A qualitative Interview Study Investigating Patient, Health Professional, and Developer Perspectives on Real-World Implementation of Patient-Centered AI Systems
Natalie Benda, Pooja Desai, Zayan Reza, Victoria Winogora, Uday Suresh, Yiye Zhang, Alison Hermann, Rochelle Joly, Jyotishman Pathak, Meghan Reading Turchioe

TL;DR
This study explores how patients, healthcare workers, and AI developers view the real-world use of patient-centered AI systems, focusing on postpartum depression risk prediction.
Contribution
The study provides a multi-stakeholder perspective on implementing patient-centered AI systems, emphasizing ethical and practical considerations.
Findings
Participants emphasized the importance of mitigating AI harms like bias and stigma.
Transparency in AI accuracy and predictors is needed for safe decision-making.
Health professionals need training to interpret AI outputs, and governance systems are essential for responsible AI use.
Abstract
Our objective was to triangulate patient, health professional, and developer perspectives for implementing patient-centered artificial intelligence (AI) systems. We conducted semi-structured interviews with patients (N = 18), health professionals (N = 8), and AI developers (N = 8). We created interview guides informed by frameworks in bioethics and health information informatics. We utilized a predictive algorithm for determining risk for postpartum depression as a use case to concretize our discussions. Our team analyzed transcripts from interview recordings using thematic, directed content analysis and the constant comparative process. Participants found mitigating potential harms caused by AI (e.g., bias, stigma, or patient anxiety) greatly important. They also believed that AI must provide clinical benefits by allowing health professionals and patients to easily take actions based…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
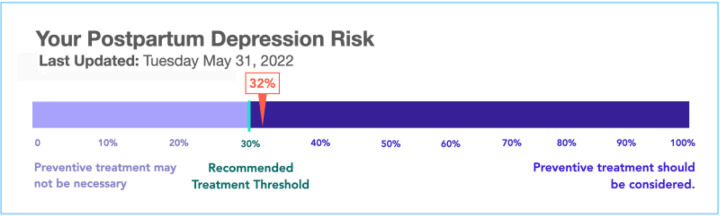 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Digital Mental Health Interventions · Electronic Health Records Systems
INTRODUCTION
The transition to artificial intelligence (AI) in healthcare continues to be significant for patients and health professionals.^1–4^ Despite AI’s predictive and generative power, many systems are never implemented or, when implemented, struggle to show improvements in patient outcomes compared to the standard of care.^5^ This clinical translation gap between AI development and real-world, successful deployment is defined as the “last mile” problem. The “last mile” problem is the fact that AI models may show high accuracy and promise in simulated lab-based tasks, but (1) they are either never deployed in clinical environments, or (2) they cannot improve outcomes in real-life due to deficiencies in implementation. A critical gap lies in end users seeing, accepting, and acting upon AI-based recommendations.^6^ Previous research in human-AI interaction has focused heavily on health professionals as the sole recipients of AI recommendations, with less attention to implementing patient-centered AI systems.^7^ Our previous pre-implementation work for AI-based systems highlighted the importance of keeping patients informed regarding AI-informed recommendations to justify interventions and to support uptake.^8^
Patients and the public have important perspectives regarding AI implementation and want to be part of the conversation.^9–11^ However, their perspectives on centering patients in AI system implementation have been understudied compared to health professionals and AI developers.^7,8,12–17^ Moreover, previous studies have independently surveyed patient, health professional, and developer preferences about AI implementation. No studies to our knowledge, however, have collected richer qualitative data and combined their collective insights. Consequently, we lack integrative, practical guidance for those seeking to ethically implement and evaluate patient-centered AI systems.
It is also becoming more likely that patients may access AI output, even if not intended by AI developers. The U.S. 21st Century Cures Act, for example, prevents information blocking from patients, requiring organizations to give patients access to their electronic health information without delay or expense.^18^ This may result in a patient seeing a predictive AI risk score before discussing it with their healthcare team. AI is also increasingly used in tools to support shared decision-making with patients.^19^ While AI output may benefit patients, it may cause stress if not appropriately contextualized. AI can also be prone to hallucinations, the creation of false information, which may be challenging to differentiate from factual evidence.
Our objective was to triangulate perspectives from patients, developers, and health professionals for real-world implementation of patient-centered AI systems. We interviewed these three stakeholder groups using interview guides informed by bioethics and informatics models.^20^ To concretize discussions, we used an existing predictive AI tool developed by our team that proactively predicts a pregnant patient’s risk of postpartum depression (PPD) as a use case. Recruited patients and health professionals were potential users of the tool. PPD presents a complex bioethical case because of the sensitivity of the data and for the multi-layer autonomy; in pregnancy, the autonomy, harms, and benefits to the perinatal patient, newborn or fetus, and partner must be weighed simultaneously.^11,12^ Our study provides novel, data-driven recommendations for how AI may be ethically implemented to support patient-centred care.
RESULTS
Participant Characteristics
Table 1 provides demographic data from each stakeholder group (N = 36).
Emerging themes
We inductively derived emerging themes for implementing patient-centered AI systems that cut across our overarching framework for analysis, Sittig and Singh’s Socio-technical Model for Studying Health Information Technology in Complex Adaptive Healthcare Systems (Table 2)^20^. We describe the detailed emerging themes with the most illustrative quotes from developers (DV), health professionals (HP), and patients (PT).
Mitigating harm
All participant roles stressed the importance of ensuring minimal harm to end users (e.g., patients, health professionals) related to AI. One primary source of harm discussed involved stigmas driven by AI-based predictions. For example, predicting risk for mental health conditions or addictions (e.g., opioid use disorder) could change patient care trajectories. Patients expressed fear that risk predictions of mental health issues could lead to child protective services (CPS) interventions.
I may run a 100 score and it’s like, ‘oh i passed’. Like, why is the doctor coming to talk to me? And ACS (local CPS department) is coming to take my child?- PT12
Participants also raised the concern about model bias, noting the importance of utilizing representative training data and valuing fairness equally to accuracy.
I’m sure they’d be curious if their ethnicity is put in there…But what if there is some type of bias in the tool?- HP02
Patients and health professionals viewed AI as potentially harmful due to the stress that high-risk predictions may cause patients. Participants described the importance of involving health professionals and patients in the early stages of AI development to identify and mitigate these harms.
The patient is going to develop that insight and be on board… and lead to like a more … patient-centered treatment.- DV08
Clinical benefit and utility
All groups expressed that AI must provide clinical benefits to patients, care partners, health professionals, or health systems. Participants agreed that for models to provide utility, a health professional or patient must be able to easily take action (e.g., making a referral, prescribing a medication, contacting their provider) based on AI’s output. Patient and health professional participants seemed most comfortable with AI that could “run in the background” and provide support to human decision-makers as needed.
If it can explain its reasoning, I feel like that’s more helpful…I like to think of AI like as a tool. So if it was actually like teaching me and…I can learn what those risk factors are and take the time, then I would find it way more useful.- PT16
For the tool discussed (predictive AI for PPD), patient participants were typically open to their providers using the tool as an additional data point and accepting treatment based on the AI and their doctor’s input. However, one patient was very averse to using the tool, indicating the preference-sensitive nature of AI use in clinical care.
I would be confused because I wouldn’t believe that they could figure that out…it seems so bizarre. I probably would lose a bit of trust.-PT09
Translating predictive models into action also requires a threshold for action. Patient participants, however, had challenges understanding what the numeric risk predictions meant practically and why there were certain thresholds for action (e.g., the tool recommended a mental health referral if the PPD risk was > 30%).
0 to 30%, you know, that’s a closer gap. And then you have like this gap from 32 to 100, but it’s like 40, 50, 60, 70. And I’m assuming the prevention treatment is starting at either 75 or 80. And I was like, what about those people in the middle?- PT12
To trust AI and promote relevant actions, most end users wanted to understand the accuracy of AI. Ideally, patients wanted to know how accurate it was for them individually. However, some patients did not need to see this information themselves but trusted health professionals to make judgments on when AI was safe for clinical use.
I assume that [if] it’s in my patient portal, I’m thinking that it’s accurate for me.- PT01
Developers noted a tension between high performance and making understandable models that people wanted to use.
Interviewer: Accuracy versus understandability and explainability, and if you could only choose one, which one would you choose and why?
DV01: We need both, you can’t really do it without both, but when forced…the majority of the crowd choose understandability.
Participants described different strategies for ensuring models provided benefits. First, health professionals need to support clinical validation and interrogate potential biases. Participants also highlighted the need to investigate and plan for how AI may alter existing workflows. Updates would then need to be implemented in line with institutional norms and policies.
Developers viewed implementation and ensuring utility as a continuous process that would require updates over time, similar to any traditional software. Developers also acknowledged the importance of end-user feedback throughout AI model development. Although they did not always feel they had the skills to include this feedback, particularly related to patient users.
I think one piece that’s definitely missing in my research is patient perspectives about whether they think this kind of tool would be useful…I think that those questions have to be asked very carefully…But I don’t know that developers should be the ones actually going in to ask those questions.- DV07
Communicating AI Models
Several questions emerged regarding if, when, where, and how AI-related information should be communicated to patients. Patients had differing perspectives regarding how they would like to view AI output, with some preferring to see it before clinical encounters and others wanting someone to explain it to them. Multiple participants agreed that patients would need support in interpreting information and suggested that the provider may be the best person to do this. However, they also noted that the provider may need training and dedicated time to do this effectively.
Who gets the alert, and what happens once you get an alert? If you’re going through all that, then how much time are you spending to explain it?- HP06
Others highlighted that interfaces should be presented in lay terms, accessible to different audiences. Feature importance was discussed at length - participants suggested conveying predictors of risk (e.g., medications, history of past illness) as both positives and negatives contributing to the patient’s total risk. Patients generally wanted to see all features, not only the modifiable predictors. Providing sensitive features (e.g., risks related to marital status, BMI) requires care but may stimulate educational conversations. It was also important to ensure the labels were understandable by patients, so using the EHR-based feature names (e.g., “thyroid preparations”, “hyperemesis”) may be insufficient.
Patients also reported varying opinions on their desire to see AI-based risk information. Some felt they had a right to see these risks, how accurate they were, and what their individual risk factors were. Others trusted their provider to see the information and make the related decisions.
Data quality
Participants described challenges related to ensuring data quality, primarily related to bias, missingness, out-of-date information, and shortcomings in interpreting unstructured data (e.g., clinical notes) with insufficient context.
These days…charts are not well updated… unless it’s thoughtfully updated, which it rarely is because hospital systems are far too busy for that kind of meticulousness, then I think that people are going to feel like I could see people being like, ‘where the hell did that come from?’- HP03
Missingness was noted to be particularly problematic in a perinatal context, where many may receive care for other specialties in different health systems.
Data security, privacy, and access
Participants agreed that the way the data is stored, the algorithm is computed, and displayed to end users must protect patient and health professional privacy. There was, however, a tension between making tools open source and protecting patient privacy, ensuring their autonomy over their data.
Many viewed external organizations, such as the Centers for Medicare and Medicaid, as having a responsibility for ensuring privacy (i.e., data de-identification) and also governing privacy rules, although it was not always clear as to which entity was responsible. Health organizations were also mentioned as having a role in supporting data privacy and promoting data access. There were other external organizations whose access to data (e.g., CPS/ACS) was viewed as detrimental.
Patients had different desires for accessing AI inputs and outputs, including through the patient portal, on mobile phones, via PDF, and secure email. Some also wanted the ability to share the information with chosen care partners, but this varied from person to person.
Others highlighted how the combination of perinatal and psychiatric concerns made privacy issues more sensitive. Some patients, for example, may be reluctant to disclose sensitive information due to stigma or fear, leading to data accuracy issues.
Whenever a pregnant woman talks about this type of information…that concerns like calling to Child Protective Services. That is a big privacy issue…clinicians worry about models raising severe alerts.- DV09
Participants working in pediatrics also noted that accessing maternal health information through a child’s chart can be challenging due to limitations in data linkage capabilities and due to confidentiality protections in the EHR for sensitive maternal data.^21^
Responsible AI practices and liability
Participants had various opinions about who was responsible for the safe development and implementation of AI. Participants mentioned responsible entities at various levels from insurers and device manufacturers to individual developers and health professionals.
There needs to be some responsible party who’s well informed, who’s making the decisions about if and how these tools are actually used and up to date on how well they’re actually being used in patient care as you introduce them- DV08
Many of the questions of responsibility stemmed from a desire to mitigate individual liability for health professionals. The prevailing perspective was that no single person or entity could be held responsible, and a structure of shared responsibility was necessary. Some perceived that determining safety for the use of an algorithm should fall to health professionals. Health professionals also highlighted the need for responsibility in terms of seeing and acting upon risk predictions. Developers, on the other hand, felt responsible for making systems with high predictive performance that also mitigated potential biases.
So a clinician needs to make an informed decision. In which case…the clinic is liable, as they would be for any misdiagnosis or incorrect treatment decision.- DV08
If we implement it then…somebody has to have ownership to it that you are responsible for this. And if the patient is seeing this information, somebody has to interpret for them.- HP06
Responsible practices mentioned included checking for bias and accuracy prior to implementation, as well as continuous monitoring to identify model drift and retrain models. The conversation surrounding ensuring accuracy could be challenging, however, as the gold standard for comparison may not always be clear.
DISCUSSION
AI implementation in health systems requires coordination between patients, clinicians, developers, and health systems administrators and leaders. Through interviews with nearly 40stakeholders representing these perspectives, we identified requirements implementation and use of patient-centered AI systems. We summarize our findings in preliminary requirements derived directly from stakeholders, shown in Table 3. Our results specific to end user perspectives on conveying AI-based risk of PPD overlap with Williams et. al’s recent qualitative study on a similar topic.^22^ However, our work extends upon their findings, incorporating developer perspectives and using PPD as a use case to make broader recommendations for patient-centered AI regardless of clinical context. Our findings also resonate with the recently released AI Code of Conduct for Health and Medicine from the National Academy of Medicine, related to: advancing benefit for humanity, ensuring equity, engaging impacted individuals, ensuring workforce wellbeing, monitoring performance, and supporting continuous learning.^23^ We describe practical next steps with data-driven insights for achieving these requirements across key stakeholder groups.
First, health professionals will require competencies to use AI effectively and safely in healthcare.^24^ Most patients reported that they wanted their health professionals to deliver predictive AI results, whereas most clinicians do not feel qualified to do so. Health professionals also highlighted the difficulty in interpreting AI output and the limited time during encounters. While some efforts have attempted to integrate AI competencies into medical and nursing education,^24^ far more work is needed to educate the existing workforce of health professionals.
Second, ur findings highlight how decisions made during the development process can have downstream impacts, for example, balancing explainability with accuracy, or addressing fairness. Model developers, at times, work in relative isolation from the health system leadership, clinicians, and patients who may ultimately adopt their model. Technical development is viewed as a foundational step with little input needed from other stakeholders. Rather, our findings suggest that because of the downstream implications of decisions made at the modeling stage, health professional and patient stakeholders should be included in the early stages of development and evaluation to ensure models prioritize the right values, are useful, and ethically sound.
Participants also raised issues related to how data completeness and timeliness may affect model accuracy. Similar to displaying significant model features, visualization may support end users in understanding when key data elements may be missing or outdated. A systematic review of 44 implemented predictive AI models highlighted the lack of attention to user workflow and providing predictive risks in a way that enhances rather than degrades cognitive processing.^12^ Future work may investigate generalizable best practices for displaying predictive AI models to work collaboratively with human end users.
Third, to provide clinical utility, predictive AI output needs to be actionable, as we have previously reported.^8^ For example, perinatal providers need a way to refer appropriate patients for psychiatric or social work evaluation. Participants noted several needs to promote actionability, including providing reasoning (i.e., risk factors) and the level of model accuracy. This information would allow them to weigh their expertise in conjunction with the model, and choose from multiple possible actions based on the patient’s risk factors. Patients wanted to understand individual risk factors, which could support shared decision-making conversations with providers regarding risk reduction. Participants also noted that meaningful thresholds for action based on the numeric risk prediction were needed. This is not done consistently in practice, and there is a lack of robust methods for determining these thresholds for actionability.
Fourth, patients in our study expressed a wide range of preferences and information needs related to interpretation of the model. Compared to clinician end users, less attention has been given to patients as end users of models. There are many scenarios in which patients may view model output, making their perspectives vital in considering how to display output. The harms of failing to incorporate their perspectives may include elevated worry and anxiety, increased outreach to care teams, and even unnecessary care visits.
Lastly, several other publications have provided detailed needs assessments for enhancing privacy, navigating liabilities, and devising regulations related to AI.^23,25–28^ Our findings reinforce that layers of shared governance, involving multiple stakeholder groups, will be necessary to address these challenging questions.
Our findings also suggest multiple important areas of future work. First, our study primarily focused on predictive AI models. Generative AI is being rapidly adopted in research and in healthcare settings. A recent systematic review identified over 200 studies that have used large language models (LLMs) for healthcare purposes, including patient education, recommendations, and guidance, customizing care plans, interpreting medical information, and facilitating patient-clinician communication.^29^ They reported positive findings relating to patient satisfaction but concerns about readability, accuracy, and bias. Thus, investigating patients’ needs and ability to use LLMs safely will be an important part of ensuring appropriate use in healthcare.
Additionally, the science for both predictive and generative AI has weighed heavily towards model development and validation, with significantly fewer studies evaluating real-world clinical implementation and health outcomes. Multiple perspective pieces have called for more implementation science studies,^30^ along with clinical trials that have thoughtful comparator arms and benchmarks representing the current state of the healthcare system.^31^ While improving clinical outcomes is the ultimate goal for most predictive AI systems, recent studies have highlighted that only measuring these outcomes may produce an incomplete picture, particularly when AI does not have the intended effect.^32^ We advocate for detailed tracking (e.g., via EHR log data) that may ascertain how AI impacts decisions, how it is accessed by patients, and the downstream impacts this may have on patient care. All of these metrics may not be assessed in a detailed manner, but having them available supports investigating “last mile” problems when highly accurate AI fails to improve clinical outcomes. This evidence is critically needed to inform continued surveillance and refinement of AI models and to guide strategies for operationalizing the broad guidelines and frameworks that professional bodies such as the National Academy of Medicine have published.^23^
Finally, there are notable gaps in patients’ expressed interest in understanding more details about model predictions, and the strategies that we presently have to provide this information in a clear and comprehensible way. Despite substantial interest in the explainability of AI, very little explainability work has considered patients as end users.^33^ Clinicians themselves may also struggle to determine how and when to follow AI recommendations, let alone how to deliver this information to patients.^34,356^ These findings point to the need to both equip health professionals, including nurses and providers, with AI-related competencies or “literacy.”^34,3524^
Limitations of this study include that we based part of our interview guide on an existing algorithm predicting postpartum depression; thus, findings may not generalize to other clinical contexts or populations. Additionally, though we strived to invite a diverse range of stakeholders to participate in interviews, some perspectives may have been underrepresented. Thus, future work building upon these findings to further investigate patient-centered AI across a range of clinical contexts and populations, with additional stakeholder groups, is needed.
CONCLUSION
Patients, health professionals, and AI developers provided important insights on AI implementation that considers patients as active end users. Participants described how to mitigate potential harms related to AI, how AI may provide meaningful benefits, recommendations, and new questions for communicating AI models, as well as challenges related to data quality, privacy, security, access, and liability. Based on our findings, we provide recommendations for patient-centered AI implementation that include engaging stakeholders throughout development (not just at the end), supporting health professionals with competencies for interpreting and communicating AI risks, and inclusively communicating AI in ways that also support taking relevant clinical actions.
METHODS
Ethics approval
All participants provided written informed consent. The Columbia University Institutional Review Board approved the study.
Setting, Study Design, and Sample
We conducted prospective qualitative interviews with AI developers, health professionals, and perinatal patients. Health professionals and patients were potential end users of the tool in our use case, and AI developers had relevant expertise but were not directly involved in development of the given tool. Table 4 describes the inclusion criteria and recruitment methods.
Data Collection
Our team iteratively developed interview guides (Supplemental file), combining insights from MITRE’s Ethical Framework for the Use of Consumer-Generated Data in Health Care and Sittig and Singh’s Socio-technical model.^20,36^ Experts in obstetrics, perinatal mental health, nursing, AI development, consumer informatics, and qualitative methods provided input. We piloted each guide before enrollment. We showed patient and health professional participants a mockup of how the algorithm from our use case (i.e., proactive prediction of postpartum depression) may be displayed to concretize the discussion (Fig. 1). The mockup was informed by a survey of over 500 perinatal participants.^37^ We found that participants trusted AI-based risk scores that included a concrete risk number (instead of phrases like “above average”), and that participants preferred number line graphics over numbers alone.
Three researchers trained in qualitative methods conducted all interviews via Zoom or telephone (NCB, PMD, ZR). Interviews lasted 30–60 minutes and were audio recorded. Participants were compensated $50. Following the interview, participants electronically completed a demographics survey.
Data Analysis
We conducted a directed content analysis using thematic analysis and the constant comparative process.^38^ In this paper, we focus on insights derived from the dimensions of the Sittig and Singh Socio-technical Model, which we first used to deductively organize the data, but with adapted definitions to suit our application to predictive AI.^20^ A group of three coders (NB, PD, ZR) first analyzed transcripts collaboratively. Two team members then coded each transcript independently. We then met to compare and resolve disagreements, using the third coder in cases where agreement could not be reached. We also reviewed transcripts for thematic saturation, ensuring our sample met this criterion based on the diminishing need to update code definitions. Once all transcripts had been coded, we reviewed the data code by code to mitigate code drift. One of the original coders (NB) and another team member (MRT) then reviewed each parent code to derive emerging themes that cut across the domains of the Sittig and Singh framework.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Science N, Technology Council. Preparing for the Future of Artificial Intelligence. Executive Office of the President; 2016. Accessed January 3, 2023. https://obamawhitehouse.archives.gov/sites/default/files/whitehouse_files/microsites/ostp/NSTC/preparing_for_the_future_of_ai.pdf
- 2Topol E. Deep medicine: how artificial intelligence can make healthcare human again. Deep medicine: how artificial intelligence can make healthcare human again. Published online 2019.
- 3Triantafyllidis AK, Tsanas A. Applications of Machine Learning in Real-Life Digital Health Interventions: Review of the Literature. J Med Internet Res. 2019;21(4):e 12286.30950797 10.2196/12286 PMC 6473205 · doi ↗ · pubmed ↗
- 4Ting DSW, Liu Y, Burlina P, Xu X, Bressler NM, Wong TY. AI for medical imaging goes deep. Nat Med. 2018;24(5):539–540.29736024 10.1038/s 41591-018-0029-3 · doi ↗ · pubmed ↗
- 5Zhou Q, Chen ZH, Cao YH, Peng S. Clinical impact and quality of randomized controlled trials involving interventions evaluating artificial intelligence prediction tools: a systematic review. npj Digital Medicine. 2021;4(1):154.34711955 10.1038/s 41746-021-00524-2PMC 8553754 · doi ↗ · pubmed ↗
- 6Walker SC, French B, Moore RP, Model-guided decision-making for thromboprophylaxis and hospital-acquired thromboembolic events among hospitalized children and adolescents: The CLOT randomized clinical trial. JAMA Netw Open. 2023;6(10):e 2337789.37831448 10.1001/jamanetworkopen.2023.37789 PMC 10576217 · doi ↗ · pubmed ↗
- 7Walsh CG, Mc Killop MM, Lee P, Harris JW, Simpson C, Novak LL. Risky business: a scoping review for communicating results of predictive models between providers and patients. JAMIA open. 2021;4(4):ooab 092.34805776 10.1093/jamiaopen/ooab 092PMC 8598291 · doi ↗ · pubmed ↗
- 8Benda NC, Das LT, Abramson EL, “How did you get to this number?” Stakeholder needs for implementing predictive analytics: a pre-implementation qualitative study. J Am Med Inform Assoc. 2020;27(5):709–716.32159774 10.1093/jamia/ocaa 021PMC 7647269 · doi ↗ · pubmed ↗