). Nilsson-Helander et al. [14] reported a 34% VTE rate in surgically treated patients; however, the difference was not statistically significant compared to the non-surgically managed group. Çolak et al. [6] observed a 9.1% postoperative VTE rate despite LMWH prophylaxis. Conversely, Blanco et al. [4] and Lee et al. [7] emphasized the importance of risk stratification and early weight-bearing protocols, respectively, to reduce VTE incidence.
Safety and Monitoring
Across all studies, bleeding complications were rare. Lapidus et al. [13], Blanco et al. [4], and Nemeth et al. [19] found no significant bleeding or heparin-induced thrombocytopenia. Nilsson-Helander et al. [14] noted non-thrombotic complications related primarily to surgery, such as wound infection. Saragas et al. [20] and Çolak et al. [6] reported no major adverse events, supporting the general safety of anticoagulants when appropriately selected and monitored.
VTE Prophylaxis Protocol for Patients With ATR
Based on current evidence, a structured, individualized approach to VTE prophylaxis is recommended for patients with ATR, incorporating risk stratification, agent selection, duration of therapy, and ongoing monitoring.
Step 1: initial assessment and risk stratification: Clinicians should use a validated prediction model for VTE risk, such as the Thrombosis Risk Prediction Following Cast Immobilization (TRiP(cast)) score, in patients with lower limb immobilization [21,22]. A score ≥7 identifies high-risk patients warranting pharmacologic prophylaxis. ATR automatically confers 3 points due to its classification as high-risk trauma. This is supported by Calder et al. [23] findings that both surgically and conservatively managed ATRs conferred a higher clinical and radiological VTE risk compared to other isolated foot and ankle injuries. Additional risk factors in the TRiP(cast) score include age >35 years, male sex, BMI >25 kg/m^2^, personal or first-degree family history of VTE, recent surgery or immobilization, hormonal therapy, malignancy, pregnancy or puerperium, and comorbidities such as congestive heart failure (CHF), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), rheumatoid arthritis, and varicose veins [21,22].
Step 2: prophylactic agent selection: For high-risk or surgical patients, LMWH (including enoxaparin, dalteparin, and reviparin) remains the most commonly used agent [4,6,7,12]. Rivaroxaban, an oral direct anticoagulant, can be an alternative for patients preferring oral therapy, provided adherence is ensured [20]. In low-risk patients, evidence remains inconclusive due to the high overall VTE incidence rates following ATR, with some studies reporting a substantial reduction in VTE risk with LMWH compared to placebo [6,12]. However, most studies do not support routine pharmacologic prophylaxis. Lapidus et al. [13] and Nilsson-Helander et al. [14] found no significant reduction in VTE risk with LMWH in this group. Instead, they advocated for early mobilization, weight-bearing protocols, and mechanical prophylaxis when mobility is limited, which aligns with the general lower limb immobilization findings by Douillet et al. [22]. Hence, a personalized shared decision-making approach is required in these cases.
Step 3: duration of prophylaxis: A minimum of 28 days of prophylaxis is advised in high-risk or surgically treated patients [4,7,12]. Some evidence supports extending prophylaxis up to six weeks depending on individual risk [14,20]. Building on Douillet et al.'s [22] general findings on lower limb immobilization, there is no clear benefit for prophylaxis beyond the immobilization period in low-risk patients.
Conclusions
This review supports a risk-stratified, individualized approach to VTE prophylaxis in ATR patients. Utilization of standardized risk assessment tools such as TRiP(cast) score, alongside careful consideration of patient-specific factors, is essential to optimize outcomes while avoiding unnecessary treatment. Pharmacologic prophylaxis is indicated in high-risk patients, particularly post-surgical cases or those with multiple VTE risk factors. For low-risk patients, the benefit of LMWH or DOACs remains uncertain and inconsistently demonstrated across studies. In these patients, early mobilization, patient education, and mechanical prophylaxis may offer a safe alternative similar to the general population of lower-limb immobilized patients. Future high-quality prospective trials are needed to clarify prophylaxis efficacy, especially in the lower-risk ATR populations, and to evaluate the long-term safety of emerging agents like DOACs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anatomy, Bony Pelvis and Lower Limb: Achilles Tendon Stat Pearls [Internet] Wong M Jardaly AH Kiel J 2025 Treasure Island, FL Stat Pearls [Internet], Stat Pearls Publishing Treasure Island 2025 https://www.ncbi.nlm.nih.gov/books/NBK 499917/29763092 · pubmed ↗
- 2Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients Knee Surg Sports Traumatol Arthrosc Ganestam A Kallemose T Troelsen A Barfod KW 373037372420162569728410.1007/s 00167-015-3544-5 · doi ↗ · pubmed ↗
- 3Incidence of Achilles tendon rupture Acta Orthop Scand Leppilahti J Puranen J Orava S 277279671996868646810.3109/17453679608994688 · doi ↗ · pubmed ↗
- 4A prospective cohort study of symptomatic venous thromboembolic events in foot and ankle trauma: the need for stratification in thromboprophylaxis?J Foot Ankle Surg Blanco JA Slater G Mangwani J 4844885720182950313510.1053/j.jfas.2017.10.036 · doi ↗ · pubmed ↗
- 5Comparison of fondaparinux with low molecular weight heparin for venous thromboembolism prevention in patients requiring rigid or semi-rigid immobilization for isolated non-surgical below-knee injury J Thromb Haemost Samama CM Lecoules N Kierzek G 183318431120132396518110.1111/jth.12395 · doi ↗ · pubmed ↗
- 6Incidence of venous thromboembolism after Achilles tendon surgery in patients receiving thromboprophlaxis J Am Podiatr Med Assoc Çolakİ Gülabi D Eceviz E Çevik BH Bulut G Bekler HI 0110202010.7547/17-01229131653 · doi ↗ · pubmed ↗
- 7Thromboembolic events during weightbearing vs nonweightbearing accelerated rehabilitation protocols for complete Achilles tendon ruptures Foot Ankle Orthop Lee C Haarer F Titheradge R Iliopoulos E 24730114231178791820233733263010.1177/24730114231178791 PMC 10272654 · doi ↗ · pubmed ↗
- 8The impact of risk assessment on the implementation of venous thromboembolism prophylaxis in foot and ankle surgery Foot Ankle Surg Saragas NP Ferrao PN Saragas E Jacobson BF 85892020142479682410.1016/j.fas.2013.11.002 · doi ↗ · pubmed ↗