Gemcitabine-Induced Thrombotic Microangiopathy in a Patient With Metastatic Pancreatic Cancer: A Case Report
Jacqueline Young

TL;DR
A 65-year-old woman with pancreatic cancer developed a rare blood disorder after gemcitabine treatment, which was managed with complement-inhibiting drugs.
Contribution
This case report documents the successful use of complement inhibitors for treating gemcitabine-induced thrombotic microangiopathy.
Findings
The patient developed acute kidney injury, hemolytic anemia, and thrombocytopenia consistent with GiTMA.
Treatment with eculizumab and later ravulizumab improved the patient's condition by inhibiting the complement cascade.
The case emphasizes the importance of early recognition and targeted therapy for GiTMA.
Abstract
Thrombotic microangiopathies (TMA) are potentially life-threatening conditions caused by small-vessel platelet thrombi. Gemcitabine has been reported to induce TMA. Early detection and treatment of gemcitabine-induced TMA (GiTMA) are important to improve overall mortality. This case details a 65-year-old female with metastatic pancreatic acinar cell carcinoma who was treated with gemcitabine. The patient presented with acute kidney injury, hemolytic anemia (requiring transfusion), and thrombocytopenia. She underwent a renal biopsy, which was consistent with thrombotic microangiopathy in the subacute to chronic phase. The patient was initially treated with eculizumab, followed by a transition to ravulizumab due to the latter's less frequent dosing. Eculizumab and ravulizumab are both monoclonal antibodies targeting complement protein C5, subsequently inhibiting the terminal complement…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
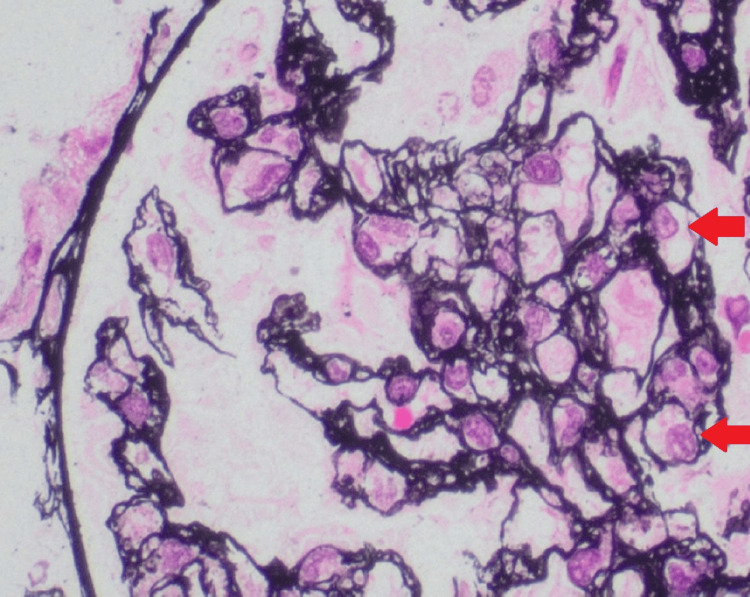 Figure 1
Figure 1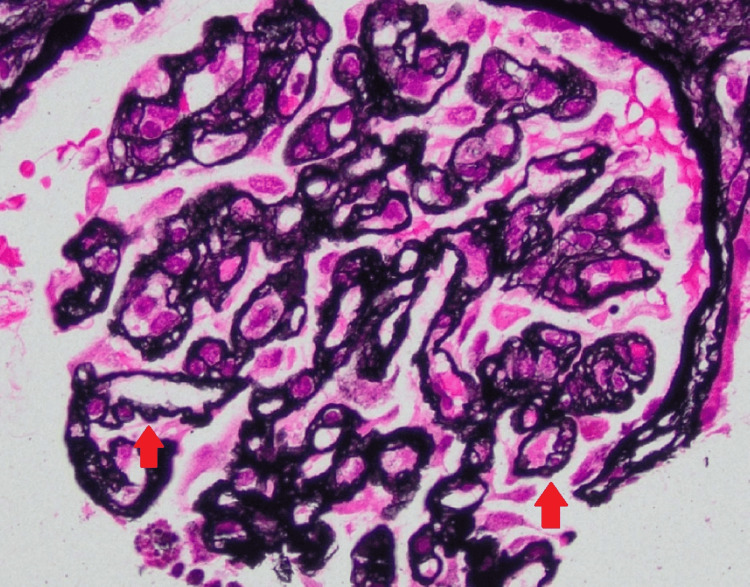 Figure 2
Figure 2| Blood Test | Result | Range |
| Sodium | 134 mmol/L | 136-145 mmol/L |
| Potassium | 5.0 mmol/L | 3.5-5.1 mmol/L |
| Chloride | 104 mmol/L | 98-107 mmol/L |
| HCO3 | 20 mmol/L | 22-29 mmol/L |
| BUN | 46 mg/dL | 6-20 mg/dL |
| Creatinine | 2.50 mg/dL | 0.7-1.2 mg/dL |
| White Blood Cell Count | 11.36 k/uL | 4.00-10.90 k/uL |
| Hemoglobin | 6.9 g/dL | 13.5-17.5 g/dL |
| Platelet Count | 95,000/μL | 150,000-450,000 /μL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Erythropoietin and Anemia Treatment · Renal Transplantation Outcomes and Treatments
Introduction
Thrombotic microangiopathy (TMA) is characterized by a triad of thrombocytopenia, microangiopathic hemolytic anemia, and organ dysfunction, most notably acute kidney injury. TMA is a broader term encompassing conditions like hemolytic uremic syndrome (HUS) and thrombotic thrombocytopenic purpura (TTP). HUS is often linked to kidney injury, while TTP is characterized by neurological involvement. Primary TMA is considered when the cause is unknown (idiopathic) and there are intrinsic abnormalities such as ADAMTS13 deficiency, complement dysregulation, or Shiga toxin-mediated injury [1]. Secondary TMA arises due to several conditions, such as infection, autoimmune disorders, pregnancy, malignancy, or medications. Drug-induced TMA (DITMA) should be suspected when TMA develops acutely after starting a new drug [2].
DITMA is challenging to diagnose, given that laboratory tests to identify a drug etiology may not be available. DITMA occurs through either immune-mediated mechanisms or direct toxicity of the drug. Gemcitabine is a nucleoside analog that is used to treat a variety of cancers, including lymphoma, lung, bladder, breast, and pancreatic cancer. Gemcitabine has been associated with TMA in 0.02-2% of treated patients [3]. Early recognition is crucial, as mortality rates can range from 50 to 90% [3,4]. This case discusses the presentation, diagnosis, and management of gemcitabine-induced thrombotic microangiopathy (GiTMA), emphasizing the critical importance of early recognition and interdisciplinary management. It also highlights the increasing role of complement inhibition therapy in improving outcomes for this rare and life-threatening complication.
Case presentation
A 65-year-old female with a past medical history of hypothyroidism, hyperlipidemia, and metastatic pancreatic acinar cell carcinoma with hepatic and retroperitoneal lymph node involvement presented as a referral from her primary care physician for worsening hypertension and kidney function. At her primary care office, she was noted to have a blood pressure of 190/90 mmHg and was placed on clonidine. Her creatinine was notable at 2.34 mg/dL (her baseline was around 0.8 mg/dL), and given that she also had significant lower extremity edema and fluid overload, the patient was admitted to our facility.
Regarding her oncological history, she presented three years earlier at an outside hospital for persistent abdominal pain radiating to the back. A CT abdomen and pelvis revealed a 9 cm mass in the perigastric region. Fine needle aspiration of the perigastric mass revealed a malignant epithelial neoplasm. The patient had a subsequent liver biopsy, which confirmed pancreatic acinar cell carcinoma. One month after diagnosis, the patient was started on fluorouracil, oxaliplatin, folinic acid, and irinotecan (FOLFIRINOX). Four months later, oxaliplatin was discontinued due to infusion reactions and neuropathy. One year after diagnosis, repeat imaging showed progression of disease, and the patient was started on gemcitabine and nab-paclitaxel. After nine cycles of gemcitabine and nab-paclitaxel, the patient was referred to radiation oncology for consolidative radiation therapy, given her low metastatic burden and biologically responsive disease. She received a total of five fractions of radiation therapy to the pancreatic mass. After completing radiation therapy, the patient was continued on gemcitabine and nab-paclitaxel. Repeat imaging continued to show stable pancreatic mass and stable retroperitoneal adenopathy with no new disease. The patient remained on gemcitabine and nab-paclitaxel until day one of the current hospital course.
Upon admission, the patient presented with bilateral lower extremity edema, resting dyspnea, paroxysmal nocturnal dyspnea, and oliguria. She denied any fever or neurological symptoms. Her initial vitals showed a blood pressure of 158/88 mmHg, a pulse of 93 bpm, a temperature of 98.6°F, a respiratory rate of 20/min, and oxygen saturation of 93% on room air. The initial blood test results are outlined in Table 1.
As seen in Table 1, the patient’s creatinine was 2.5 mg/dL on admission, with her normal baseline creatinine around 0.8 mg/dL. Her initial urinalysis was significant for proteinuria (170 mg/dL) and microscopic hematuria. Her urine protein-to-creatinine ratio was 4038.0 mg/g. A renal ultrasound was obtained, which showed no developing hydronephrosis and stable mild fullness of the left intrarenal collecting system. She was evaluated by nephrology, and a workup was initiated for nephrotic syndrome and concern for gemcitabine-induced thrombotic microangiopathy (GiTMA).
Given the low hemoglobin, the patient was transfused one unit of packed red blood cells. A hemolysis panel was obtained, which found an elevated lactate dehydrogenase at 525 U/L, a decreased haptoglobin at <8 mg/dL, and an elevated reticulocyte count of 7.65%. An ADAMTS13 level was obtained and resulting in 40% (with normal being greater than or equal to 61%). This further supported a diagnosis of TMA rather than thrombotic thrombocytopenic purpura (TTP), given that ADAMTS13 activity in TTP is usually less than 10%.
An extensive diagnostic workup was performed during hospitalization to evaluate infectious and autoimmune causes. Testing for Mycoplasma, Bordetella, parainfluenza, Chlamydia pneumoniae, RSV, and COVID-19 was negative. Blood cultures remained sterile. Serologic studies for hepatitis B and C, antinuclear antibodies (ANA), antineutrophil cytoplasmic antibodies (ANCA), cryoglobulins, and lupus anticoagulant were all negative. Her complement C3 and 4 levels were within normal limits. Shiga toxin testing was also negative, effectively ruling out Escherichia coli-associated hemolytic uremic syndrome (eHUS).
Due to the risk of progressive kidney injury, the patient was treated empirically with eculizumab alongside corticosteroids. Vaccinations against pneumococcus and meningococcus were administered prior to therapy, and penicillin V prophylaxis was initiated. Despite therapy, her kidney function declined, and she had worsening uremia, with a creatinine peaking at 4.0 mg/dL and a BUN of 106 mg/dL. This necessitated tunneled catheter placement and hemodialysis initiation. A renal biopsy was obtained and confirmed thrombotic microangiopathy in the subacute to chronic phase, with features such as endothelial cell swelling and glomerular basement membrane duplication, as seen in Figures 1, 2.
Silver stain demonstrates a glomerulus with prominent endothelial cell swelling (red arrow), which is commonly seen in conditions such as TMA and HUS. This indicates acute endothelial injury and dysfunction.TMA: Thrombotic microangiopathies, HUS: hemolytic uremic syndrome
Silver stain reveals glomerular basement membrane wrinkling and duplication (red arrow). This indicates chronic or ongoing injury to the glomerular wall.
Reassuringly, the patient remained transfusion independent after starting eculizumab. She was eventually discharged while remaining hemodialysis dependent. The patient was also discharged with prednisone 60 mg daily in addition to continuing the eculizumab 900 mg IV weekly.
The patient followed up with her oncologist and nephrologist. Her oncologist transitioned her chemotherapy regimen from gemcitabine and nab-paclitaxel to 5-fluorouracil and irinotecan liposome injection, as gemcitabine was no longer a viable option in her treatment plan. After four doses of eculizumab, she had some improvement in urine output but remained dialysis-dependent. Due to the advantage of less frequent dosing, her nephrologist replaced eculizumab with ravulizumab. After switching to ravulizumab, the patient had further improvement in urine output but continued to require hemodialysis. The patient’s hemoglobin and platelet counts continued to improve.
Discussion
Gemcitabine-induced TMA is associated with a constellation of symptoms. In a retrospective French cohort study, 97.4% of patients had AKI, 95.6% had hemolytic anemia, 74.6% had thrombocytopenia, 62.2% had hypertension, 56.7% had edema, 34.2% had proteinuria, and 22.8% had hematuria [5]. Our patient had all of the above symptoms. In addition, although the ADAMTS13 activity was decreased, the absence of fever and neurological symptoms made TTP less likely. Confirmation of the diagnosis was obtained via a renal biopsy, which was consistent with thrombotic microangiopathy in the subacute to chronic phase.
Gemcitabine is a nucleoside analog that incorporates into newly synthesized DNA, disrupting DNA replication and ultimately leading to cell death. Although the exact pathophysiology of GiTMA remains unclear, it is thought to involve endothelial cell injury, particularly within the renal vasculature [4]. Management of GiTMA begins with the prompt discontinuation of gemcitabine. Concurrent supportive care (including corticosteroids, blood transfusions, and hemodialysis) is essential to address complications. Eculizumab and ravulizumab are both monoclonal antibodies targeting the complement protein C5. They both inhibit the terminal complement cascade, reducing inflammation and tissue injury. While there is no definitive therapy for GiTMA, multiple case reports have documented successful outcomes with eculizumab, which is already approved for complement-mediated TMA [3].
Eculizumab has been the standard of care for treating atypical hemolytic uremic syndrome (aHUS) since it was approved in the United States in 2011. It requires maintenance dosing every two weeks for patients weighing 10 kg or more. Ravulizumab was approved in 2019 for the same indication. It has a longer half-life and requires less frequent dosing every 4 to 8 weeks, depending on body weight. Clinical studies have demonstrated that ravulizumab has comparable efficacy to eculizumab. In comparative studies, ravulizumab was associated with improved quality of life for both patients and caregivers and increased adherence and compliance to treatment, and was identified as the preferred treatment overall [6,7].
Conclusions
A high index of suspicion for GiTMA is essential, particularly as the use of gemcitabine continues to increase in oncology. Given the associated high mortality, early recognition and prompt discontinuation of gemcitabine are critical. Supportive care should be initiated immediately, and treatment with a complement inhibitor such as eculizumab should be strongly considered. Ravulizumab can also be considered, given it has shown similar efficacy and improved quality of life due to the need for less frequent dosing.
In our case, the patient was empirically treated with eculizumab early in the hospital course due to the high clinical suspicion for GiTMA and the potential consequences of delayed intervention. A subsequent renal biopsy confirmed the diagnosis. This case underscores the importance of early recognition and intervention, as the patient became transfusion-independent, progressed from anuria to oliguria, and demonstrated improvement in both platelet count and hemoglobin levels. However, it is important to note that the patient remained dialysis-dependent, which limits the assessment of the treatment efficacy. This outcome may be attributed to subacute to chronic changes already seen on the renal pathology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gemcitabine-induced thrombotic microangiopathy in a patient with cholangiocarcinoma: an atypical case Cureus Anil V Alhujaily E Grover D 016202410.7759/cureus.63385 PMC 1128384339070506 · doi ↗ · pubmed ↗
- 2Gemcitabine-induced thrombotic microangiopathy Intern Med J Richmond J Gilbar P Abro E 124012424320132423764610.1111/imj.12261 · doi ↗ · pubmed ↗
- 3Gemcitabine-induced thrombotic microangiopathy treated with eculizumab: a case report J Gastrointest Oncol Van den Eeckhaut L Hannon H Schurgers M 331433201320223663605410.21037/jgo-22-509PMC 9830318 · doi ↗ · pubmed ↗
- 4A case of gemcitabine-induced thrombotic microangiopathy treated with ravulizumab in a patient with Stage IV pancreatic cancer Cureus Mac Dougall KN Schwartz B Harewood J 013202110.7759/cureus.13031 PMC 793177533680585 · doi ↗ · pubmed ↗
- 5Thrombotic microangiopathy associated with gemcitabine use: Presentation and outcome in a national French retrospective cohort Br J Clin Pharmacol Daviet F Rouby F Poullin P 4034128520193039458110.1111/bcp.13808 PMC 6339967 · doi ↗ · pubmed ↗
- 6Treatment preference and quality of life impact: ravulizumab vs eculizumab for atypical hemolytic uremic syndrome J Comp Eff Res Mauch TJ Chladek MR Cataland S 012202310.57264/cer-2023-0036 PMC 1069041137515502 · doi ↗ · pubmed ↗
- 7Clinical efficacy and safety of switching from eculizumab to ravulizumab in adult patients with a HUS- real-world data BMC Nephrol Schönfelder K Kühne L Schulte-Kemna L 2022520243889842710.1186/s 12882-024-03638-3PMC 11188157 · doi ↗ · pubmed ↗