Electroporation for the Treatment of Pancreatic Ductal Adenocarcinoma: A Systematic Review of Preclinical and Clinical Studies
Gabriel Marcellier, Theo Le Berre, Paul Rivallin, Marie Frenea-Robin, Frédéric Prat

TL;DR
This paper reviews electroporation-based therapies for pancreatic cancer, finding electrochemotherapy and electroimmunotherapy promising while suggesting caution with irreversible electroporation.
Contribution
The study presents the largest systematic review to date on electroporation therapies for pancreatic ductal adenocarcinoma.
Findings
Electrochemotherapy showed promising safety and efficiency in preclinical and human models.
Irreversible electroporation had a 36% adverse event rate with a median survival of 17.2 months.
Electroimmunotherapy demonstrated significant immunotherapy potentiation in both preclinical and human models.
Abstract
Pancreatic ductal adenocarcinoma (PDAC) is a highly aggressive malignancy with poor prognosis and limited treatment options. Electroporation-based therapies, such as electrochemotherapy (ECT) and irreversible electroporation (IRE), could be promising alternatives. ECT combines reversible electroporation with chemotherapy, enhancing intracellular drug uptake, while IRE leads to nonthermal tumor ablation. Both have been suggested as immunotherapy potentiators (electroimmunotherapy) in some tumor locations. We conducted a systematic review to evaluate the efficiency and safety of ECT, IRE, and immunoelectroporation in PDAC treatment. We searched Medline, Embase, Cochrane, and Google-Scholar for ECT, IRE, and electroimmunotherapy following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. For ECT and electroimmunotherapy, regarding the scarcity of the data,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
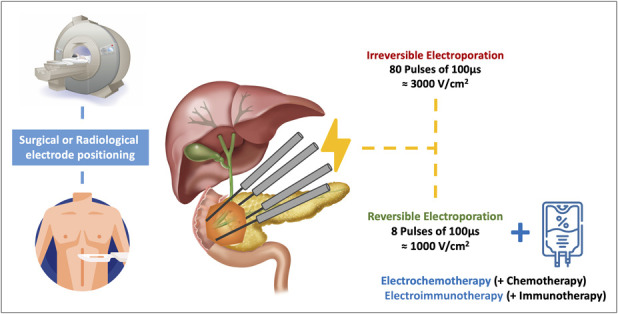 Figure 1
Figure 1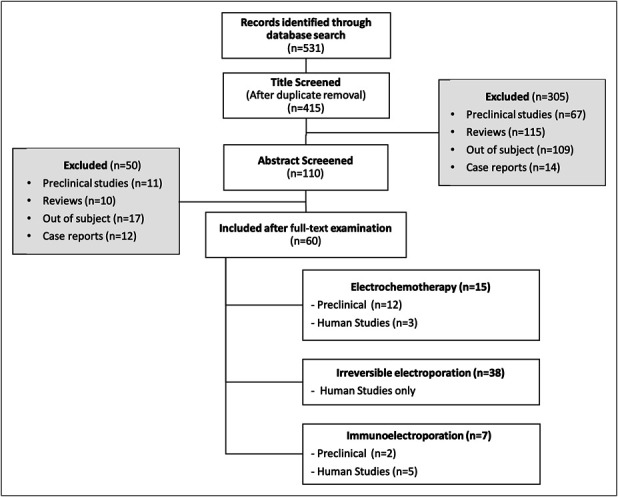 Figure 2
Figure 2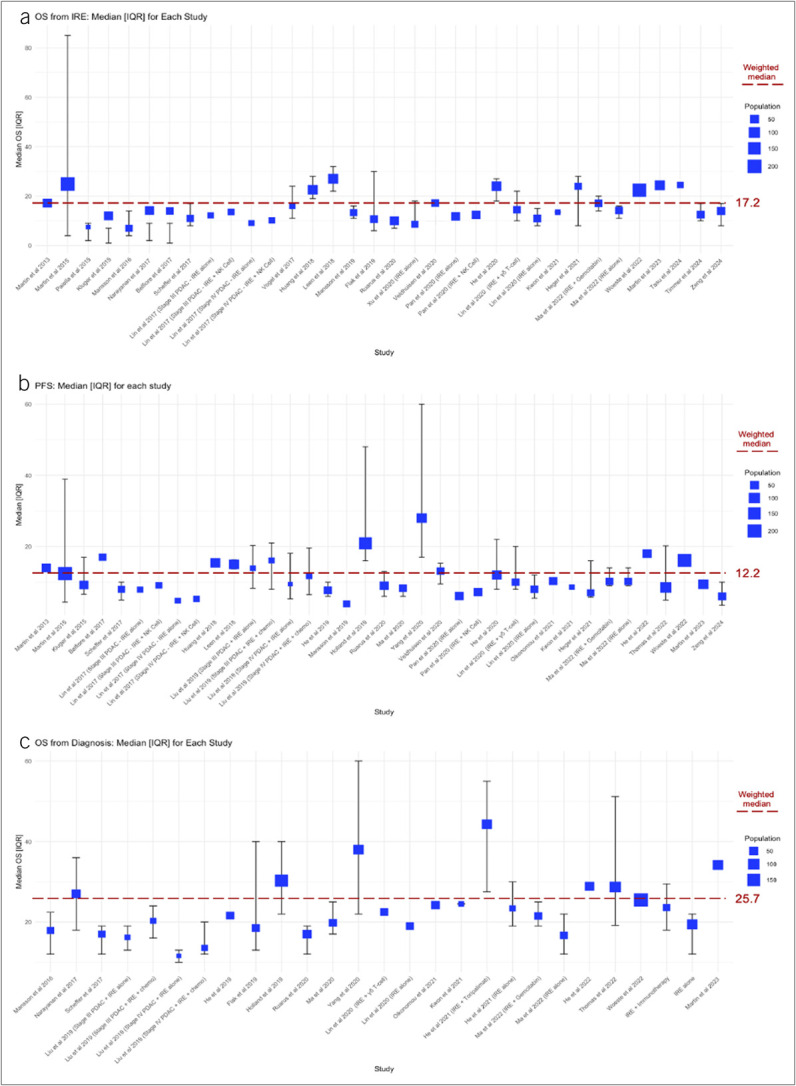 Figure 3
Figure 3| References | Model description | Drugs and electrical settings | Outcomes |
| Jaroszeski et al ( | Several cell lines | Different voltages (500–4,000 V/cm) | Ratios between IC50 with and without ECT were 700 for bleomycin, 12 for cisplatin, 2 for cytarabine, and 1.6 for carboplatin |
| Girelli et al ( | PANC1 and MiaPaCa2 human PDAC cells | ESOPE protocol (8 × 100 μs pulses at 1,000 V/cm) | Without chemotherapy, RE induced 4% cellular death and permeabilization of 90% of PANC1 cells and 75% of MiaPaCa2 cells |
| Fernandes et al ( | Human PANC1 cells | ESOPE protocol (8 × 100 μs pulses at 1,000 V/cm) | ECT significantly increased the lethality of bleomycin, cisplatin, and oxaliplatin on both PANC1 and Pan02 cells |
| Bosnjak et al ( | BxPC-3 human pancreatic cells | PEFs were delivered at 1,300 V/cm and 100 μs with a frequency of 1 Hz | ECT potentialized the effects of bleomycin and cisplatin |
| Michel et al ( | Several cell lines derived from pulmonary metastasis of PDAC | Cisplatin | On the pulmonary metastasis cell lines, ECT improved the efficiency of cisplatin, even if the cells were cisplatin-resistant before ECT |
| Girelli et al ( | Non pathological rabbit's pancreas | ESOPE protocol for PEFs | Transaminase and amylase levels were not significantly modified, and all rabbits survived procedures |
| Dezman et al ( | Electroporation on porcine pancreas | Surgical (laparotomy) electrode positioning in the pancreatic head and tail | 2 pigs presented a transitory increase in pancreatic enzymes levels |
| Stupan et al ( | Electroporation on porcine blood vessels | PEFs delivered on several locations and vascular surgical anastomosis (portal vein, inferior vena cava) | CT scans found no vascular thrombosis despite ECT but some anastomoses were strictured (possibly because of technical difficulties during procedures) |
| Dev et al ( | Human PANC3 cells were implanted subcutaneously on nude mice | Bleomycin ECT | Mice treated with ECT had tumor size decrease, while size increased in mice treated with bleomycin alone |
| Nanda et al ( | Human cells implanted subcutaneously in nude mice | ECT with bleomycin, mitomycin, and carboplatin | Neither PEFs alone nor drugs alone were effective |
| Jaroszeski et al 1999 ( | Hamsters with PDAC PC-1 cells orthotopic and subcutaneously injected | Bleomycin | No response for drug or PEF alone |
| Dev et al ( | Human PDAC cells subcutaneously injected in nude mice | ECT with bleomycin, mitomycin, and carboplatin | Complete response rate at day 89 |
| References | Patients | Drugs | Electrical settings | Outcome |
| Granata et al ( | Clinical phase I–II studies | Chemotherapy: All patients received systemic chemotherapy prior ECT (gemcitabine + oxaliplatin or 5 FU-irinotecan-oxaliplatin) | Pancreatic access threw median laparotomy and positioning of 6 peripheric needles around the tumor and 1 central electrode | No serious adverse event occurred |
| Izzo et al ( | Prospective phase I–II studies | Overall survival of 11.5 mo with better survival when electrodes were manually positioned and adapted to the tumor rather than if they had a predefined geometry (but not significant) | ||
| Casadei et al ( | Stable patients with LAPC pretreated with chemotherapy + radiotherapy | Chemotherapy: 6 cycles before and 3 after ECT with either FOLFIRINOX or gemcitabine + nab-paclitaxel | Laparotomic positioning of electrodes (number and position according to tumor) | Reduction in tumor size but not in vascular encasement (no downstaging) |
| Cebron et al ( | Resectable PDAC (head of pancreas) | ECT: bleomycin 15 mg/m2 IV injected 8 min before electroporation | Surgery followed by intraoperative electroporation with 2 plate electrodes of 30 mm separated by 8 mm | No AEs related to ECT per or post procedure |
| No. | Reference | Patients | Protocol | Outcome | Safety | Other | ||||||||||||||||||||||||||
| Patients treated with IRE (n) | Age (mean) | Stage | Largest tumor diameter (cm) | Prospective (Y/N) | Pretreatment with chemotherapy (%) | Electrode positioning (PC/SUR) | OS from IRE (median) | IQR | PFS (median) | IQR | OS from diagnosis (median) | IQR | HS (d) | Patients with AEs (n) | SAEs (n) | Pancreatic/biliary fistula | Ascite | Pain | Pleural effusion | Pancreatitis | Thrombosis | Hemorrhage | Delayed gastric emptying | Splenic infarction | Fever | Infection | Digestive perforation | Biliary stricture | Death | |||
| 1 | Martin et al ( | 54 | 61 | III | NA | Y | 91 | SUR | 17.2 | NA | 14 | NA | NA | NA | NA | 32 | 9 | 2 | 3 | 0 | 3 | 0 | 6 | 3 | 2 | 0 | 0 | 6 | 0 | 0 | 0 | |
| 2 | Martin et al ( | 200 | 62 | III | 2.8 | Y | 100 | SUR | 24.9 | 4.9–85 | 12.4 | 4.4–38.9 | NA | 6 | 74 | 42 | 1 | 0 | 0 | 0 | 1 | 13 | 0 | 0 | 1 | 0 | 18 | 0 | 0 | 3 | #1 | |
| 3 | Paiella et al ( | 10 | 66 | III | 3 | Y | 100 | SUR | 7.5 | 2.9–15.9 | NA | NA | NA | NA | 9.5 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| 4 | Kluger et al ( | 50 | 66.5 | III | 3 | Y | 100 | SUR | 12.03 | 7.7–23.1 | 9.2 | 6.6–16.98 | NA | NA | 6 | 29 | 16 | 2 | 1 | 0 | 0 | 0 | 2 | 6 | 3 | 0 | 0 | 3 | 1 | 1 | 6 | #2 |
| 5 | Mansson et al ( | 24 | 65 | III | 2.75 | Y | 100 | PC | 7 | 4–14 | NA | NA | 17.9 | 12–22.4 | 5 | 11 | 3 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 6 | Narayanan et al ( | 50 | 62.5 | III | 3.2 | N | 100 | PC | 14.2 | 9.7–16.2 | NA | NA | 27 | 18–36 | NA | 21 | 10 | 0 | 0 | 19 | 0 | 6 | 3 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| 7 | Belfiore et al ( | 29 | 68 | III | 5.65 | N | 100 | PC | 14 | 9.9–18.1 | 17 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 8 | Scheffer et al ( | 25 | 61 | III | 4 | Y | 100 | PC | 11 | 8–17 | 8 | 5–10 | 17 | 12–19 | 3 | 10 | 2 | 1 | 0 | 3 | 0 | 1 | 0 | 1 | 2 | 0 | 0 | 1 | 0 | 3 | 0 | #3 |
| 9 | Lin et al ( | 67 | 57 | III + IV | 4.9 | N | 73 | PC | NA | 22 | 0 | 0 | 0 | 17 | 0 | 0 | 0 | 0 | 4 | 0 | 22 | 0 | 0 | 0 | 0 | #4 | ||||||
| IRE alone | 16 | III | 12.2 | NA | 7.9 | NA | NA | NA | ||||||||||||||||||||||||
| IRE + NK cell | 19 | III | 13.6 | NA | 9.1 | NA | NA | NA | ||||||||||||||||||||||||
| IRE alone | 14 | IV | 9.1 | NA | 4.8 | NA | NA | NA | ||||||||||||||||||||||||
| IRE + NK cell | 18 | IV | 10.2 | NA | 5.3 | NA | NA | NA | ||||||||||||||||||||||||
| 10 | Vogel et al ( | 15 | 64 | III | 4.1 | Y | 100 | SUR | 16 | 11–24 | NA | NA | NA | NA | NA | 8 | 8 | 4 | 0 | 0 | 0 | 0 | 2 | 0 | 3 | 0 | 0 | 0 | 0 | 1 | 0 | |
| 11 | Huang et al ( | 70 | NA | III | NA | N | 100 | SUR | 22.6 | 19–28 | 15.4 | NA | NA | NA | NA | 13 | 3 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| 12 | Leen et al ( | 75 | 63.4 | III | 3.47 | Y | 100 | PC | 27 | 22–32 | 15 | 13.7–16.3 | NA | NA | NA | 19 | 1 | 0 | 0 | 15 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | #5 |
| 13 | Liu et al ( | 54 | 61 | III + IV | 4.97 | Y | NA | PC/SUR | NA | 15 | 4 | 0 | 15 | 6 | 14 | 0 | 1 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | |||||||
| III + IRE alone | 13 | III | NA | NA | 13.9 | 8.3–20.2 | 16.2 | 13–19 | ||||||||||||||||||||||||
| III + IRE + chemo | 15 | III | NA | NA | 16.1 | 8–21 | 20.3 | 16–24 | ||||||||||||||||||||||||
| IV + IRE alone | 10 | IV | NA | NA | 9.45 | 5.3–18.1 | 11.6 | 10–13 | ||||||||||||||||||||||||
| IV + IRE + chemo | 16 | iV | NA | NA | 11.7 | 6.6–19.6 | 13.56 | 12–20 | ||||||||||||||||||||||||
| 14 | He et al ( | 36 | NA | III | NA | N | 100 | PC | NA | NA | 7.7 | 6–10 | 21.6 | NA | NA | 23 | 0 | 0 | 1 | 2 | 0 | 0 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 15 | Mansson et al ( | 24 | 68 | III | NA | Y | 100 | PC | 13.3 | 11–16 | 3.9 | NA | NA | NA | 5 | 6 | 6 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | |
| 16 | Flak et al ( | 33 | 67.1 | III | 3 | Y | 100 | PC | 10.7 | 6–30 | NA | NA | 18.5 | 13–40 | 1 | 21 | 8 | 0 | 2 | 3 | 0 | 0 | 1 | 2 | 0 | 0 | 0 | 3 | 0 | 0 | 2 | |
| 17 | Holland et al ( | 152 | 62 | III | 2.7 | Y | 100 | PC | NA | NA | 20.9 | 16–48 | 30.3 | 22–40 | 27 | 26 | 0 | 0 | 0 | 4 | 4 | 3 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 3 | ||
| 18 | Ruarus et al ( | 50 | 61 | III + REC | 4 | Y | 100 | PC | 10 | 7.5–11 | 9 | 6–13 | 17 | 12–19 | 4 | 29 | 21 | 1 | 0 | 2 | 0 | 3 | 3 | 0 | 3 | 0 | 0 | 3 | 1 | 4 | 2 | |
| 19 | Ma et al ( | 33 | 64 | III | 4.1 | Y | 100 | PC | NA | NA | 8.3 | 6–9 | 19.8 | 17–25 | NA | 3 | 3 | 0 | 2 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 0 | O | 0 | 0 | 0 | #6 |
| 20 | Xu et al ( | 42 | 58 | III | 4 | N | 100 | PC | NA | 3 | 2 | 2 | 0 | 0 | 0 | 3 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | |||||||
| IRE alone | 22 | 8.6 | 8–18 | NA | NA | NA | NA | |||||||||||||||||||||||||
| IRE + chemotherapy/radiotherapy | 20 | NA | NA | NA | NA | NA | NA | #7 | ||||||||||||||||||||||||
| 21 | Yang et al ( | 74 | 62 | III | 3.8 | Y | 100 | SUR | NA | NA | 28 | 17–60 | 38 | 22–60 | NA | 13 | 9 | 1 | 8 | 0 | 0 | 0 | 0 | 7 | 11 | 0 | 0 | 1 | 0 | 0 | 0 | |
| 22 | Veldhuisen et al ( | 30 | 62 | III | 3.8 | N | 100 | PC | 17.2 | 10.7–18.9 | 13.1 | 9.5–15.3 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 23 | Pan et al ( | 92 | 57 | III | 4.2 | Y | NA | PC | NA | NA | 7.7 | 31 | NA | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 31 | 0 | 0 | 0 | 0 | #8 | ||||
| IRE alone | 46 | 11.8 | NA | 6.1 | NA | NA | NA | |||||||||||||||||||||||||
| IRE + NK cell | 46 | 12.4 | NA | 7.2 | NA | NA | NA | |||||||||||||||||||||||||
| 24 | He et al ( | 64 | 58.5 | III | 3.95 | N | 100 | PC | 24 | 18–27 | 12 | 8–22 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 25 | Lin et al ( | 62 | 62 | III | 4 | Y | 84 | NA | NA | 31 | 14 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 | #9 | ||||||
| IRE + γδ T-cell | 30 | 14.5 | 10–22 | 10 | 8–20 | 22.5 | ||||||||||||||||||||||||||
| IRE | 32 | 11 | 8–15 | 8 | 5.5–12 | 19 | ||||||||||||||||||||||||||
| 26 | Oikonomou et al ( | 40 | 65.2 | III | 3.8 | N | 83 | SUR | NA | NA | 10.3 | NA | 24.2 | NA | NA | 8 | 11 | 8 | NA | NA | NA | NA | NA | NA | 3 | NA | NA | NA | NA | NA | NA | |
| 27 | Kwon et al ( | 12 | 64 | III | 3.1 | N | SUR | 13.5 | NA | 8.6 | NA | 24.5 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 1 | ||
| 28 | He et al ( | 85 | 57.84 | III | 3.5 | N | 100 | PC | NA | 13 | NA | 13 | 0 | 12 | 0 | 10 | 3 | 0 | 3 | 0 | 0 | 10 | 0 | 0 | 0 | |||||||
| IRE + toripalimab | 70 | NA | NA | NA | NA | 44.3 | 27.5–55 | |||||||||||||||||||||||||
| IRE alone | 15 | NA | NA | NA | NA | 23.4 | 19–30 | |||||||||||||||||||||||||
| 29 | Heger et al ( | 25 | 58 | III + REC | NA | N | 100 | SUR | 24 | 8–28 | 7 | 5.8–16 | NA | NA | 7 | 20 | 3 | 1 | 6 | 0 | 0 | 2 | 1 | 1 | 0 | 0 | 0 | 20 | 0 | 0 | 0 | #10 |
| 30 | Ma et al ( | 61 | 64 | III | 4 | N | 100 | PC | NA | 20 | 4 | 0 | 27 | 39 | 8 | 2 | 0 | 1 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | |||||||
| IRE + gemcitabin | 31 | 17.1 | 14–20 | 10.2 | 9–14 | 21.5 | 19–25 | |||||||||||||||||||||||||
| IRE alone | 30 | 14.2 | 11–16 | 10.2 | 9–14 | 16.7 | 12–22 | |||||||||||||||||||||||||
| 31 | He et al ( | 53 | 57.5 | III | NA | N | 100 | PC | NA | NA | 18 | NA | 28.9 | NA | 9 | 10 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| 32 | Thomas et al ( | 100 | NA | III | NA | N | 100 | NA | NA | NA | 8.51 | 4.95–20.2 | 28.71 | 19.17–51.19 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | #11 |
| 33 | Woeste et al ( | 187 | 62 | III | NA | N | 100 | SUR | 22.4 | NA | 16.1 | NA | 25.5 | NA | NA | 49 | 48 | 1 | 5 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 2 | 6 | 0 | 0 | 6 | |
| 34 | Ma et al ( | 103 | NA | III | 4.1 | N | 100 | PC | NA | 80 | 36 | 26 | 12 | 80 | 6 | 34 | 0 | 19 | 0 | 0 | 18 | 0 | 0 | 0 | 0 | |||||||
| IRE + immunotherapy | 25 | NA | NA | NA | NA | 23.6 | 18–29.5 | |||||||||||||||||||||||||
| IRE alone | 78 | NA | NA | NA | NA | 19.4 | 12–22 | |||||||||||||||||||||||||
| 35 | Martin et al ( | 75 | 61 | III | 2.9 | Y | 100 | SUR | 24.4 | NA | 9.4 | NA | 34.2 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | #12 |
| 36 | Tasu et al ( | 17 | 61 | III | NA | Y | 100 | PC | 24.5 | NA | NA | NA | NA | NA | NA | 10 | 25 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | #13 |
| 37 | Timmer et al ( | 34 | 65 | III | NA | Y | 100 | PC | 12.5 | 10.9–17 | NA | NA | NA | NA | NA | 19 | 8 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | #14 |
| 38 | Zeng et al ( | 38 | 67.7 | IV | 4.29 | Y | 100 | PC | 14 | 8–17 | 6 | 3.5–10 | 0 | 0 | 5.9 | 13 | 4 | 0 | 0 | 13 | 0 | 1 | 0 | 1 | 1 | 0 | 10 | 0 | 0 | 1 | 0 | #15 |
| Parameter | Calculation | Value | Population, N () |
| Population | 2,245 | ||
| Age (median in years) | Weighted mean | 61.7 | 1,936 (82) |
| Largest tumoral diameter (median size in cm) | 3.6 | 1,645 (73) | |
| Tumor stage | Total population (% of the population) | ||
| III (LAPC) | 2,149 (96) | 2,245 (100) | |
| IV (metastatic) | 96 (4) | ||
| Study protocol | |||
| Prospective | Total population (% of the population) | 1,191 (53) | |
| Retrospective | 1,054 (47) | 2,245 (100) | |
| Randomized | 96 (4) | ||
| Pretreated with chemotherapy (%) | Weighted mean | 98 | 2,087 (93) |
| Electrode positioning | Total population (% of the population) | ||
| Surgical | 839 (41) | 2,056 (92) | |
| Percutaneous | 1,217 (59) | ||
| Outcome | |||
| OS from IRE (median) | Weighted mean | 18.2 | 1,495 (67) |
| OS from diagnosis (median) | Weighted mean | 26.3 | 1,309 (58) |
| PFS from IRE (median) | Weighted mean | 12.8 | 1,832 (82) |
| Safety | |||
| Patients experiencing adverse event | Total population (% of the population) | ||
| Studies where it is clearly cited | 495 (26) | 1,342 (60) | |
| Filling the missing data | 699 (36) | 1,935 (86) | |
| Severe adverse events | 327 (19) | 1,705 (76) | |
| Main IRE-related adverse events | 1,935 (86) | ||
| Pancreatic/biliary fistula | 66 (3.4) | ||
| Ascites | 82 (4.2) | ||
| Pain | 213 (11) | ||
| Pleural effusion | 37 (1.9) | ||
| Pancreatitis | 71 (3.7) | ||
| Thrombosis | 44 (2.3) | ||
| Hemorrhage | 50 (2.6) | ||
| Delayed gastric emptying | 43 (2.2) | ||
| Splenic infarction | 1 (0.1) | ||
| Infection | 82 (4.2) | ||
| Biliary stricture | 11 (0.6) | ||
| Digestive perforation | 2 (0.1) | ||
| Death | 25 (1.3) | ||
| Hospital stay (median stay in days) | Weighted mean | 6 | 624 (28) |
| References | Model description | Drugs and electrical settings | Outcomes |
| Narayanan et al ( | Immunocompetent mice with subcutaneous injection of PDAC cells from KPC mice | No immunotherapy injection but assessment of the immune response induced by IRE | IRE alone significantly inhibited tumor growth compared with controls and induced systemic adaptive immune response which is promising regarding potential benefits of IRE + immunotherapy |
| Zhao et al ( | Murine model with orthotopic PDAC | IRE with anti-PD1 immune checkpoint blockade | Promotes selective tumor infiltration by CD8+ T cells |
| Human studies | |||
| Lin et al ( | Unresectable PDAC (stage III, 19 patients; IV, 18 patients) | IRE with allogenic natural killer cell immunotherapy | No major adverse events were described |
| He et al ( | Unresectable PDAC (stage III, 70 patients) | IRE alone against IRE + toripalimab (antiPD1) | Description of an IRE-based immunomodulatory effect ( |
| Lin et al ( | Unresectable PDAC (stage III, 30 patients) | IRE alone against IRE + adjunction of γδ-T cell | Improved survival in the immunotherapy arm |
| Ma et al ( | Unresectable PDAC (stage III, 25 patients) | IRE alone against IRE with PD1 or PDL1 | OS was significantly improved in the immunotherapy arm compared with the IRE arm |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicrobial Inactivation Methods · Plant tissue culture and regeneration
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) represents one of the main causes of cancer mortality in western countries (1), with a 5-year survival rate of approximately 13% (American Cancer Society based on data from 2014 to 2020). Its constantly rising incidence combined with steady mortality rates despite therapeutic advances in oncology is expected to make it the second leading cause of cancer mortality by 2030 in some western countries (2) and a major public health issue worldwide (3).
The poor prognosis of PDAC is related to several factors. One is the absence of early diagnostic markers, which results in most cases being detected at locally advanced (stage III, locally advanced pancreatic cancer [LAPC]) or metastatic (stage IV) stages, when curative surgery is rarely feasible. Another is the presence of a dense, immunosuppressive tumor microenvironment (TME) that limits the effectiveness of most medical treatments (radiotherapy and chemotherapy) and acts as a barrier to immunotherapy (1).
The search for physical processes that disrupt the TME to improve chemosensitivity and/or allow immunomodulation could lead to survival improvement in PDAC.
Electroporation is based on the use of pulsed electric fields (PEFs), very high-voltage, short-duration current actuations that open up cell membrane nanopores, either temporarily (reversible electroporation [RE]) or permanently (irreversible electroporation [IRE]), depending on the duration and intensity of the current applied.
In preclinical studies, a succession of 8 × 100 μs PEFs with an amplitude of 100–1,000 V/cm^2^ results in RE, while a succession of 80–100 PEFs around 3,000 V/cm^2^ exceeds the cell's adaptive capacity and results in IRE by electrolyte disturbance and cellular apoptosis (4,5) (Figure 1). Although RE does not cause cell death per se, it can enhance the cellular penetration of cytotoxic molecules. The use of RE to improve the effects of chemotherapy is thus called electrochemotherapy (ECT) (6). Effects of PEF on TME and the immune response to cancer invasion and metastasis have also been proven (electroimmunotherapy) (7). The exact mechanisms leading to cellular permeabilization under electrical fields remain an area of controversy, but electroporation has been used since 1968 for cellular transfer of DNA, pasteurization, and more recently cancer treatment with prostate, skin cancer, Kaposi sarcoma, among other recognized indications. The potential benefits of RE and IRE for the treatment of PDAC have logically been investigated. We conducted a systematic review of the clinical and preclinical literature on uses of electroporation for the treatment of PDAC.
Electroporation for the treatment of human pancreatic ductal adenocarcinoma. Electrodes are positioned either surgically or under radiological control. 8–80 pulses of 1,000–3,000 V/cm2 are then applied to perform reversible or irreversible electroporation. The combination of reversible electroporation and chemotherapy or immunotherapy is, respectively, defined as electrochemotherapy or electroimmunotherapy.
METHODS
Screening methodology
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines for systematic reviews (8).
We searched articles regarding 3 major topics:
- ECT in PDAC, defined by the use of RE to potentiate a cytotoxic agent. Regarding the scarcity of the human studies describing ECT for PDAC, we included preclinical works on in vitro and murine models.
- IRE in PDAC. We focused on the human data describing the outcomes of IRE for PDAC treatment. Studies describing IRE for other neoplasm than PDAC, preclinical studies testing IRE on in vitro or in vivo models, feasibility studies, clinical protocols without any survival outcome (see below), and literature reviews were excluded from the systematic review. We also excluded case reports and case report compilations of less than 5 patients per category as judged too small to allow for survival calculations.
- Electroimmunotherapy, defined by the use of electroporation to enhance immunotherapy. A very few studies are available on this topic, so we included preclinical and human studies implying reversible and/or IRE. Immunotherapy was defined as based on any drug aiming to improve the immune response against the tumor. We therefore present an exhaustive “state-of-the-art” review of preclinical and clinical studies.
Two physicians (F.P. and G.M.) from our unit went manually and independently through the below-mentioned databases. Keywords used for the research were pancreatic cancer, PDAC, electroporation, and ECT. Articles were screened from 1997 to 2024 across several databases (Medline, Cochrane Library, Embase, and Google Scholar). Databases were last checked on December 31, 2024.
Data collection
For ECT and electroimmunotherapy, since the small number of studies did not allow statistical analysis, we reported individually the main available data from each preclinical or clinical study. We reported the type of drug used in association with electroporation and the electrical settings. If available, we also presented survival outcomes.
For IRE, due to the larger set of clinical data, only clinical studies were analyzed, with the following information being retrieved as available:
- Patients and methodology: number of included patients, median tumor size, disease stage (III or IV), and median population age. The approach used for electrode positioning (surgical [SUR] or percutaneous [PC]), the prospective, retrospective, controlled design of the study, and the percentage of chemotherapy pretreated patients.
- Outcomes: Studies had to provide at least one of the following “survival outcome” to be included: median overall survival (OS) from diagnosis or from IRE or progression-free survival (PFS) from IRE. Survival was expressed in months with interquartile range (IQR). If IQR were not provided in the publication, manual analysis of the Kaplan-Meier curves allowed calculation.
- Safety: Median hospital stay duration was expressed in days. The number of patients who underwent an adverse event (AE) was noted for each study in association with the number of severe adverse events (SAEs) defined as Clavien-Dindo ≥3/5 (9). The main types of AEs described were also collected. In several studies, the number of patients experiencing AEs was not available (NA). We estimated that it was at least equal to the most frequently reported AEs (e.g., if 50 patients experienced fever and 45 pleural effusions, the number of patients with AEs was at least 50).
Statistical analysis
For ECT and electroimmunotherapy, the scarcity of the available literature did not allow us to provide pooled statistical analysis. For IRE, statistical analysis was performed with the use of R Software (version 4.4.2). Since several data were NA, calculations were realized on the subpopulation where the analyzed data were present. For each analysis, we provided the size of the subpopulation and the percentage of the entire population it represents N (%).
We calculated weighted means for age, tumor size, hospital stays, and AEs/SAEs rates. The association between the AEs/SAEs percentages and the SUR or PC approaches was calculated with the Fischer tests.
For survival outcomes (OS and PFS), we calculated a weighted median in addition to the weighted mean to take the wide range of variables dispersion into consideration. We used the IQR to provide a boxplot of the survival outcomes for each study.
RESULTS
Literature screening
The results of the systematic review are displayed in Figure 2. From the 415 studies identified through database research after duplicate removal, 60 were included in our review. Studies were excluded because they were either preclinical IRE studies (n = 73), because they were reviews or articles bringing no additional data (generalities about EP, letters, comments, study protocols, etc.) (n = 140), or because they were case reports (n = 24). Finally, some studies were excluded because being out of the topic (n = 118). Fifteen studies treated from ECT, 38 from IRE, and 7 form immune-electroporation.
PRISMA flowchart of the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Electrochemotherapy
ECT relies on the ability of cells to open up membrane nanopores under the effect of PEFs. This allows chemical agents to which the cell is normally impervious to penetrate it during a few minutes (10). ECT application to control subcutaneous skin metastasis progression has been widely described in the European Standard Operating Procedures of Electrochemotherapy (ESOPE) protocol (5), which is worth being cited because most of the following works use the same electrical parameters (8 × 100 μs pulses at 1,000 V/cm—at a 5 kHz frequency) and cytotoxic agent, namely bleomycin. Although clinical literature is scarce regarding ECT for PDAC, several studies have reported potential benefits of ECT at several scales in preclinical PDAC models. Table 1 summarizes these different trials, their experimental settings, and their outcomes.
In vitro studies highlight the increased efficiency of bleomycin and cisplatin in PDAC cells, with bleomycin being the strongest potentiator. The ESOPE protocol was used in most study protocols. Innovative combination such as sunitinib could improve the cytotoxicity of bleomycin.
In vivo studies show that ECT seems to be safe when performed on large animals such as pigs. Its nonthermal effects reduce the number of complications compared with thermal techniques such as radiofrequency ablation (RFA) (22). Some data on electrical settings were NA. ECT preserves collagen membranes, leaving blood vessels and biliary/pancreatic ducts relatively undamaged (23). This has also been confirmed on humans with a 2017 study describing treatment of vascular portal metastasis of liver cancers with bleomycin ECT. In this study (6 patients), the thrombus seemed efficiently treated and no major side effect was noted (24). Preclinical results of ECT's efficiency have been evaluated on murine models (25). The results are promising with a potentiation of bleomycin and carboplatin.
Human studies
Several human phase I–II studies have been published, a randomized phase IIB study is actually ongoing, but to date, no preliminary results have been published (26). The main results of clinical studies regarding ECT for the treatment of PDAC are detailed in Table 2. Preliminary results are encouraging with no SAEs and some pain improvement. Available data are however insufficient to assess its effectiveness.
Irreversible electroporation
IRE induces cellular death by prolonged nanopore opening in cellular membranes leading to cellular implosion. It offers the advantage of being (almost) nonthermal and to preserve collagen matrix (and thus vascular and biliary structures) compared with other ablative techniques. It is widely used in prostate cancer (Nanoknife).
The results of our systematic review describing its uses for human PDAC treatment are summarized in Table 3.
In contrast to ECT, no standard IRE protocol is available. However, a recent expert consensus (69) proposed the following settings: interelectrode distance of 10–20 mm and 90 pulses of 1,500 V/cm with a 90-μs pulse length.
We conducted a statistical analysis of the data collected from the systematic review on IRE (Table 4).
Population: We included 38 studies with a total amount of 2,245 patients receiving IRE mostly for LAPC (>95%). The median age was 61.7 (n = 1,936). The median tumor size was 3.6 cm. Most of the patients received IRE for tumoral ablation in unresectable tumors and 9% for margin enhancement during surgery.
Methodology.
Only 2 studies including 4.3% of the population were randomized. Fifty-three percent of the population came from prospective studies and 47% from retrospective ones. Electrode positioning for IRE was SUR in 41% of the patients and PC in 59%.
Safety.
Thirty-six percent of patients experienced AEs, 47% of which severe. AEs occurred more frequently in the PC group (38%) compared with the SUR group (35%), odds ratio 0.82, confidence interval 0.66–1.01, P = 0.07. However, there were significantly more SAEs in the SUR group, odds ratio 1.30, confidence interval 1.01–1.7, P = 0.04. The most commonly described AEs were pain (30.6% of the AEs), ascites (11.8%), pancreatitis (10.2%), biliary or pancreatic fistulas (9.5%), infections (11.8%), delayed gastric emptying (6.2%), and hemorrhages (7.2). Twenty-five patients died as a direct consequence of IRE (1.3%). The median hospital stay was 6 days.
Survival.
The estimated weighted median of OS after IRE was 17.2 months, the overall PFS was 12.2 months, and the overall OS from diagnosis was 25.6 months. Figure 3 offers a graphic representation of survival outcomes.
Graphic representation of survival outcomes after IRE for PDAC. IQR, interquartile range; IRE, irreversible electroporation; OS, overall survival; PDAC, pancreatic ductal adenocarcinoma; PFS, progression-free survival.
Electroporation and immunotherapy
Table 5 summarizes the different trials describing a potential benefit of electroporation (reversible or irreversible) on immunotherapy (70). Immunotherapy seemed to improve the survival of patients treated with IRE. To date, no randomized trial has compared IRE + immunotherapy with the standard of care.
DISCUSSION
Electrochemotherapy
ECT has shown promising results in in vitro and murine models of PDAC, although we have access to a limited number of studies. The most commonly used drug was bleomycin with an electrical protocol following the ESOPE consensus.
Whereas several works have proven the benefits of ECT in oncology, few studies in patients with PDAC are available to date. One randomized trial comparing ECT with bleomycin with standard of care is currently ongoing with no published results to date.
Further preclinical studies on innovative translational models such as tumor slices or murine immunocompetent models could help investigate the value of combining ECT and immunotherapy.
One major limitation for the human applications of ECT and IRE is the difficulty of the pancreatic access (needing to be radiological or even surgical). This difficulty increases the morbidity of procedures and limits its recurrences to 1 single application. Minimally invasive approaches, such as endoscopically guided devices, could provide safer and repeatable means to perform pancreatic ECT.
We can conclude from the available data that the outcomes of ECT are promising on pain management, but further studies are needed to explore the OS or PFS benefits. ECT seems safe compared with the AEs described in the IRE, or other ablative procedures but larger studies have to be performed to confirm this trend.
Irreversible electroporation
Benefits of IRE.
We present, to our knowledge, the largest literature review regarding IRE in PDAC (73–75). Most of the patients had LAPC. The OS from IRE was 18.2 months. Among the studies described, few compared IRE with standard of care and none with a proper randomized design. The only available randomized studies compared IRE with radiotherapy (with no significant difference) or with IRE with immunotherapy, showing in that case some benefit of the adjunction of immunotherapy.
When comparing the calculated OS after IRE with the reported survival of LAPC with folfirinox (17.1 months) (76) or with OS from patients who do not undergo surgical resection after chemotherapy (16.3 months) (77), IRE does not seem to extend survival significantly. This trend is confirmed by a recent meta-analysis highlighting the absence of significant survival benefits of IRE (75). A randomized trial is actually ongoing (PMC11662571), but the lack of significant benefit of IRE associated with a high AE rate pleads against its use in clinical practice.
Side effects.
About one-third of the treated population experimented side effects with 47% of those being classified as severe, including intra-abdominal hemorrhage, fistulas, or pancreatitis and with an overall IRE-related mortality exceeding 1%. These results are consistent with other systematic reviews (78). There was no significant association between AEs and the SUR or PC approach; however, the SUR approach was significantly associated with a higher number of SAEs. It is noteworthy that the procedure is contraindicated if a self-expandable biliary stent is present in the electric field, which is a particularly common occurrence in PDAC management (79). No mentions were found regarding the risks of RE if a biliary stent is positioned, but the few available clinical studies included patients with biliary stents and no major AE occurred suggesting that the inference of the metallic stents might be related to the higher current delivered during IRE. This limitation should however be taken into consideration, should RE and ECT be used in common practice.
IRE compared with other ablative techniques.
In contrast to ECT and electroimmunotherapy, IRE is an ablative technique and can be compared with other minimally invasive procedures such as RFA, microwave ablation (80), brachytherapy (81), or cryotherapy (82,83). If the data regarding the latest remain scarce, several studies describe the pancreatic uses of RFA which be performed under endoscopic-ultrasound guidance. For PDAC treatment (84), RFA is followed by approximately 13% of AEs with some benefits on tumor growth or pain management but no demonstrated survival benefit (85,86). RFA however progressively integrates the common practice with its applications for small (<2 cm) pancreatic neuroendocrine tumors such as insulinomas (87).
Limitations and bias.
The conclusions provided by this literature review on IRE are subject to limitations.
Population.
Patients recruited in the studies included for this IRE review were hyperselected. They were also relatively young compared with the literature (88) but had a tumor size comparable with other cohorts of LAPC (77). Our review is also subject to publication bias that could lead to overlook negative survival and/or morbidity results.
Methodology.
Many studies are retrospective or stemming from prospectively maintained databases. Some teams published successive cohorts but with overlapping inclusion times which means that some patient's data might be analyzed twice.
Data analysis.
Several missing data were reported which leads to bias. In several studies, the number of patients experiencing AEs was not described. We estimated that it was at least equal to the most described AEs. This allowed to include more studies in the AEs analysis but can underestimate the total amount of AEs. For SAEs however, calculations were made only on available data because it was not possible to infer if not specified. Finally, the available data did not allow to perform multivariate analysis. Our results remain however consistent with other literature reviews (75).
Immunotherapy and electroporation
Immunotherapy has significantly improved therapeutic outcomes in some cancers (skin, lung, and stomach), but efficacy results have been elusive in PDAC so far. Among others, one reason could be the dense and immunosuppressive TME surrounding PDACs limiting cytotoxic lymphocyte trafficking. The abscopal (literally, “away from target”) effect describes the action on metastasis of the treatment of a local lesion with an ablative therapy which is supposed to rely on the release of tumoral antigens after local ablation, enhancing global antitumoral immunity (89–91). Some preclinical works on IRE highlight similar effects with an increase of regulatory T cells and PD-1^+^ T cells after IRE on small groups of human patients (92).
A synergy between ECT and immunotherapy has been described for melanoma since 2003 (93). Studies have demonstrated a higher efficiency in melanoma of ipilimumab (antiCTLA-4) + ECT (94) and pembrolizumab (antiPD1) + ECT (95) vs immunotherapy alone. Few studies have described the association of immunotherapy and electroporation, but to date, no study has focused on ECT + immunotherapy combination. Some IRE + immunotherapy studies were included in the analysis and seemed to provide a better OS compared with IRE alone. The adjunction of immunotherapy was not associated with significantly higher AEs/SAEs rates in these studies. These results are promising and deserve further investigation because other ablative techniques such as radiotherapy are not associated with such a strong potentiation (96).
Electroporation for the treatment of pancreatic cancer has been studied for the past 20 years. IRE to treat locally advanced PDAC does not seem efficient enough, regarding its high rate of AEs to be used in clinical practice. The benefits of combining IRE with immunotherapy are promising but remain experimental and deserve prospective controlled studies. ECT for PDAC is still in its infancy, but its low associated morbidity and potentialities for overcoming the TME barrier and stimulating the immune response bear some promises.
CONFLICTS OF INTEREST
Guarantor of the article: Gabriel Marcellier.
Specific author contributions: G.M.: data collection, writing, reviewing, and statistical analysis. T.L., P.R., and M.R.: reviewing. F.P.: reviewing, data collection, and writing.
Financial support: None to report.
Potential competing interests: None to report.
Availability of data: The complete data collected are included in the study tables.
Acknowledegments: We could like to express our gratitude to the teams involved in the PACTE projetct (Pancreatic Cancer Treatment using EUS-Guided Electroporation), as well as to the members of our research consortium (APHP, Ampère, LGEF, ILM) for their invaluable collaboration and support throughout this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sherman MH Beatty GL. Tumor microenvironment in pancreatic cancer pathogenesis and therapeutic resistance. Annu Rev Pathol 2023;18:123–48.36130070 10.1146/annurev-pathmechdis-031621-024600 PMC 9877114 · doi ↗ · pubmed ↗
- 2Park W Chawla A O'Reilly EM. Pancreatic cancer: A review. JAMA 2021;326(9):851–62.34547082 10.1001/jama.2021.13027 PMC 9363152 · doi ↗ · pubmed ↗
- 3Klein AP. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat Rev Gastroenterol Hepatol 2021;18(7):493–502.34002083 10.1038/s 41575-021-00457-x PMC 9265847 · doi ↗ · pubmed ↗
- 4Geboers B Scheffer HJ Graybill PM . High-voltage electrical pulses in oncology: Irreversible electroporation, electrochemotherapy, gene electrotransfer, electrofusion, and electroimmunotherapy. Radiology 2020;295(2):254–72.32208094 10.1148/radiol.2020192190 · doi ↗ · pubmed ↗
- 5Marty M Sersa G Garbay JR . Electrochemotherapy: An easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur J Cancer Suppl 2006;4(11):3–13.
- 6MiklavčičD Mali B Kos B . Electrochemotherapy: From the drawing board into medical practice. Biomed Eng Online 2014;13(1):29.24621079 10.1186/1475-925X-13-29PMC 3995705 · doi ↗ · pubmed ↗
- 7Narayanan JSS Ray P Hayashi T . Irreversible electroporation combined with checkpoint blockade and TLR 7 stimulation induces antitumor immunity in a murine pancreatic cancer model. Cancer Immunol Res 2019;7(10):1714–26.31409607 10.1158/2326-6066.CIR-19-0101 PMC 6774877 · doi ↗ · pubmed ↗
- 8Page MJ Mc Kenzie JE Bossuyt PM . The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021;372:71.10.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗