Real-Time Personal Protective Equipment (PPE) Compliance and Clinical Tool Monitoring Using Generative AI: A Novel Approach for Adaptive and Automated Healthcare Surveillance
Manit Gupta, Rajaram Gairaboni, Andrei Lyle Bautista, Katherine Vo Brown, Bhavit Gupta, Austin Bautista, Alexander Bautista, Lady Christine Ong Sio, Shuchita Garg

TL;DR
A new generative AI system monitors PPE compliance in real-time, adapting to changing hospital rules without retraining, and shows high accuracy in tests.
Contribution
A generative AI system that translates natural language rules into real-time monitoring logic without retraining.
Findings
The system achieved 95.8% accuracy and 91.0% recall in mannequin-based trials.
Performance was consistent across different skin tones and prompt types with no false positives.
The system showed high adaptability and cost efficiency for real-time healthcare surveillance.
Abstract
Background: Hospital-acquired infections (HAIs) remain a critical patient safety concern, affecting one in 31 hospitalized patients daily. Non-compliance with personal protective equipment (PPE) protocols is a preventable driver. Current monitoring methods, such as manual audits and closed-circuit television (CCTV), are limited by delays, inconsistency, and reactivity. Traditional artificial intelligence (AI) systems are rigid and require retraining when protocols change. Objective: To construct and evaluate a generative AI-driven compliance monitoring system, built with Google Gemini (Mountain View, CA, USA) on Raspberry Pi (Cambridge, UK) hardware that translates hospital rulebooks or free-text prompts into real-time enforcement logic without retraining. Methods: The system integrated Gemini, OpenCV (Dover, DE, USA) and Streamlit (San Francisco, CA, USA) to convert natural language…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
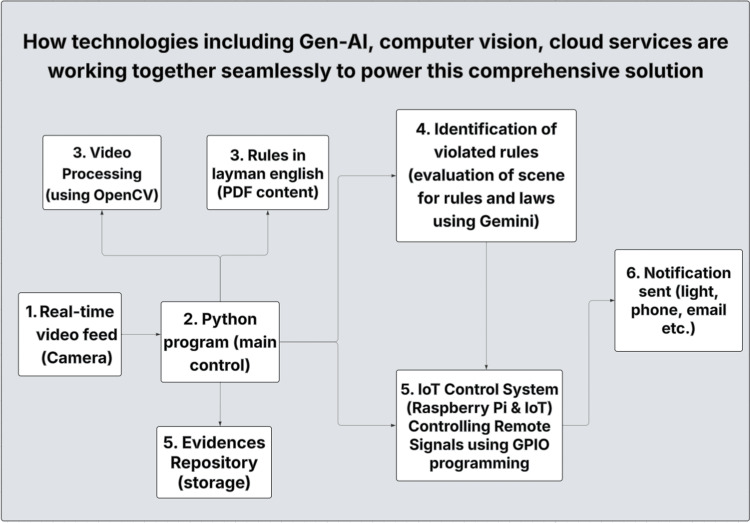 Figure 1
Figure 1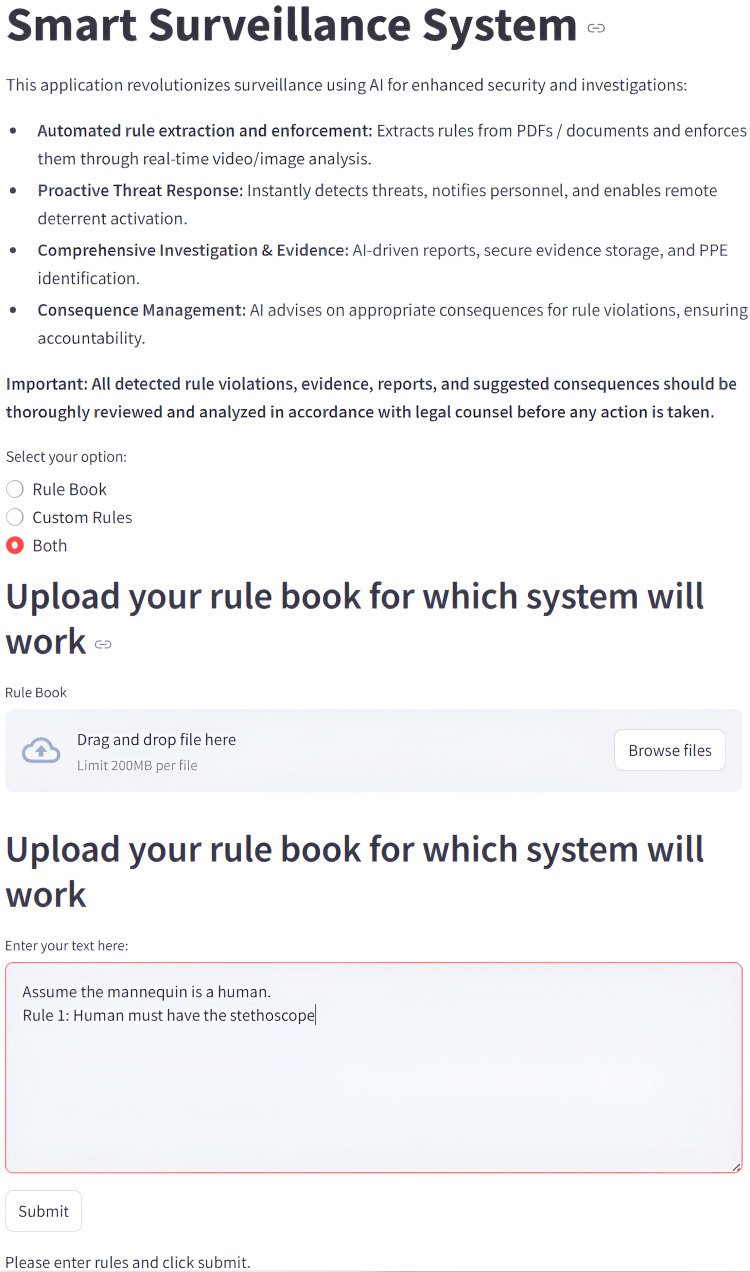 Figure 2
Figure 2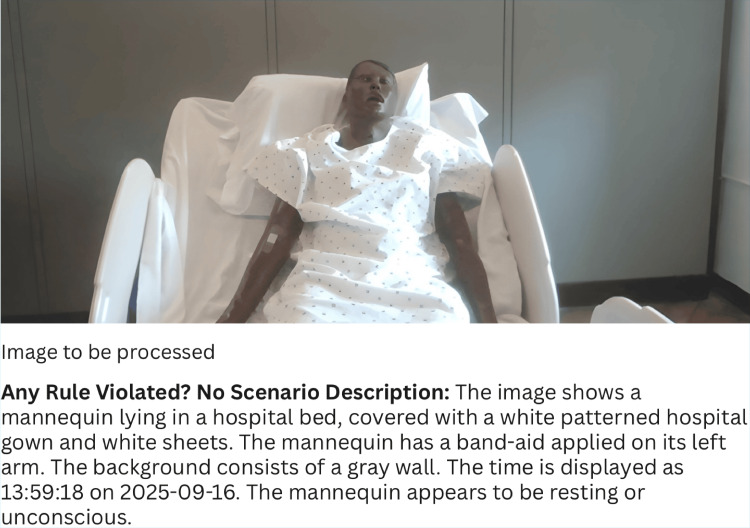 Figure 3
Figure 3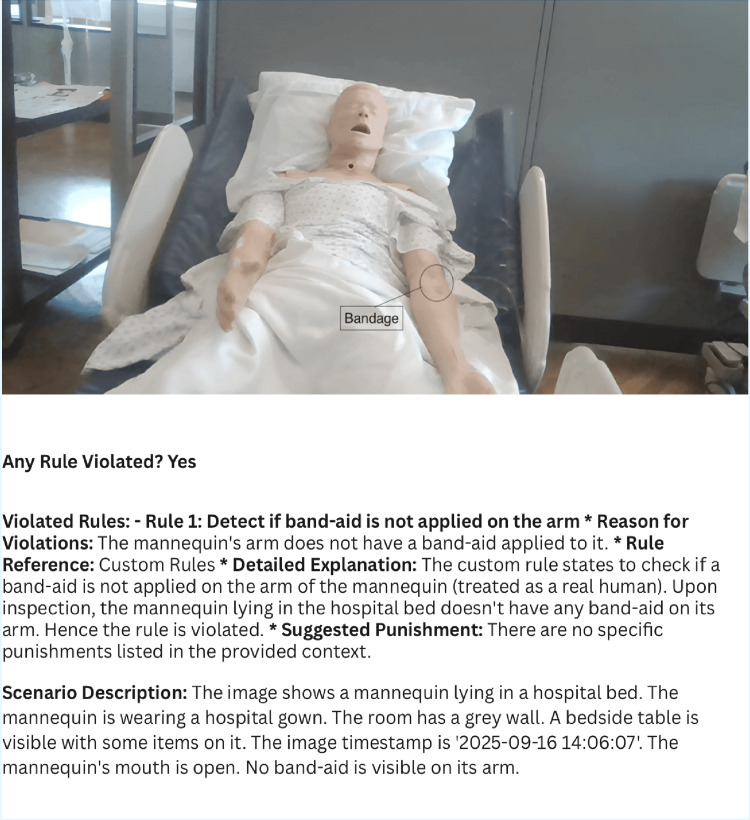 Figure 4
Figure 4| Measure | Value | Formula |
| Sensitivity | 0.9103 | True Positive Rate = True Positive / (True Positive + False Negative) |
| Specificity | 1 | Specificity = True Negative / (False Positive + True Negative) |
| Positive Predictive Value (Precision) | 1 | Positive Predictive Value = True Positive / (True Positive + False Positive) |
| Negative Predictive Value | 0.9278 | Negative Predictive Value = True Negative / (True Negative + False Negative) |
| False Positive Rate | 0 | False Positive Rate = False Positive / (False Positive + True Negative) |
| False Discovery Rate | 0 | False Discovery Rate = False Positive / (False Positive + True Positive) |
| False Negative Rate | 0.0897 | False Negative Rate = False Negative / (False Negative + True Positive) |
| Accuracy | 0.9583 | Accuracy = (True Positive + True Negative) / (True Positive + True Negative + False Positive + False Negative) |
| F1 Score | 0.953 | F1 = 2*True Positive / (2*True Positive + False Positive + False Negative) |
| Matthews Correlation Coefficient | 0.919 | Matthews Correlation Coefficient = (True Positive * True Negative – False Positive * False Negative) / (sqrt((True Positive + False Positive) * (True Positive + False Negative) * (True Negative + False Positive) * (True Negative + False Negative))) |
| Label | Total | True Positive | False Negative | True Negative | False Positive | Accuracy | Sensitivity (Recall) | Specificity | Precision | F1 Score | Balanced Accuracy |
| Object: Blood Pressure Cuff | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Blood Pressure Cuff | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Bandaid | 12 | 3 | 3 | 6 | 0 | 0.75 | 0.5 | 1 | 1 | 0.6666666667 | 0.75 |
| Object: Bandaid + Syringe | 12 | 2 | 4 | 6 | 0 | 0.6666666667 | 0.3333333333 | 1 | 1 | 0.5 | 0.6666666667 |
| Object: Gloves | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Gown | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Gown + Socks | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Gown+socks | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Mask | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: On floor | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Oximeter | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Oximeter | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Oximeter + Gown + Blood Pressure Cuff | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Rulebook | 12 | 0 | 0 | 12 | 0 | 1 | 1 | 1 | |||
| Object: Rulebook + rule glove | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Rulebook + rule mask | 12 | 6 | 0 | 6 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Stehoscope | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Object: Stethoscope | 6 | 3 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Label | Total | True Positive | False Negative | True Negative | False Positive | Accuracy | Sensitivity (Recall) | Specificity | Precision (PPV) | F1 Score | Balanced Accuracy |
| Skin: Black | 84 | 37 | 2 | 45 | 0 | 0.9761904762 | 0.9487179487 | 1 | 1 | 0.9736842105 | 0.9743589744 |
| Skin: White | 84 | 34 | 5 | 45 | 0 | 0.9404761905 | 0.8717948718 | 1 | 1 | 0.9315068493 | 0.9358974359 |
| Label | Total | True Positive | False Negative | True Negative | False Positive | Accuracy | Sensitivity (Recall) | Specificity | Precision (PPV) | F1 Score | Balanced Accuracy |
| Position: Front | 84 | 48 | 4 | 32 | 0 | 0.9523809524 | 0.9230769231 | 1 | 1 | 0.96 | 0.9615384615 |
| Position: Left | 84 | 23 | 3 | 58 | 0 | 0.9642857143 | 0.8846153846 | 1 | 1 | 0.9387755102 | 0.9423076923 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsQuality and Safety in Healthcare · Occupational Health and Safety Research · Healthcare Technology and Patient Monitoring
Introduction
Healthcare-associated infections (HAIs) significantly increase patient morbidity, mortality, and healthcare costs [1,2]. Adherence to hand hygiene (HH) and personal protective equipment (PPE) is central to infection prevention [2-4]. However, compliance remains inconsistent, with lapses driving nosocomial infection [3,5,6].
Traditional compliance monitoring has critical limitations. Direct observation, while considered a gold standard, is resource-intensive, prone to bias, and subject to the Hawthorne effect [7-10]. Closed-circuit television (CCTV) provides objective data but is primarily retrospective and raises privacy concerns [10]. Traditional artificial intelligence (AI) surveillance relies on rigid, predefined algorithms that require retraining when guidelines change [1,11]. Collectively, these issues underscore the need for flexible, adaptive, and scalable monitoring systems.
AI has shown promise across infection prevention and safety applications. AI has improved HH compliance [9], enhanced fall detection [11-13], and supported environmental safety with disinfection robots [14]. These applications illustrate AI’s ability to deliver proactive and reliable monitoring.
Unlike prior AI-based PPE monitoring approaches, this system uses generative AI to translate unstructured compliance rules into executable monitoring logic without retraining, enabling rapid adaptation to changing protocols. Generative AI models are designed to learn patterns from large datasets and create new outputs such as text, images, or structured logic based on learned representations, allowing flexible adaptation across contexts.
We hypothesize that a generative AI-driven compliance monitoring system can detect PPE adherence with ≥90% accuracy across varying conditions, offering a measurable improvement over conventional manual audits or static AI approaches. This study evaluates whether a generative AI system can reliably detect PPE compliance in simulated clinical scenarios, quantifying sensitivity, specificity, and inter-rater agreement.
Materials and methods
System design
The system is a generative AI-driven surveillance platform built on a standard camera and Raspberry Pi 3B+ (Cambridge, UK). A real-time video feed is processed by both a main Python (Fredericksburg, VA, USA) program and OpenCV (Dover, DE, USA) for object detection. User-defined compliance rules, entered through a Streamlit (San Francisco, CA, USA) interface are sent to Google Gemini (gemini-2.0-flash-001; Mountain View, CA, USA) which interprets the natural language rules and analyzes the scene. When violations are detected, Raspberry Pi functions as an Internet of Things (IoT) controller, triggering real-time notifications via legacy devices (lights, alarms) connected using general-purpose input/output (GPIO) programming, and storing evidence (annotated images and video) for later investigation. This architecture enables low-cost deployment without new infrastructure (Figure 1).
End-to-end surveillance workflow: real-time video is processed with OpenCV, analyzed by Gemini AI against user-defined rules, and triggers alerts with evidence storage.PDF: portable document format, IoT: Internet of Things, GPIO: general-purpose input/output
Development and testing procedures
A Streamlit interface enabled rule entry via free text or uploaded documents (Figure 2). Gemini translated these inputs into executable logic for OpenCV object recognition, with evidence of violations (annotated frames and text) automatically stored. Notifications were delivered through a Raspberry Pi, which activated legacy devices (lights, alarms) as intelligent outputs. Testing was conducted at three levels: functional (rule creation and detection), integration (component interaction), and notification (delivery speed). Independent variables included mannequin conditions, object type, and prompt type; dependent variables were detection accuracy and notification success. Each object was tested with two variations of the same prompt to ensure consistency across natural language variations.
This image shows the web interface for the Smart Surveillance System, which allows users to define custom monitoring rules. The user can select to upload a portable document format (PDF) rulebook, enter custom rules directly, or both. The screenshot shows the "Both" option selected, with a sample rule entered that instructs the system to assume a mannequin is a human and requires it to be holding a stethoscope along with an option given to upload a rulebook.
Experimental setup and evaluation
Trials (n=168) used mannequins of two skin tones (Black/White) and orientations (Front/Left). Objects included PPE and medical tools (e.g., gloves, gowns, stethoscopes), with both single- and multi-object scenarios (Figure 3). Two input modes were assessed: free-text prompts and Occupational Safety and Health Administration (OSHA) rulebook-derived prompts from uploaded documents. For each object-condition pair, six trials were run (three with the object present, three absent), with ground truth defined as a binary Yes/No label. Performance was evaluated using accuracy, sensitivity, specificity, F1 score, and Cohen’s Kappa, with 95% confidence intervals calculated via Wilson and bootstrap methods.
System output showing a mannequin in a hospital bed with AI analysis below, including rule evaluation, scene description, object identification, and required items. The rule given for this trial was “Assume the Mannequin is a real human. Detect if band-aid is not applied on the arm”, and the system correctly identifies it.
This dynamic approach allows hospitals or administrators to upload rulebooks and custom rules in various formats, which are automatically transformed into monitoring logic without requiring model retraining. This provides a highly adaptable system that can quickly accommodate new compliance criteria. The system was designed around four key criteria: real-time detection with a target accuracy of over 90%, immediate notifications, seamless integration with existing CCTV infrastructure, and a user-friendly interface. A hybrid software stack was implemented, combining Google Gemini for semantic interpretation, OpenCV for image and video stream processing, Streamlit for the user interface, and Python-based Application Programming Interface (API) for hardware and cloud integration.
Results
Overall performance
The system demonstrated robust detection capabilities across all 168 mannequin-based trials. Overall accuracy reached 95.8% (95% CI: 91.7-98.0%), with sensitivity of 91.0% (95% CI: 82.6-95.6%) and perfect specificity of 100% (95% CI: 95.9-100%), indicating that the model reliably detected true violations while avoiding false positives. Precision was 100% (95% CI: 94.9-100%), and the F1 score, reflecting the balance between precision and recall, was 0.953 (bootstrap 95% CI: 0.911-0.986). Agreement with the reference standard was excellent, with a Cohen’s Kappa of 0.916 (Table 1). These results indicate a conservative yet highly reliable detection profile, prioritizing accuracy and precision while maintaining high recall, which is critical for minimizing unnecessary alerts and alarm fatigue in healthcare settings.
Subgroup analyses
Single-object trials consistently exhibited higher sensitivity and F1 scores than multi-object combinations, though overall performance remained strong (Table 2). The AI system achieved perfect accuracy, sensitivity, specificity, and F1 scores (1.0) for most PPE and patient-safety rules-including stethoscopes, gloves, gowns, masks, blood pressure cuffs, oximeters, and bed placement were also included to evaluate the system’s versatility in detecting both PPE adherence and proper handling of clinical equipment, with no false positives observed, indicating alerts were mostly correct. Performance was lower for nuanced tasks such as band-aid placement or combined syringe and band-aid detection, with accuracy 0.5-0.83 and sensitivity 0-0.67, though specificity and precision remained high across all prompts. In rulebook trials, the numerous rules caused the system to flag violations for all missing items, making it impossible to satisfy every rule simultaneously (Table 2). Rulebook-only trials tested the mannequin without PPE, while rulebook + item trials assessed one item at a time. Consequently, F1, precision, and sensitivity are not reported for rulebook-only trials, as no scenario satisfied all rules.
System performance across skin tones was robust: Black and White mannequins showed overlapping confidence intervals for sensitivity, specificity, and F1 scores, indicating negligible bias and equitable detection (Table 3).
Similarly, performance across camera positions was consistently high, with accuracy >95% and perfect specificity. Slightly lower sensitivity in side-angle trials suggests minor variation, but confidence intervals overlapped, confirming robustness across viewing perspectives (Table 4).
Overall, false negatives were limited, and no false positives were observed, reflecting a conservative detection strategy. Multi-object scenarios and certain positional angles were the most challenging, yet overall performance remained strong. Rulebook integration proved advantageous for consistent compliance enforcement, supporting the system’s practical utility in real-world hospital settings.
Discussion
This study demonstrates that a generative AI-based compliance monitoring system can reliably detect PPE adherence and other healthcare safety behaviors, such as the correct handling and placement of clinical tools including stethoscopes, blood pressure cuffs, and oximeters, in real time, achieving high accuracy and excellent agreement with reference standards (Cohen’s Kappa = 0.92). Detection performance was consistent across mannequin skin tones, camera orientations, and prompt types, highlighting fairness and potential generalizability. Importantly, no false positives were observed, minimizing unnecessary alerts that could contribute to alarm fatigue, while sensitivity remained high at 91%, indicating effective detection of true violations.
Compared with manual audits, CCTV monitoring, and conventional AI systems, the system offers significant advantages: proactive monitoring, dynamic interpretation of evolving compliance rules without retraining, and integration with existing infrastructure via low-cost Raspberry Pi hardware [1-3,10]. Clinically, this enables real-time enforcement of infection prevention measures such as PPE adherence, hand hygiene, operating room sterile protocols, and safe handling of medical equipment, while reducing hospital-acquired infections, labor-intensive observation, associated costs, and the workload for infection prevention and control nurses.
Limitations include mannequin-based testing under controlled conditions, sensitivity below 100%, and challenges in multi-object detection, camera distance, or objects blending with backgrounds (Figure 4). Additionally, real-time monitoring systems raise important ethical concerns related to privacy and potential HIPAA violations. Future work should expand datasets, conduct live hospital trials with cost-benefit analyses, integrate with electronic health records and alert systems, and optimize detection under more complex environmental conditions.
The image shows a mannequin in a hospital bed, with a bandage, serving as the input for the project. The analysis correctly notes the mannequin's appearance but provides an incorrect result, flagging a rule violation for a "missing" band-aid, even though one is present.
Overall, this generative AI system combines adaptability, fairness, and cost-efficiency, offering a robust solution for real-time compliance monitoring. Its consistent performance across object combinations, skin tones, and camera angles demonstrates strong generalizability, highlighting its potential for dynamic hospital environments. By enabling proactive detection of PPE and safety protocol adherence, the system can enhance patient and staff safety, reduce reliance on manual audits, and support scalable, automated infection prevention.
Conclusions
This generative AI-driven surveillance system demonstrated high accuracy, reliability, and fairness in monitoring PPE and healthcare compliance behaviors across different mannequin skin tones, orientations, and prompt types. Compared with manual audits, CCTV monitoring, and conventional AI models, it offers a proactive, flexible, and cost-effective approach that can dynamically incorporate evolving protocols without retraining. While testing was limited to mannequin trials under controlled conditions, and sensitivity below 100% indicates a small risk of missed detections, the results support further hospital-based trials and integration with clinical systems. With additional validation, this system has the potential to enhance real-time compliance monitoring, reduce infection risk, and improve patient and staff safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Enhancing infection control in IC Us through AI: a literature review Health Sci Rep Godbole AA Paras Paras Mehra M Banerjee S Roy P Deb N Jagtap S 08202510.1002/hsr 2.70288 PMC 1170550739777278 · doi ↗ · pubmed ↗
- 2Importance of hospital infection control Cureus Kubde D Badge AK Ugemuge S Shahu S 015202310.7759/cureus.50931 PMC 1080128638259418 · doi ↗ · pubmed ↗
- 3Factors influencing compliance with personal protective equipment (PPE) use among healthcare workers Cureus George J Shafqat N Verma R Patidar AB 015202310.7759/cureus.35269 PMC 1003575936968930 · doi ↗ · pubmed ↗
- 4OSHA: Personal Protective Equipment Washington, D.C.U.S. Department of Labor 2023 https://www.osha.gov/sites/default/files/publications/osha 3151.pdf
- 5Successfully addressing non-compliance with behavioral and social infection control measures is a critical component in management of healthcare worker COVID-19 outbreaks: learning outcomes from the first staff outbreak in the main maternity hospital in Qatar Front Public Health Petkar HM George B Mostafa E 15344211320254095963610.3389/fpubh.2025.1534421 PMC 12434125 · doi ↗ · pubmed ↗
- 6Infection prevention and control compliance among exposed healthcare workers in COVID-19 treatment centers in Ghana: a descriptive cross-sectional study P Lo S One Ashinyo ME Dubik SD Duti V 016202110.1371/journal.pone.0248282 PMC 794301033690699 · doi ↗ · pubmed ↗
- 7Hand-hygiene compliance by hospital staff and incidence of health-care-associated infections, Finland Bull World Health Organ OjanperäH Kanste OI Syrjala H 4754839820203274203310.2471/BLT.19.247494 PMC 7375219 · doi ↗ · pubmed ↗
- 8Impact of an automated hand hygiene monitoring system combined with a performance improvement intervention on hospital-acquired infections Infect Control Hosp Epidemiol Knepper BC Miller AM Young HL 9319374120203246092810.1017/ice.2020.182 · doi ↗ · pubmed ↗