Spontaneous Hemarthrosis and Compartment Syndrome in an Elderly Female With Acquired Hemophilia A: A Case Report
Mohammed S Alam, Mahfuza Khan, Roxana Lazarescu

TL;DR
An elderly woman with no prior bleeding history developed severe joint bleeding and muscle swelling due to a rare autoimmune condition called acquired hemophilia A, which was successfully treated with specialized care.
Contribution
This case report highlights the importance of diagnosing acquired hemophilia A in elderly patients presenting with unexplained bleeding and prolonged aPTT.
Findings
A 79-year-old woman presented with elbow pain and swelling due to acquired hemophilia A, confirmed by prolonged aPTT and factor VIII deficiency.
The patient required fasciotomy due to compartment syndrome caused by intramuscular hematoma and hemarthrosis.
Successful treatment involved prothrombin complex concentrate, corticosteroids, and surgical intervention.
Abstract
Acquired hemophilia A (AHA) is a rare but life-threatening bleeding disorder caused by autoantibodies against factor VIII. Unlike congenital hemophilia, AHA often presents in older adults without a prior bleeding history, manifesting with spontaneous, severe bleeding into soft tissues, muscles, or joints. We report the case of a 79-year-old woman with osteoporosis and osteoarthritis who presented with progressive right elbow pain and swelling, initially suspected to be septic arthritis or synovial tumor. Her course was complicated by massive hemarthrosis, intramuscular hematoma, and compartment syndrome requiring fasciotomy. Laboratory evaluation revealed a prolonged activated partial thromboplastin time (aPTT), markedly reduced factor VIII activity, and the presence of inhibitors, confirming the diagnosis of AHA. The patient was successfully managed with prothrombin complex…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1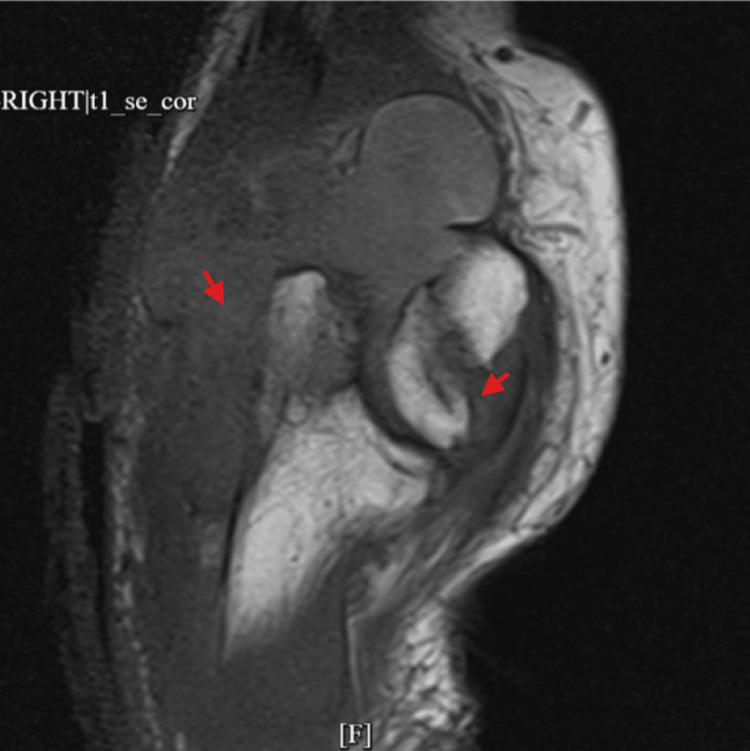 Figure 2
Figure 2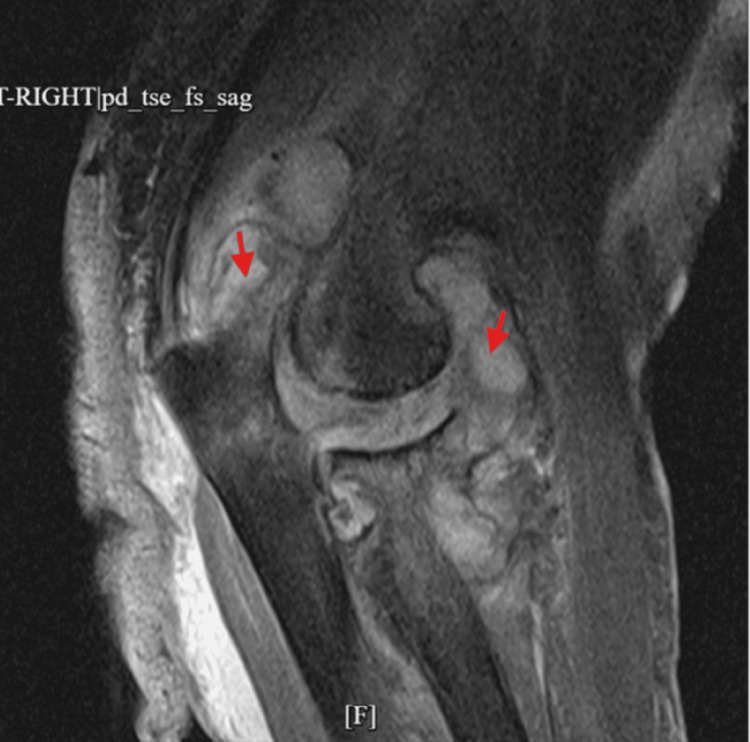 Figure 3
Figure 3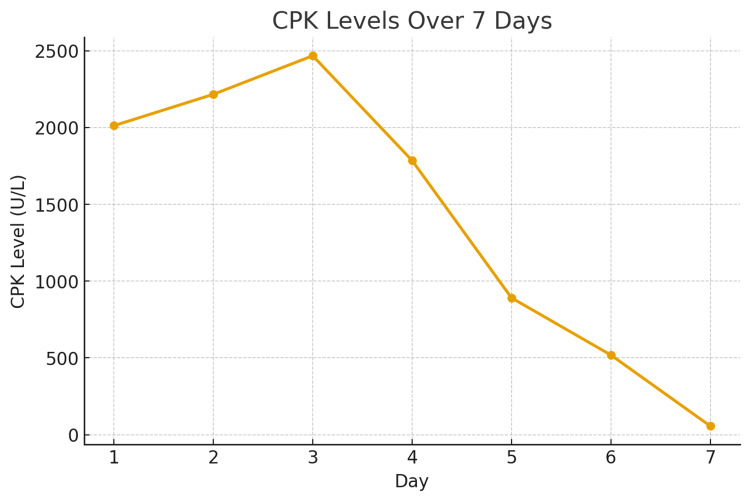 Figure 4
Figure 4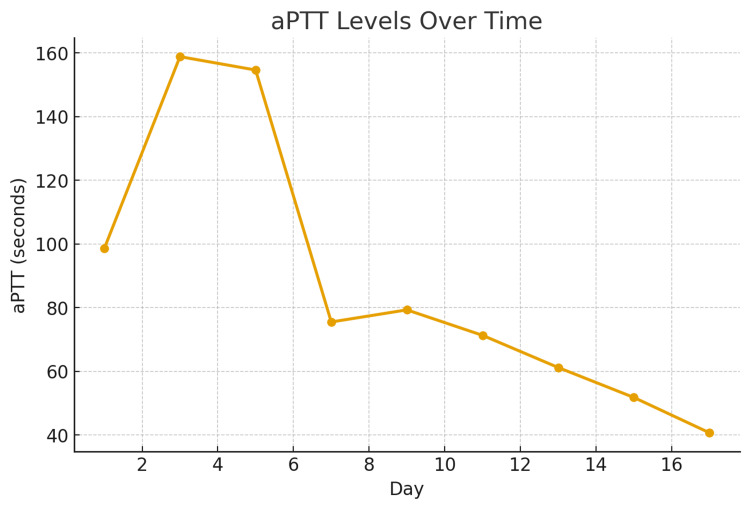 Figure 5
Figure 5| Parameters | Patient values | Reference range |
| Hemoglobin | 7 g/dL | 12–16 g/dL |
| Hematocrit | 22% | 36–46% |
| Platelet count | 154 × 10⁹/L | 150–400 × 10⁹/L |
| aPTT | 98.6 seconds | 25–35 seconds |
| PT/INR | Normal | PT: 11–14 seconds; INR: 0.8–1.2 |
| Factor VIII activity | 2% | 70–180% |
| Factor VIII inhibitor | Positive | Negative |
| Mixing study | No correction | Correction expected in deficiency |
| Lupus anticoagulant | Positive | Negative |
| CPK | 2,012 U/L | 26–192 U/L |
| Iron studies | Normal | Normal |
| Haptoglobin | 305 mg/dL | 34–200 mg/dL |
| Hepatitis A, B, C serologies | Negative | Negative |
| Acute lymphoma panel | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemophilia Treatment and Research · Coagulation, Bradykinin, Polyphosphates, and Angioedema · Blood Coagulation and Thrombosis Mechanisms
Introduction
Acquired hemophilia A (AHA) is a rare autoimmune disorder with an estimated incidence of 1-1.5 cases per million annually [1]. Most patients are elderly, and bleeding often presents spontaneously without trauma or a family history of bleeding disorders [2]. Delay in recognition increases morbidity and mortality due to uncontrolled bleeding or complications such as compartment syndrome [3-5]. AHA results from the development of inhibitory autoantibodies against clotting factor VIII, leading to impaired coagulation [6]. Misdiagnosis is common because clinical presentation can mimic septic arthritis, malignancy, or traumatic injury [7]. Management of AHA involves both hemostatic control and eradication of the inhibitor [8]. Here, we present a case illustrating this diagnostic challenge and its potentially limb-threatening consequences.
Case presentation
A 79-year-old woman with a history of osteoporosis and osteoarthritis presented to the emergency department with a two-week history of progressive pain and swelling in her right elbow. On arrival, her elbow was visibly swollen, warm, and tender, with marked limitation of movement. The swelling extended into her hand, which showed discoloration. The initial clinical impression raised concern for septic arthritis or a possible synovial tumor. Pain was described as progressive but not associated with systemic symptoms, which contrasts with septic arthritis (acute, severe pain with fever and elevated inflammatory markers) or malignancy (often chronic swelling with systemic features).
Laboratory investigations (Table 1) quickly shifted the diagnostic focus. Her activated partial thromboplastin time (aPTT) was markedly prolonged and failed to correct with a mixing study. Factor VIII activity was reduced to 2%, and a lupus anticoagulant was detected. In addition, her hemoglobin had fallen to 7 g/dL, and creatine kinase was elevated to over 2,000 U/L. Viral serology and lymphoma panel were negative.
Imaging supported a significant joint and soft tissue process. X-ray showed a large elbow effusion with soft tissue swelling (Figure 1). MRI revealed a large heterogeneous fluid collection with enhancing synovium, marrow edema, and intramuscular edema (Figures 2, 3). Ultrasound suggested a nonspecific intra- or extra-articular lesion.
X-ray of the right elbow showing large right elbow joint effusion with soft tissue swelling (red arrows).
MRI of the right elbow with and without contrast showing large, complex, heterogeneous, partially enhancing fluid and synovium within the elbow joint anteriorly and posteriorly (red arrows).
MRI of the right elbow with and without contrast showing large, complex, heterogeneous, partially enhancing fluid and synovium within the elbow joint anteriorly and posteriorly (red arrows).
A synovial biopsy was performed, but it only showed nonspecific changes without malignancy. Markedly prolonged aPTT uncorrected by mixing studies, severely reduced factor VIII activity, and a confirmed lupus anticoagulant established the diagnosis of AHA.
Her clinical course worsened as she developed compartment syndrome of the right upper extremity, requiring urgent fasciotomy and evacuation of a hematoma. Hematology confirmed the diagnosis of AHA, and treatment was started with prothrombin complex concentrate at 50 U/kg (3,000 units total) and prednisone 50 mg daily, with pantoprazole added for gastric protection. Rituximab was planned but deferred while awaiting family consent. Because of the anticipated prolonged course of corticosteroids, Bactrim prophylaxis was started to reduce the risk of Pneumocystis infection.
Over the following days, her bleeding stabilized with prothrombin complex concentrate (PCC) and prednisone. Her creatinine phosphokinase and aPTT gradually improved, though aPTT remained prolonged because of the coexisting lupus anticoagulant (Figures 4, 5). Her limb function improved after the fasciotomy, and she was able to begin rehabilitation. She was discharged home on prednisone with instructions for close hematology follow-up and weekly monitoring of factor VIII levels and inhibitor titers.
Graph showing CPK levels steadily decreasing over time.X-axis: hospital days. Y-axis: CPK in U/L.CPK: creatinine phosphokinase
Graph showing gradual declining of aPTT level over time.X-axis: hospital day. Y-axis: aPTT in seconds.aPTT: activated partial thrombplastin time
Discussion
AHA is a rare bleeding disorder caused by inhibitory autoantibodies against factor VIII. It typically affects the elderly and presents with spontaneous bleeding in soft tissues or mucous membranes, although hemarthrosis is less common than in congenital hemophilia [1,6,8]. While hemarthrosis is more commonly associated with weight-bearing joints such as the knee, it can also affect non-weight-bearing joints such as the elbow [9].
This case underscores that early recognition of AHA requires careful attention to subtle distinguishing features. Key clues include acute or progressive joint swelling without trauma, absence of systemic symptoms such as fever, and disproportionate bleeding relative to the apparent severity of joint findings. In this case, the patient presented with symptoms mimicking septic arthritis or a synovial tumor, initially delaying diagnosis. Septic arthritis was excluded based on synovial fluid analysis, which demonstrated bloody aspirate without evidence of infection, and negative cultures for bacterial growth [7]. Synovial tumor, including pigmented villonodular synovitis, was excluded on histopathological examination, which demonstrated hemorrhagic and fibrotic tissue without neoplastic features [7]. Hemarthrosis secondary to congenital or systemic coagulopathies was excluded, as the patient had no prior bleeding history and laboratory studies (prothrombin time, fibrinogen, platelets, liver function tests) were normal, making congenital hemophilia, von Willebrand disease, or consumptive coagulopathy unlikely [6]. This systematic exclusion of alternative causes supported the diagnosis of AHA, characterized by an isolated prolonged aPTT, reduced factor VIII activity, and the presence of factor VIII inhibitors [3,4]. Compartment syndrome due to intramuscular hematoma is an unusual but serious complication of AHA [3-5]. Prompt surgical decompression alongside hemostatic therapy is required to preserve limb function. Management of AHA involves both hemostatic control and eradication of the inhibitor. Bypassing agents (recombinant activated factor VII, activated PCC) or, less commonly, PCC can be used for bleeding control [7]. Immunosuppression with corticosteroids, rituximab, or cyclophosphamide is the mainstay of inhibitor eradication [2,8].
This case emphasizes the importance of considering AHA in elderly patients with unexplained bleeding and isolated prolonged aPTT, as timely hematology input can be life-saving.
Conclusions
AHA should be suspected in elderly patients with unexplained bleeding and prolonged aPTT uncorrected by a mixing study. Hemarthrosis in AHA is rare but may mimic septic arthritis or synovial tumors. Compartment syndrome from intramuscular hematoma is a rare complication requiring urgent surgical intervention. Optimal management requires both hemostatic therapy (PCC, recombinant activated factor VII). Awareness of this rare presentation is crucial for avoiding misdiagnosis and initiating timely, life-saving therapy. This report highlights that prompt suspicion based on atypical presentations and prolonged aPTT can prevent diagnostic delays and improve short-term and long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors' Organisation Blood Collins PW Hirsch S Baglin TP 1870187710920071704714810.1182/blood-2006-06-029850 · doi ↗ · pubmed ↗
- 2International recommendations on the diagnosis and treatment of patients with acquired hemophilia A Haematologica Huth-Kühne A Baudo F Collins P 5665759420091933675110.3324/haematol.2008.001743 PMC 2663620 · doi ↗ · pubmed ↗
- 3Illustrated operative management of spontaneous bleeding and compartment syndrome of the lower extremity in a patient with acquired hemophilia A: a case report J Med Case Rep Jentzsch T Brand-Staufer B Schäfer FP Wanner GA Simmen HP 132820142488603010.1186/1752-1947-8-132PMC 4109126 · doi ↗ · pubmed ↗
- 4Use of thrombolytic agents to treat neonatal thrombosis in clinical practice Blood Coagul Fibrinolysis Leong R Patel J Samji N Paes BA Chan AK Petropoulos JA Bhatt MD 1932003320223528544910.1097/MBC.0000000000001134 · doi ↗ · pubmed ↗
- 5Treatment of a compartment syndrome in the leg in an elderly patient with acquired hemophilia type A: a case report Int J Surg Case Rep Fonseca AF Herrera GA Gallego A Llinas PJ 10899911220233949140810.1016/j.ijscr.2023.108999 PMC 10667864 · doi ↗ · pubmed ↗
- 6Potential pitfalls in the diagnosis of Hb Handsworth in areas with high prevalence of Hb S Int J Lab Hematol Al Zadjali S Al-Riyami AZ Gravell D Al Haddabi H Al Rawahi M Al Falahi K Daar S 4884923620142416556310.1111/ijlh.12157 · doi ↗ · pubmed ↗
- 7A unique presentation of spontaneous compartment syndrome due to acquired hemophilia A and associated malignancy: case report and literature review World J Oncol Alidoost M Conte GA Chaudry R Nahum K Marchesani D 72751120203228477510.14740/wjon 1260 PMC 7141160 · doi ↗ · pubmed ↗
- 8Acquired haemophilia A: a 2013 update Thromb Haemost Franchini M Mannucci PM 1114112011020132400830610.1160/TH 13-05-0363 · doi ↗ · pubmed ↗