Return rates for the use of ovarian tissue cryopreserved prior to gonadotoxic treatment as fertility preservation: a systematic review
Anna Mathilde Yde, Lotte Berdiin Colmorn, Amalie Somuncu Johansen, Elisabeth Clare Larsen, Anja Pinborg, Kirsten Tryde Macklon

TL;DR
This study finds that only a small percentage of women who freeze their ovarian tissue before fertility-threatening treatments later use it for fertility restoration.
Contribution
The study provides a systematic review of return rates for ovarian tissue cryopreservation, highlighting the low utilization and the need for better patient selection criteria.
Findings
Most studies report return rates of ≤5% for ovarian tissue cryopreservation use.
Only one study reported a return rate of 14%, indicating generally low utilization.
The overall evidence quality was moderate, with limited follow-up time potentially biasing results.
Abstract
What is the return rate for the use of ovarian tissue cryopreserved for fertility preservation prior to gonadotoxic treatment? The return rate for the use of ovarian tissue cryopreserved for fertility preservation prior to gonadotoxic treatment is modest, with most studies reporting rates of ≤5%. A considerable number of years have passed since ovarian tissue cryopreservation (OTC) was first implemented for fertility preservation, and many studies now provide long-term follow-up data, including return rates. This allows for a more comprehensive evaluation of OTC as a fertility preservation option and of the characteristics of the population to whom it is offered. We searched PubMed, EMBASE, and the Cochrane Library for MeSH words, Emtree terms, and text words related to return rates for the use of ovarian tissue cryopreserved prior to gonadotoxic treatment up to March 2025, in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
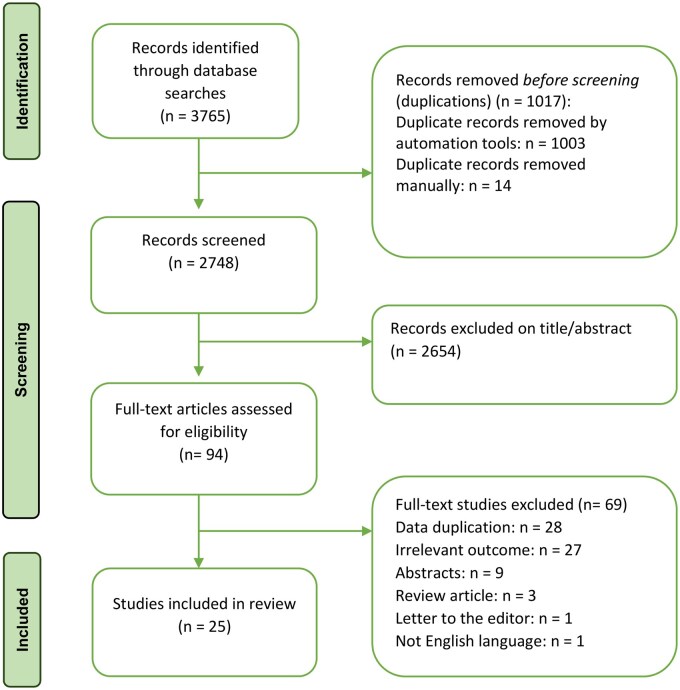 Figure 1
Figure 1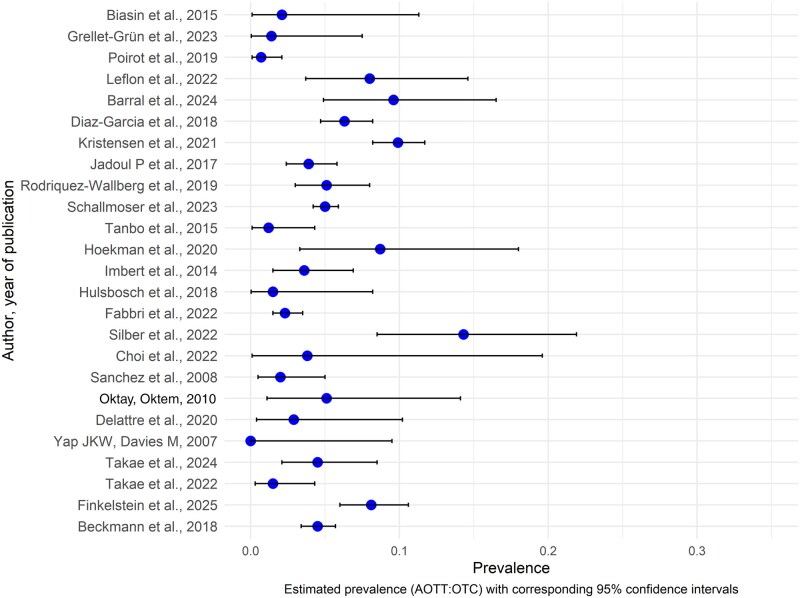 Figure 2
Figure 2| Author, year, country, title | Study design, cohort | Follow-up (FU) time | Indications for fertility preservation | Review outcomes | Comments |
|---|---|---|---|---|---|
|
Italy ‘Ovarian tissue cryopreservation in girls undergoing hematopoietic stem cell transplant: Experience of a single center’ |
Pre-pubertal: n=24 (51%) Pubertal: n=23 (49%)
|
|
|
| |
|
France ‘A 16-year biocentric retrospective analysis of ovarian tissue cryopreservation in pediatric units: indications, results, and outcome’ |
Pre-pubertal: n=51 Post-pubertal: n=21
|
|
nonmalignant disease: 21 (29.1%) (Hemoglobinopathies n=15 (21%), other non-malignant diseases n=6 (8%)).
|
| |
|
France ‘Ovarian tissue cryopreservation for fertility preservation in 418 girls and adolescents up to 15 years of age facing highly gonadotoxic treatment. Twenty years of experience at a single center’ |
median age 6.9 years (range 0.3–15 years) <10 years: n=278 (66.5%) <5 years: n=150 (35.9%)
|
|
non-malignant diseases: n=105 (25.2%) (hemoglobinopathies n=71 (68.9%)).
restore fertility: n=2 |
| Return rate for only those alive and 18 years or older at EOF: 3:149=2.2% |
|
France ‘Experience, and gynecological and reproductive health follow-up of young adult women who have undergone ovarian tissue cryopreservation’ |
|
|
|
| 11 patients (9.7%) requested AOTT |
|
Spain ‘Current status of fertility preservation in a Spanish tertiary public hospital: multidisciplinary approach and experience in over 1500 patients’ |
|
|
|
| |
|
Spain ‘Oocyte vitrification versus ovarian cortex transplantation in fertility preservation for adult women undergoing gonadotoxic treatments: a prospective cohort study’ |
|
|
seeking pregnancy: n=44 (88%) endocrine purposes: n=6 (12%) |
| |
|
Denmark ‘Use of cryopreserved ovarian tissue in the Danish fertility preservation cohort’ |
≤18 years: n=242 (21%) 19–34 years: n=833 (70%) ≥35: n=111 (9%) Subgroup 1: 24.6 years (±9 years)
deceased total number: n=142 (12%) deceased subgroup 1: n=135 (18%) donated tissue for science: n=72 (6%) |
Mean FU time in subgroup 1 was 10.9 years, minimum 5 years |
benign indications, 12%: benign hematological diseases (5%), systemic diseases (rheumatologic and autoimmune disease (3%)), genetic diseases (2%).
restore hormone production: n=10 induce puberty: n=1 |
|
Subgroup 1: >5 years FU Subgroup 2: alive and aged >24 years in July 2020 |
|
Belgium ‘Efficacy of ovarian tissue cryopreservation for fertility preservation: lessons learned from 545 cases’ |
mean age 22.3±8.8 years (range 6 months–39 years) ≤18 years: n=157 (29%) prepubertal: n=80 (15%) >18 to ≤35: n=388 (71%)
deceased: n=54 (10%) |
|
|
| 24 (4.4%) patients requested AOTT |
|
Sweden ‘A prospective study of women and girls undergoing fertility preservation due to oncologic and non-oncologic indications in Sweden-Trends in patients’ choices and benefit of the chosen methods after long-term follow up’ |
adults: n=1076 children: n=178
adult women, n=221: mean age 28.1 years (range 18–39 years) post-pubertal teenagers, n=66: mean age 15.6 years (range 14–17 years) pre-pubertal, n=48: mean age 11.2 years (range 3–13 years)
deceased: n=97:1254 (7.7%) emigrated: n=18:1254 (1.4%) |
|
malignant diseases: n=852 benign diseases: n=402
|
| Utilization rate was calculated as the number of patients who returned for AOTT out of all patients aged 18–40 years who had undergone FP, and were alive and living in Sweden at least 1 year following FP |
|
Germany ‘Cryostorage of human ovarian tissue: evaluating the storage and disposal pattern over a 22-year period in 2475 patients’ |
|
≥5 years active storage: n=661 (median storage duration 7.4 years) (range 5–16.3 years) ≥10 years active storage: n=148 (median storage duration 11.9 years) (range 10–16.3 years) Ended storage: n=1155 (median storage duration 3.8 years) (range 0–19.1 years) |
non-specified: 165 (6.7%))
|
| Of the 124 AOTT 29 (1.17%) were performed on site and 95 (3.83%) were outsourced for scheduled transplantation at other sites. |
|
Norway ‘Autotransplantation of cryopreserved ovarian tissue after treatment for malignant disease—the first Norwegian results’ |
|
|
|
| 6:162 patients (3.6%) requested AOTT (1 patient conceived spontaneously immediately before AOTT; 1 patient was diagnosed with BRCA1 and BRCA2 gene mutations, and had a family history of several BRCA related cancers, and was therefore advised against AOTT; 1 patient had leukemia-specific gene re-arrangements (IgH and TCRD/A) in the cryopreserved ovarian tissue; 1 patient treated for diffuse natural killer cell lymphoma was under assessment for AOTT at the time of the study) |
|
Netherlands ‘Ovarian tissue cryopreservation: Low usage rates and high live-birth rate after transplantation’ |
mean age 24 years (range 10.2–35.7 years) <18 years: n=19 ≥18: n=50
|
|
benign indications: n=13 (18.9%)
|
| |
|
Belgium ‘Safety and usefulness of cryopreservation of ovarian tissue to preserve fertility: a 12-year retrospective analysis’ |
aged 0.8–17 years: n=45 (20%) aged ≥18 years: n=180 (80%)
|
|
prepubertal (n=27): hematological benign diseases (58%), lymphoma (4%), leukemia (27%), solid tumor (7%), immunological diseases (4%) post-pubertal (n=198): breast cancer (43%), lymphoma (22%), leukemia (6%), ovarian borderline tumor (8%), solid tumor (7%), pelvic tumor (8%), immunological disease (5%), hematological benign disease (1%)
|
| |
|
Belgium ‘A real-life Analysis of Reproductive Outcome after Fertility Preservation in Female Cancer Patients’ |
|
|
|
| |
|
Italy ‘Ovarian tissue cryopreservation and transplantation: 20 years experience in Bologna University’ |
≤17 years: 238 (23.2%) (group 1) 18–38 years: 788 (76.8%) (group 2) mean age ±SD: group 1: 12.9 ± 4.14 group 2: 28.0 ± 5.7
|
|
non-malignant diseases: n=96 (9%) (genetic diseases: n=52, autoimmune diseases: n=17, others: n=27)
restore-and or improve ovarian function and seek pregnancy: n=20 restore steroidogenesis: n=4 |
| |
|
USA ‘ |
|
|
cancer: n=85 premature ovarian failure: n=8 social reasons: n=13 others (turner syndrome, endometriosis, MS, aplastic anemia, massive ovarian bilateral teratoma or a daughter born with no ovary)
|
| The 17 recipients were between 18 and 31 years at OTC (median age of 24 years) |
|
Korea ‘The experience of Fertility Preservation in a Single Tertiary Center in Korea’ |
|
|
|
| |
|
Valencia ‘The Valencia Programme for Fertility Preservation’ |
|
|
other malignant or non-malignant diseases: 20% (colorectal carcinoma, sarcoma, glomerulonephritis, cancer, lupus, other)
|
| |
|
USA ‘Ovarian cryopreservation and transplantation for fertility preservation for medical indications: report of an ongoing experience’ |
0–18 years: 19% 19–29 years: 42% 30–39 years: 31% 40–44 years: 8%
|
|
|
| |
|
Belgium ‘Combining fertility preservation procedures to spread the eggs across different baskets: a feasibility study’ |
prepubertal: n=13 OTC (n=4) mean age ±SD: 5.5 years (±7.1) OTC + OTO–IVM (n=9) mean age ±SD: 5.1 years (± 3.6) post-pubertal: n=55 OTC + OTO–IVM (n=24) mean age ±SD: 27.9 years (±6.6) OPU–IVM + OTC + OTO–IVM (n=17) mean age ±SD: 25.9 years (± 4.8) OTC + OTO–IVM COS (n=13) mean age ± SD: 26.2 years (± 4.3)
|
|
|
| |
|
UK ‘Fertility preservation in female cancer survivors’ |
|
|
|
| |
|
Japan ‘Survey on the implementation status and reproductive outcomes of oocyte and ovarian tissue cryopreservation in Japan: Historical comparison with nationwide surveys’ |
|
|
|
| Survey targeting 51 facilities, response rate of 43:51 (84.3%). OTC was performed in 18 facilities |
|
Japan ‘A practical survery of fertility preservation treatments in the startup phase in Japan’ |
<10: n=3 11–15: n=23 16–20: n=17 21–25: n=26 26–30: n=37 31–35: n=57 36–40: n=33 41–45: n=4 46–50: n=1 <15 years: 12.9%
|
|
|
| 100% survey response rate from 30 facilities that performed OTC |
|
Australia ‘Pregnancy outcomes following ovarian tissue cryopreservation: an Australian cohort study’ |
|
|
non-transplant: solid tumor cancer 275:545 (50.5%), hematological cancer 171:545 (31.4%), autoimmune disorder 24:545 (4.4%), benign gynecological disorder 21:545 (3.9%), other benign disease 21:545 (3.9%), other cancer 21:545 (3.9%), genetic disorder 8:545 (1.5%), donor 3:545 (0.6%), not reported 1:545 (0.2%)
|
| |
|
FertiProtekt (Germany, Austria, Switzerland) ‘Fertility protection: complications of surgery and results of removal and transplantation of ovarian tissue’ |
|
|
Benign disease: n=85 (6.5%) |
|
- —Independent Research Fund Denmark10.13039/501100004836
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Biology and Fertility · Sperm and Testicular Function · Ovarian function and disorders
Introduction
Gonadotoxic treatment for both malignant and benign conditions, including chemotherapy, radiation therapy, and hematopoietic stem cell transplantation, can damage the ovarian reserve and possibly result in premature ovarian insufficiency (POI) and infertility (Meirow, 2000; Overbeek et al., 2017; van Dorp et al., 2018; Su et al., 2025). While the incidence of cancer among women of reproductive age is increasing, the overall survival rate after cancer is also rising (Nordcan 2.0, 2024). Many women postpone childbearing, and as a result, may not have started or completed their family by the time they receive gonadotoxic treatment (Eurostat, 2025). The risk of treatment-induced infertility is a major concern among these women (Partridge et al., 2004; Peate et al., 2009; Howard-Anderson et al., 2012; Bentsen et al., 2023). The area of reproductive medicine focusing on fertility preservation (FP) prior to gonadotoxic treatment has evolved rapidly during the last few decades, and the number of clinics that guide women and offer FP treatments, including ovarian tissue cryopreservation (OTC), has increased worldwide (Donnez and Dolmans, 2017; Anderson et al., 2020).
Donnez et al. (2004) reported the first live birth after auto-transplantation of cryopreserved ovarian tissue, and OTC has been recognized as an option for FP by the American Society for Reproductive Medicine (ASRM) since 2019 (Practice Committee of the American Society for Reproductive Medicine, 2019). OTC typically involves the removal of an entire ovary or ovarian cortical biopsies under general anesthesia usually via laparoscopic surgery. The excised ovary is then dissected into cortical strips which are cryopreserved (Rosendahl et al., 2011). Slow freezing remains the current standard technique for OTC (Anderson et al., 2017), whereas vitrification is emerging as an alternative approach (Sänger et al., 2024). Autologous ovarian tissue transplantation (AOTT) can be performed in women exhibiting signs of POI following completion of gonadotoxic treatment, with the aim of restoring endocrine function and/or achieving pregnancy, either naturally or through ovarian stimulation and IVF. Live birth rates following AOTT have been reported ranging from 25% to 41% (Colmorn et al., 2022; Lotz et al., 2022; Fraison et al., 2023) with no increased risk of perinatal complications compared with the general population except for preeclampsia (Erden et al., 2024). Even though OTC in many clinics is not the first choice of FP (Rodriguez-Wallberg et al., 2019), it is still considered relevant in premenarchal girls, post-menarche girls considered too young for ovarian stimulation and egg retrieval, and in women who are experiencing time constraints due to the urgency of initiating chemotherapy, and therefore do not have the time to go through ovarian stimulation. Although OTC is generally considered safe with little risk of complications (Beckmann et al., 2018), surgery still carries risks that may delay the initiation of life-saving chemotherapy. Furthermore, a proportion of the women may never develop POI following gonadotoxic treatment, and therefore, the use of costly and potentially risky treatments as a precautionary measure should be carefully evaluated, particularly when it involves removing healthy ovarian tissue, which could potentially reduce the ovarian reserve further. These factors underscore the importance of evaluating return rates.
A considerable number of years have passed since the first ovarian tissue was cryopreserved, and many studies are now able to report long-term follow-up data. This enables evaluation of FP treatment options and the populations to whom they are offered. The aim of this systematic review was to assess the return rates for the use of ovarian tissue cryopreserved as FP prior to gonadotoxic treatment.
Methods
The study was registered in PROSPERO (ID number CRD42024537107). We made no amendment after registration except from using an alternative risk of bias evaluation tool (described below). We used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines in the development of the systematic review (Page et al., 2021).
Information sources and eligibility criteria
We searched PubMed (MEDLINE), EMBASE, and the Cochrane Library using medical subject headings (MeSH), Emtree Terms, and text words. Retrospective and prospective cohort studies, case-control studies, and randomized controlled trials that reported the proportion of women who returned for AOTT out of the total number who underwent OTC prior to gonadotoxic treatment were included. Studies that examined only the return rate for oocyte and/or embryo cryopreservation, and studies that investigated the outcomes from OTC without reporting the proportion of women who returned for AOTT were excluded. Furthermore, we excluded studies in languages other than English, abstracts without full text, letters to the editor, and case series involving fewer than 25 females undergoing OTC. Systematic reviews were screened for relevant references but not included in data extraction.
Search strategy
We developed the search strategy by combining search terms relating to FP, OTC and return rates in collaboration with a health science librarian, who specializes in systematic review searching. No filters or limits were used. The last search was run on 11 March 2025. We manually screened reference lists of selected studies for additional relevant articles. The following search strategy was conducted for the PubMed Search:
(((“Fertility Preservation”[Mesh]) OR (“fertility preser*”[Title/Abstract])) AND (((ovar*[Title/Abstract]) AND (cryopreserv*[Title/Abstract])) OR ((“Cryopreservation”[Mesh]) AND (“Ovary”[Mesh])))) AND (((((((outcome*[Title/Abstract]) OR (“return rate*”[Title/Abstract])) OR (retransplant*[Title/Abstract])) OR (“autologous transplant*”[Title/Abstract])) OR (autotransplant*[Title/Abstract])) OR (transplant*[Title/Abstract])) OR (“Transplantation”[Mesh]))
For additional strategies, see Supplementary Table S1.
Study selection
We imported the search results to Covidence (Veritas Health Innovation, Melbourne, Australia) to facilitate deselection of data duplicates, and the collaboration between reviewers regarding the screening process. Four reviewers took part in the screening process (A.M.Y., L.B.C., A.S.J., and K.T.M.). Each study was evaluated independently by two reviewers who were blinded to each other’s choices. Studies were screened according to relevance regarding the topic, content, and inclusion/exclusion criteria. In case of disagreement between reviewers in any point during the screening process, consensus was reached either through discussion or by consulting a third reviewer. In cases where more than one study was published using the same population or dataset, the most recent publication was included, and the other study/studies were excluded at the full-text screening stage due to ‘data duplication’. The study selection process is depicted in the PRISMA flowchart (Fig. 1).
Flow-chart for the study inclusion in a systematic review on the return rates for the use of cryopreserved ovarian tissue.
Data extraction
A data extraction template was developed and agreed on by all reviewers. Data were extracted by one reviewer (A.M.Y.) and validated by a second reviewer (K.T.M.). From each included study, we extracted the following information: author, year of publication, title, country of publication, study design, and outcome details including the number of females receiving OTC prior to gonadotoxic treatment and the number of women returning for AOTT. When available, we also extracted the following data: age at OTC and AOTT, indication for OTC and AOTT, time interval from OTC to AOTT, follow-up time, proportion of participants aged ≥18 years at the end of follow-up (EOF), and the number of women lost to follow-up and mortality during the study period.
Data synthesis
We performed a synthesis by summarizing the results through text and tables following the Synthesis Without Meta-Analysis (SWiM) in systematic reviews: reporting guideline (Campbell et al., 2020). The outcome metric was the proportion of women who underwent AOTT among those who had their tissue cryopreserved (AOTT:OTC), presented as percentage. We generated a Forest plot (Fig. 2) using the statistical software R (version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria), including all eligible studies, illustrating the prevalence of the utilization rate with 95% CIs. Due to differences between children and adults (indications for OTC, risk of POI following gonadotoxic treatment, and the number of participants who were old enough to undergo AOTT or expressing a desire for pregnancy at the EOF), studies were grouped by age at OTC (children, adults, or both) within Table 1, Supplementary Table S2, and Fig. 2. Due to substantial heterogeneity in study characteristics (age at OTC and AOTT, follow-up time, indications for OTC) we did not perform a meta-analysis, as it would not yield a meaningful summary estimate.
Forest plot of the return rates for the use of ovarian tissue cryopreserved prior to gonadotoxic treatment. Prevalence of women returning for autotransplantation out of those who had their tissue frozen with corresponding 95% CIs.
Risk of bias assessment and quality assessment
We assessed risk of bias for each included study using the Joanna Briggs Institute (JBI) Cohort Checklist. Although most of the included studies primarily investigated outcomes related to FP treatment success (e.g. pregnancy rate), secondary data on the return rate for the use of cryopreserved ovarian tissue were extracted for the purpose of this review. Risk of bias for this outcome was therefore assessed using the JBI Critical Appraisal Checklist for Cohort Studies, which is appropriate for evaluating studies reporting descriptive data on prevalence or return rates (Joanna Briggs Institute, 2020). The overall certainty of evidence was assessed using Grading of Recommendations Assessment, Development, and Evaluation (GRADE), considering risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Results
After screening 2748 studies on title abstract and 94 studies on full text, 25 studies were found eligible for inclusion. The study selection process is depicted in the PRISMA flow chart (Fig. 1). All studies were cohort studies. Supplementary Tables S2 and S3 present the Risk of Bias Assessment according to JBI Critical Appraisal Checklist for Cohort Studies and quality assessment according to GRADE, respectively. Unspecified or insufficient follow-up time was a possible source of bias in all included studies (Supplementary Table S2). Some studies addressed this limitation through sensitivity analyses. For example, Kristensen et al. performed sensitivity analysis by stratifying the population by >5 years of follow-up (subgroup 1) and by >5 years of follow-up, alive and aged >24 years (subgroup 2) (Kristensen et al., 2021). The overall quality of the studies in reporting the return rate for the use of cryopreserved ovarian tissue was moderate (Supplementary Table S3).
Table 1 provides an overview of the study characteristics and outcomes across the 25 included studies. The studies were largely heterogeneous regarding cohort size, time period during which OTC was performed, indication for OTC, age at the time of OTC, and follow-up time.
The number of females undergoing OTC varied substantially across the included studies, ranging from 26 participants in the smallest study (Choi et al., 2022), to 2475 in the largest (Schallmoser et al., 2023). Three studies reported cohorts of ≤50 (Yap and Davies, 2007; Biasin et al., 2015; Choi et al., 2022). Five reported cohorts of >50–100 (Oktay and Oktem, 2010; Hulsbosch et al., 2018; Delattre et al., 2020; Hoekman et al., 2020; Grellet-Grün et al., 2023). Six reported cohorts of >100–200 (Sánchez et al., 2008; Tanbo et al., 2015; Leflon et al., 2022; Silber et al., 2022; Barral et al., 2024; Takae et al., 2024). Three studies reported cohorts of >200–400 participants (Imbert et al., 2014; Rodriguez-Wallberg et al., 2019; Takae et al., 2022), and another three reported cohorts of >400–600 (Jadoul et al., 2017; Poirot et al., 2019; Finkelstein et al., 2025). One study reported a cohort of 800 participants (Diaz-Garcia et al., 2018). Additionally, three reported cohorts of >1000–1500 (Beckmann et al., 2018; Kristensen et al., 2021) and one reported a cohort of >2000 (Schallmoser et al., 2023). All OTC procedures were performed between 1999 and 2022. In all studies, OTC was performed for both malignant and benign indications; however, malignant disease made up the more frequent indication for OTC. Fabbri et al. reported that among 1026 patients who underwent OTC, 91% (n = 930) did so for malignant indications, whereas 9% (n = 96) did so for non-malignant indications (Fabbri et al., 2022), while Beckmann et al. reported that only 6.3% of the women had their tissue frozen for benign indications (Beckmann et al., 2018) (Table 1). The age at OTC ranged from 0 to 44 years. Three studies included only pediatric patients (aged ≤20 years at OTC) (Biasin et al., 2015; Poirot et al., 2019; Grellet-Grün et al., 2023), three studies included only adolescent and adult patients (≥16 years) (Diaz-Garcia et al., 2018; Leflon et al., 2022; Barral et al., 2024), 18 studies included both pediatric and adult patients at the time of OTC (Yap and Davies, 2007; Sánchez et al., 2008; Oktay and Oktem, 2010; Imbert et al., 2014; Tanbo et al., 2015; Jadoul et al., 2017; Hulsbosch et al., 2018; Rodriguez-Wallberg et al., 2019; Delattre et al., 2020; Hoekman et al., 2020; Kristensen et al., 2021; Choi et al., 2022; Silber et al., 2022; Takae et al., 2022, 2024; Schallmoser et al., 2023; Finkelstein et al., 2025), and 1 study did not specify the age of the patients at the time of OTC (Beckmann et al., 2018).
In most included studies, the follow-up time was not clearly defined but occurred within the overall time frame of the study (Table 1). For example, an Australian study by Finkelstein et al., which assessed return rates among women who underwent OTC between 1995 and 2022, reported that 48 of 593 women had returned for OTT (8.1%). However, the follow-up duration was not specified (Finkelstein et al., 2025). Except from one study that reported a minimum follow-up duration of ≥3 years after primary cancer treatment (Hulsbosch et al., 2018), none of the other studies reported a defined overall minimum follow-up duration (Table 1). Most studies did not account for patient mortality when calculating overall return rates; however, in one study, the overall return rate was calculated as the proportion of women who returned out of those who were alive (Rodriguez-Wallberg et al., 2019).
The return rate for use of cryopreserved ovarian tissue after completion of gonadotoxic treatment is depicted in the Forest plot (Fig. 2) and ranged from 0% to 14%. Of the 25 studies, 18 reported a return rate of ≤5%, 6 reported a return rate of >5% to ≤10% while only 1 study reported a return rate of 14%.
When stratified by age group at the time of OTC, studies including only pediatric patients reported return rates ranging from 0.7% to 2% (Biasin et al., 2015; Poirot et al., 2019; Grellet-Grün et al., 2023), compared to return rates of 6.2–9.5% (Diaz-Garcia et al., 2018; Leflon et al., 2022; Barral et al., 2024) in studies including only adolescents and adults (≥16 years).
Discussion
Overall, we found a low return rate of 0–14% after OTC, with most of the studies reporting return rates of ≤5%. In most studies, follow-up occurred within the time frame of the study, with only 8 studies explicitly reporting the follow-up duration, which ranged from 0 to 19.1 years (Oktay and Oktem, 2010; Biasin et al., 2015; Diaz-Garcia et al., 2018; Rodriguez-Wallberg et al., 2019; Hoekman et al., 2020; Leflon et al., 2022; Grellet-Grün et al., 2023; Schallmoser et al., 2023) (Table 1). The reasons for the modest return rates can be manyfold. Key factors influencing the return rate for AOTT include: 1) length of follow-up, 2) need for AOTT (development of POI after OTC), 3) desire to undergo AOTT, and 4) the actual feasibility of AOTT, including mortality among those who had undergone OTC.
Length of follow-up
Since AOTT may occur several years after OTC, limited follow-up time may bias the results. In all included studies, a subset of participants remained within reproductive age at EOF. Furthermore, most of the studies included both children and adults who underwent OTC and did not exclude individuals younger than 18 years of age at EOF when calculating return rates. Consequently, these analyses may underestimate true utilization rates by not accounting for participants who were not yet eligible for tissue transplantation (e.g. actively undergoing gonadotoxic therapy or in convalescence) or had not reached reproductive age or expressed a desire for pregnancy yet. Consistent with this, Emrich et al. (2025) examined storage patterns across age groups at the time of OTC and found that children and adolescents had a significantly higher proportion of active storage beyond 10 years compared with adults.
Need for AOTT (development of POI)
The risk of POI and infertility following cancer treatment depends, among others, on the type and cumulative dose of chemo and radiation therapy and therefore varies depending on the primary cancer diagnosis (Schüring et al., 2018; Van Den Berg et al., 2018). A substantial proportion of women who underwent OTC had been diagnosed with breast cancer. In the study by Schallmoser et al., women diagnosed with breast cancer accounted for 44.8% of patients who underwent OTC (1108 out of 2475), whereas in the study by Diaz-Garcia et al., it was 53.9% (431 out of 800) (Diaz-Garcia et al., 2018; Schallmoser et al., 2023). However, many clinics no longer offer OTC as the first choice of FP to women with breast cancer, partly because the likelihood of natural pregnancy after treatment in this patient group is high (Partridge et al., 2023; Magaton et al., 2025), and partly because oocyte or embryo cryopreservation provides additional benefits, such as the possibility of pre-implantation genetic testing (PGT) for individuals carrying BRCA 1/2 gene mutations (Macklon and De Vos, 2024).
In a sub-analysis of a Danish cohort, Kristensen et al. reported the use of cryopreserved ovarian tissue among patients who were alive and >24 years in 2020, stratified by diagnosis. They found a lower return rate among women diagnosed with breast cancer (18%) compared to that of women diagnosed with other malignant diseases (gastrointestinal malignancies (27%), gynecological malignancies (22%), sarcoma (21%)) (Kristensen et al., 2021).
Young age at cancer treatment has a mitigating effect on the risk of POI (Schüring et al., 2018; Anderson et al., 2022) and therefore, utilization rate for AOTT may be higher among women diagnosed at a more advanced age. Kristensen et al. (2021) assessed the impact of age at the time of OTC on subsequent return rates. They found that women who underwent OTC aged ≥30 years had a return rate of 15%, nearly twice that of those aged 18–29 years (8%) (Kristensen et al., 2021). In many facilities, OTC is recommended only for women aged <35 years (Anderson et al., 2020), due to unfavorable results in those >35 years, and the lower risk of infertility after gonadotoxic treatment in younger patients may therefore also contribute to the overall low return rate. This may also partially explain the low return rates reported in studies that include only pediatric patients.
Desire to undergo AOTT
Patients undergoing OTC for FP prior to gonadotoxic treatment may experience a change in their desire to have children following cancer treatment. For many cancer survivors, fear of disease recurrence is a significant concern and the possibility of bringing a child into the world who might lose a parent at an early age may also play an important role in their decision-making regarding attempts to conceive (Liu et al., 2025). A Belgian study by Hulsbosch et al. showed that among women in remission who had undergone OTC±GnRH agonist (n = 39), 46% (n = 18) expressed a desire for pregnancy, while 54% (n = 21) did not, after a minimum of 3-year follow-up (Hulsbosch et al., 2018). A Danish study by Macklon et al. found that among those who requested disposal of their cryopreserved ovarian tissue after an initial period of at least 5 years (17%), 19% did so because they decided not to have children (Macklon et al., 2014). Furthermore, following a prolonged treatment period, often including both surgical and medical interventions, patients may be reluctant to undergo additional surgical procedures required for transplantation of the cryopreserved tissue. Schallmoser et al. assessed the reason for ending storage among 224 patients who had undergone OTC for FP. They showed that 25.9% ended storage due to a lack of desire to have children, while 3.1% cited fear of future surgery as a reason. Additional reasons for discontinuing storage included pregnancy (natural or after IVF treatment), cancer recurrence, high storage costs, or patient death (Schallmoser et al., 2023).
Actual feasibility of AOTT, including mortality
The low return rate, when reported without accounting for mortality, may be further influenced by the fact that some of the diagnoses associated with a high risk of infertility also carry a high mortality risk. Macklon (2019) found a mortality rate of 13% in a Danish cohort of 927 girls and women who underwent OTC with the most deaths observed in the group with upper gastro-intestinal cancers and sarcomas. Furthermore, oocyte and embryo cryopreservation have partly replaced OTC as preferred FP method in recent times (Anderson et al., 2020). Consequently, OTC is increasingly offered only to women with limited time before starting chemotherapy, often due to advanced cancer progression. Therefore, women undergoing OTC for FP, particularly in more recent times, may have a worse prognosis, potentially reducing the number of women who survive long enough to utilize the cryopreserved tissue and thereby contributing to the lower observed return rates.
Heterogeneity between studies
The return rate for the use of cryopreserved ovarian tissue varied substantially across included studies, possibly explained by the heterogeneity between studies including age at OTC, follow-up time, indications for OTC, and country of FP. Stratified by age at OTC, the utilization rate among patients who had their tissue frozen as children (range 0.7–2%) was lower compared to the rate among those who had their tissue frozen as adolescents and adults (range 6.2–9.5%). As return for AOTT may occur several years after OTC, the lower return rate observed among children may be partly explained by the fact that they have not yet reached reproductive age or have not yet expressed desire for childbearing by the end of the follow-up period. Further studies with extended follow-up duration are needed.
Furthermore, in a Belgian study by Delattre et al., OTC was performed in addition to either controlled ovarian stimulation (COS), oocytes retrieved from ovarian tissue ex vivo (OTO-IVM), or transvaginal retrieval of oocytes for IVM. Consequently, the return rate for utilization of the cryopreserved ovarian tissue may be lower in these patients as they would likely choose to use their cryopreserved oocytes or embryos first in order to avoid another surgical procedure (Delattre et al., 2020). This may also apply to some of the other included studies, as it is unclear whether they exclusively had OTC performed or if other FP methods were used simultaneously.
Overall, studies have reported higher return rates for the use of cryopreserved oocytes, embryos, and semen compared to OTC. A review by Wnuk et al. (2023)found that return rates for the use of oocytes, embryos, and semen cryopreserved prior to gonadotoxic treatment ranged from 3.1% to 8.7%, 9% to 22.4%, and 2.6% to 21%, respectively.
Variations among countries concerning patient-borne cost of the treatment may result in differences between populations receiving OTC and the length of storage. In countries where patients must cover the costs themselves, OTC is more likely to be pursued by women with a clear intention to undergo AOTT, if needed. In contrast, in countries where the procedure is offered to patients free of charge, a greater proportion of women may choose to undergo it as a precautionary measure, even though they may never use it. This may partly explain the high return rate in the study by Silber et al. (2022).
Cultural and religious variations between countries regarding whether women are reluctant to undergo AOTT if they are unmarried may also contribute to variations in return rates between countries. Studies have shown that cancer survivors are less likely to marry, compared to the general population, and they may therefore, in some countries, have a reduced likelihood of becoming mothers (Syse, 2008; Kirchhoff et al., 2012).
Furthermore, eligibility criteria for OTC may vary between countries, influenced by disease severity and associated mortality risk. This is particularly important, as most studies do not account for mortality when reporting return rates.
Limitations
Although this systematic review is up to date and methodologically robust, with broad search criteria, it has several limitations. Many of the included studies either lack follow-up information or fail to specify a minimum follow-up duration. The studies are also heterogeneous in their populations, particularly regarding patient age. Moreover, standardized definitions of ‘return’ are absent. These limitations may contribute to underreporting and bias. Return rate was not the primary outcome of most of the included studies, and therefore, there is a risk of underreporting or inconsistent outcome ascertainment. This may influence the reliability of the prevalence estimates reported.
Conclusion
Despite the common practice of offering OTC as FP, the low utilization rates highlight the need for careful consideration to avoid subjecting women to potentially unnecessary and costly treatment. The procedure diminishes the ovarian reserve and, like all surgical interventions, carries risks of complications such as infection and bleeding, that could, if severe enough, delay subsequent cancer treatment. Reassuringly, however, studies have shown a high satisfaction rate and a low complication rate (Beckmann et al., 2018). On the other hand, the importance of the hope that OTC represents for the patients during a very difficult time should not be underestimated either (Bach et al., 2020; Bentsen et al., 2023). The overall modest return rates for the use of ovarian tissue cryopreserved prior to gonadotoxic treatment found in this study emphasize the importance of future studies with longer follow-up time to assess patterns of tissue utilization in relation to diagnosis, treatment protocol, and age thereby setting criteria in the selection of patients who would actually benefit from OTC.
Supplementary Material
hoaf068_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anderson RA , Amant F, Braat D, D’Angelo A, Chuva de Sousa Lopes SM, Demeestere I, Dwek S, Frith L, Lambertini M, Maslin C et al ESHRE guideline: female fertility preservation. Hum Reprod Open 2020;2020:hoaa 052.33225079 10.1093/hropen/hoaa 052PMC 7666361 · doi ↗ · pubmed ↗
- 2Anderson RA , Cameron D, Clatot F, Demeestere I, Lambertini M, Nelson SM, Peccatori F. Anti-Müllerian hormone as a marker of ovarian reserve and premature ovarian insufficiency in children and women with cancer: a systematic review. Hum Reprod Update 2022;28:417–434.35199161 10.1093/humupd/dmac 004PMC 9071067 · doi ↗ · pubmed ↗
- 3Anderson RA , Wallace WHB, Telfer EE. Ovarian tissue cryopreservation for fertility preservation: clinical and research perspectives. Hum Reprod Open 2017;2017:hox 001.30895221 10.1093/hropen/hox 001PMC 6276668 · doi ↗ · pubmed ↗
- 4Bach AS , Macklon KT, Kristensen SG. Futures and fears in the freezer: Danish women’s experiences with ovarian tissue cryopreservation and transplantation. Reprod Biomed Online 2020;41:555–565.32736871 10.1016/j.rbmo.2020.06.009 · doi ↗ · pubmed ↗
- 5Barral Y , Borrás A, Carrillo P, AgustíI, Peralta S, Casals G, Fàbregues F, GuimeràM, Corral JM, Calafell JM et al Current status of fertility preservation in a Spanish tertiary public hospital: multidisciplinary approach and experience in over 1500 patients. Clin Transl Oncol 2024;26:1129–1138.37872422 10.1007/s 12094-023-03330-2 · doi ↗ · pubmed ↗
- 6Beckmann MW , Dittrich R, Lotz L, van der Ven K, van der Ven HH, Liebenthron J, Korell M, Frambach T, Sütterlin M, Schwab R et al Fertility protection: complications of surgery and results of removal and transplantation of ovarian tissue. Reprod Biomed Online 2018;36:188–196.29198423 10.1016/j.rbmo.2017.10.109 · doi ↗ · pubmed ↗
- 7Bentsen L , Pappot H, Hjerming M, Hanghøj S. Thoughts about fertility among female adolescents and young adults with cancer: a qualitative study. Support Care Cancer 2023;31:421.37357225 10.1007/s 00520-023-07887-0PMC 10290964 · doi ↗ · pubmed ↗
- 8Biasin E , Salvagno F, Berger M, Nesi F, Quarello P, Vassallo E, Evangelista F, Marchino GL, Revelli A, Benedetto C et al Ovarian tissue cryopreservation in girls undergoing haematopoietic stem cell transplant: experience of a single centre. Bone Marrow Transplant 2015;50:1206–1211.25961773 10.1038/bmt.2015.111 · doi ↗ · pubmed ↗