Retrograde intramedullary nailing for femoral shaft fracture with ipsilateral dynamic hip screw fixation for femur neck fracture; dual fixation. Case study
Said Osman Dahir, Abdirahman Omer Ali, Mohamoud Hashi Abdi, Ridwan Mohamed Farah, Hodo Abdi Abdillahi, Hassan Elmi Moumin

TL;DR
This case study presents a successful treatment for a rare combination of femoral shaft and neck fractures using dual fixation techniques.
Contribution
The paper introduces dual fixation as a viable treatment option for ipsilateral femoral shaft and neck fractures.
Findings
Dual fixation with retrograde nailing and DHS provided stable fixation in a non-displaced femoral neck fracture.
The technique minimized soft tissue disruption and allowed for early mobilization.
The case highlights the potential of this approach for managing complex femoral fractures.
Abstract
Ipsilateral femoral neck and shaft fractures are rare, high-energy injuries posing diagnostic and management challenges. Optimal treatment strategies remain debated. This case study presents a successful approach using dual fixation with retrograde intramedullary nailing and dynamic hip screw (DHS) fixation. A 38-year-old male driver presented following a motor vehicle accident with right thigh and hip pain, swelling, and deformity. Radiographic evaluation revealed a transverse femoral shaft fracture combined with an ipsilateral, non-displaced transcervical femoral neck fracture. Dual fixation with retrograde femoral nailing for the shaft and DHS for the neck offers a stable construct while minimizing soft tissue disruption and potentially facilitating early weight-bearing. While open reduction and internal fixation can lead to complications, our chosen technique aimed to avoid them.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
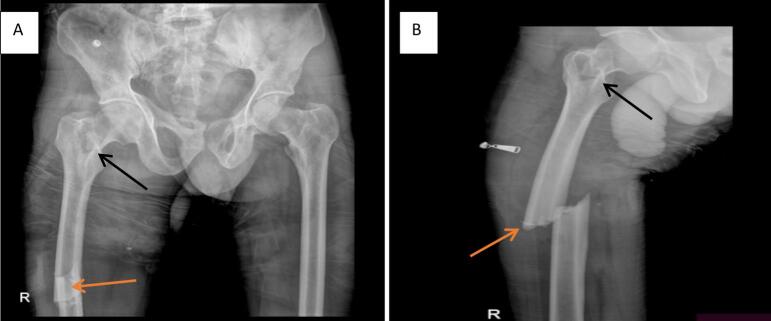 Figure 1
Figure 1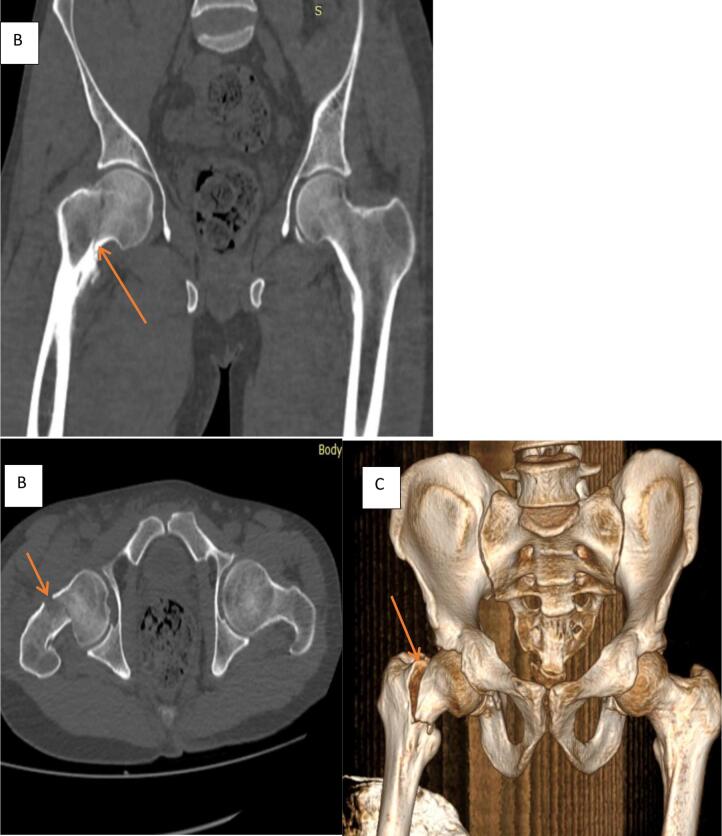 Figure 2
Figure 2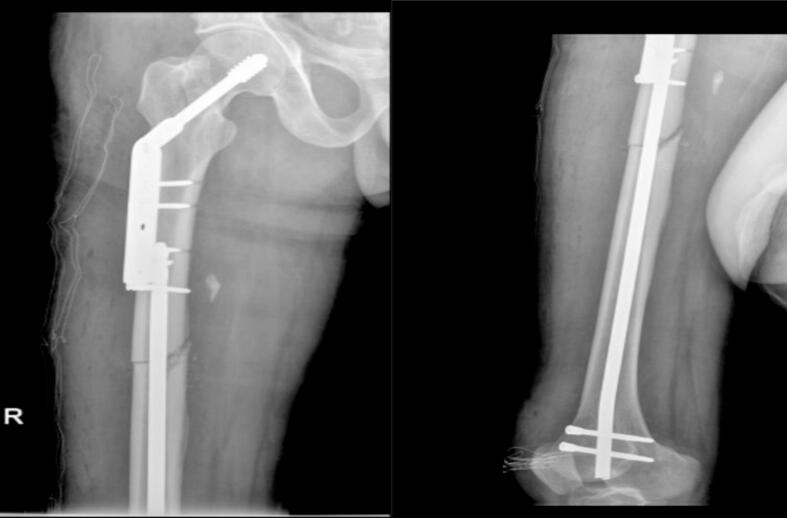 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Hip and Femur Fractures · Orthopaedic implants and arthroplasty
Introduction
1
Ipsilateral femoral neck and shaft fractures are relatively rare yet present significant clinical difficulties, accounting for approximately 2.5–9 % of all femoral fractures. This distinct fracture variant was documented for the first time in 1953 [1,2]. The concomitant fractures of the femoral neck and shaft typically arise from high-energy traumas, such as motor vehicle collisions (MVC) and falls from significant elevations. The fracture manifests when the hip experiences axial loading concurrent with leg abduction [3,4]. Affected individuals are predominantly young and frequently present with multiple concomitant injuries [5]. The identification of the femoral neck fracture is often postponed in 19–31 % of patients [6]. The management of ipsilateral femoral neck and shaft fractures presents considerable complexity, and a multitude of protocols exist for their treatment. The potential therapeutic approaches include: (1) antegrade femoral nailing of the shaft, supplemented by cancellous screws located anterior to the nail for the stabilization of the neck [6]; (2) reconstruction-type intramedullary nailing [1,7]; (3) various combinations of plate constructs [which may involve a dynamic hip screw (DHS) paired with a long side plate configuration, a hip screw accompanied by a short side plate for the neck, and a separate plate for the shaft, or the utilization of cancellous screws for the femoral neck alongside a plate for the shaft] [8], (4) retrograde intramedullary nailing of the shaft combined with screw fixation of the neck [8]. The three predominant concerns associated with these fractures pertain to the optimal timing of surgical intervention, the sequence of fracture stabilization, and the selection of the most effective implant to employ [8]. This report is written in line with the SCARE 2025 guideline [9].
Case presentation
2
A 38-year-old male driver presented following a motor vehicle accident with right thigh and hip pain, swelling, and deformity. The patient has no significant past medical or surgical history and no relevant family history of orthopedic or significant medical conditions. He reported no current medications. Radiographic evaluation revealed a transverse femoral shaft fracture combined with an ipsilateral, non-displaced transcervical femoral neck fracture.
Examination
3
On initial examination, the patient was alert but appeared to be in significant pain. His vital signs were stable. Musculoskeletal examination revealed significant swelling, deformity, and shortening of the right thigh. Distal neurovascular examination of the right lower extremity was intact. No open wounds were present.
Investigations
4
Following Advanced Trauma Life Support (ATLS) protocols [4], initial resuscitation and analgesia were administered. A radiographic evaluation was performed. A plain radiograph of the right femur revealed a transverse fracture of the femoral shaft (Fig. 1). Subsequent computed tomography (CT) scan of the pelvis revealed an ipsilateral, non-displaced transcervical fracture of the femoral neck (Fig. 2).Fig. 1AP (A) and Lateral (B) X-ray views demonstrating a complete transverse femoral shaft fracture with shortening and complete displacement (orange arrows). A lucency consistent with a non-displaced transcervical femoral neck fracture is also visible (black arrows).Fig. 1. Fig. 2Pelvic CT Scan coronal and axial 3D rendering image demonstrating non-displaced trans cervical right femoral neck fracture orange arrows in A, B and C.Fig. 2
Diagnosis
5
Based on the clinical and radiographic findings, the patient was diagnosed with a right femoral shaft transverse fracture with an ipsilateral femoral neck transcervical non-displaced fracture.
Treatment
6
Following the diagnosis, the patient was admitted to the orthopedic ward for surgical management. The surgical plan involved dual fixation: retrograde femoral nailing for the femoral shaft fracture and dynamic hip screw (DHS) fixation for the femoral neck fracture.
Surgical technique
7
The patient was placed supine on an operating table. A retrograde intramedullary nail was inserted through the distal femur intercondylar notch on the medial side of the lateral condyle as the entry point through a lateral knee arthrotomy. The fracture was reduced and stabilized with an intramedullary SIGN nail with interlocking distal and proximal screws. Fluoroscopic imaging was utilized throughout the procedure to confirm fracture reduction and implant placement (Fig. 3).Fig. 3. Retrograde intramedullary nail and the femoral neck fracture was reduced anatomically and fixed with a dynamic hip screw (DHS) system.Fig. 3
Postoperative course
8
The patient tolerated the procedure well and was transferred to the post-anesthesia care unit in stable condition. Postoperative pain management was initiated with a multimodal analgesic regimen. Thromboprophylaxis with low-molecular-weight heparin was administered to prevent deep vein thrombosis (DVT) [10]. Six weeks of non-weight-bearing on the right lower extremity were encouraged. A structured physiotherapy and rehabilitation program was initiated to improve range of motion, muscle strength, and functional recovery. The patient was closely monitored for potential complications, including avascular necrosis (AVN) of the femoral head, nonunion, malunion, infection, and hardware failure. Serial radiographs were obtained to assess fracture healing.
Discussion
9
In this case study, we successfully treated a 38-year-old male with an ipsilateral femoral neck and shaft fracture using a dual fixation approach: retrograde intramedullary nailing for the femoral shaft and dynamic hip screw (DHS) fixation for the non-displaced transcervical femoral neck fracture. This technique provided a stable construct, facilitated early mobilization, and avoided complications typically associated with more invasive open reduction methods, leading to a favorable early clinical outcome.
Ipsilateral femoral shaft and neck fractures constitute rare injuries, primarily resulting from high-energy trauma [11,12]. The mechanism of injury typically involves a combination of axial loading, bending, and rotational forces [[12], [13], [14]]. Diagnosing these fractures poses a significant challenge, particularly in scenarios where one fracture obscures the other. Thus, maintaining a heightened index of suspicion and conducting a thorough radiographic assessment, which should encompass both conventional radiographs and computed tomography scans, is imperative to prevent overlooked injuries [2,7,8,17].
The management of ipsilateral femoral shaft and neck fractures is notably intricate [18]. The treatment of these fractures necessitates a nuanced approach that considers multiple variables, including the fracture configuration, the age of the patient, physiological condition, and the experience level of the surgeon [8]. Numerous fixation methodologies have been documented, such as open reduction and internal fixation (ORIF) utilizing plates and screws, cephalomedullary nailing, and dual fixation [[17], [18], [19]]. Open reduction accompanied by plating for femoral shaft fractures has been associated with a heightened incidence of complications such as infection and nonunion [20]. In the present case, we opted to implement dual fixation utilizing retrograde femoral nailing for the shaft fracture in conjunction with dynamic hip screw (DHS) fixation for the neck fracture. Retrograde nailing provides several benefits, including minimal disruption of soft tissues, a decreased likelihood of nonunion, and the facilitation of early weight-bearing [21]. DHS fixation is a well-established modality for addressing femoral neck fractures, ensuring stable fixation while permitting controlled impaction at the fracture site [12,15,22]. The non-displaced character of the femoral neck fracture rendered it suitable for DHS fixation. Potential complications linked with these fractures encompass avascular necrosis (AVN) of the femoral head, nonunion, malunion, infection, hardware failure, and thromboembolic phenomena [17,18,27]. Vigilant observation and strict adherence to established protocols for thromboprophylaxis and infection prevention are vital to mitigate these risks. Extended follow-up is critical to evaluate the healing of the fracture, functional outcomes, and the emergence of any late complications.
Conclusion
10
The management of ipsilateral femoral neck and shaft fractures remains challenging. This case study supports the use of dual fixation with retrograde intramedullary nailing and dynamic hip screw fixation as a potential solution. While our results are encouraging, future research should focus on comparing this technique to other methods, identifying ideal patient selection criteria, and defining long-term outcomes to establish evidence-based guidelines for the optimal treatment of these rare and complex fractures.
Author contribution
Dr. Said Osman Dahir, Dr. Abdirahman Omer Ali, Dr. Ridwan Mohamed Farah and Hassan Elmi Moumin contributed in taking history and providing care to the patient throughout his hospital stay. Additionally, Dr Abdirahman Omer Ali, Hassan Elmi Moumin and Dr. Said Osman Dahira contributed to the development of the manuscript. Dr. Mohamoud Hashi Abdi is the radiologist.
Consent for publication statement
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
The study protocol, case investigation, and consent form were thoroughly examined by the institutional review board of the College of Health Sciences at Amoud University. They granted approval for the study, along with the Ministry of Health and Borama Regional Hospital in Awdal Region, Somaliland (BRHH-220/2024). Prior to participation, written informed consent was obtained from every individual involved.
Guarantor
Dr.Hassan Elmi Moumin, on behalf of all authors, accept full responsibility for the work
Research registration number
Number Not applicable.
Funding
The study did not receive funding.
Conflict of interest statement
The authors report no declarations of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jain P.Maini L.Mishra P.Upadhyay A.Agarwal A.Cephalomedullary interlocked nail for ipsilateral hip and femoral shaft fractures Injury 35102004103110381535167210.1016/j.injury.2003.09.039 · doi ↗ · pubmed ↗
- 2Singh R.Rohilla R.Magu N.K.Siwach R.Kadian V.Sangwan S.S.Ipsilateral femoral neck and shaft fractures: a retrospective analysis of two treatment methods J. Orthop. Traumatol.93200814114710.1007/s 10195-008-0025-319384610 PMC 2656981 · doi ↗ · pubmed ↗
- 3Kazley J.Bagchi K.Femoral Neck Fractures 201930726032 · pubmed ↗
- 4Denisiuk M.Afsari A.Femoral Shaft Fractures 202032310517 · pubmed ↗
- 5Watson J.T.Moed B.R.Ipsilateral femoral neck and shaft fractures: complications and their treatment Clin. Orthop. Relat. Res. (1976-2007)3992002788610.1097/00003086-200206000-0001112011697 · doi ↗ · pubmed ↗
- 6Wolinsky P.R.Johnson K.D.Ipsilateral femoral neck and shaft fractures Clin. Orthop. Relat. Res. (1976-2007)318199581907671535 · pubmed ↗
- 7Shetty M.S.Kumar M.A.Ireshanavar S.S.Sudhakar D.Ipsilateral hip and femoral shaft fractures treated with intramedullary nails Int. Orthop.31200777811674173310.1007/s 00264-006-0143-6PMC 2267537 · doi ↗ · pubmed ↗
- 8Hung S.-H.Surgical treatment for ipsilateral fractures of the hip and femoral shaft Injury 35220041651691473647510.1016/s 0020-1383(03)00278-x · doi ↗ · pubmed ↗