Assessment of Donor‐Specific Human Leukocyte Antigen Antibodies Following Pediatric Liver Transplantation: Predictors, Protectors, and Clinical Relevance
Evelien Kanaan, Sinja Ohlsson, Simone Kathemann, Benas Prusinskas, Sofia Tsaka, Falko M. Heinemann, Andreas Heinold, Maren Schulze, Lars Pape, Elke Lainka

TL;DR
This study examines donor-specific antibodies in children after liver transplants, finding they are common and linked to worse outcomes, but overall patient survival remains high.
Contribution
The study identifies predictors and protectors of donor-specific HLA antibodies in pediatric liver transplant recipients and their clinical relevance.
Findings
Donor-specific antibodies were present in 39% of patients and linked to antibody-mediated rejection in 13%.
Graft survival was significantly worse in patients with donor-specific antibodies.
Living donation and shorter cold ischemia time were protective against donor-specific antibodies.
Abstract
Following pediatric liver transplantation (pLT), the significance and management of donor‐specific antibodies (DSA) against human leukocyte antigen (HLA) remain undefined. The aim of this single‐center study was to investigate the occurrence of DSA, their clinical impact on predictors for and protectors against DSA. We compared anti‐HLA DSA (cutoff for mean fluorescence intensity (MFI) ≥ 1000), clinical and laboratory results and outcome in a routine (RG, n = 142, standard DSA testing) and a hepatopathy group (HG, n = 19, DSA testing following indeterminate hepatopathy) in 161 pLT patients, treated 2000–2021, retrospectively. 40% of RG and 32% of HG patients were DSA+ (39% of all patients, of which 13% with antibody‐mediated rejection [AMR]). Most frequent DSA subtypes were HLA‐DQ3, ‐DQ1, ‐DQ2 in RG and HLA‐DQ2, ‐DR15 in HG. MFI was higher for anti‐HLA II DSA (15 257 DSA+ vs. 5500…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
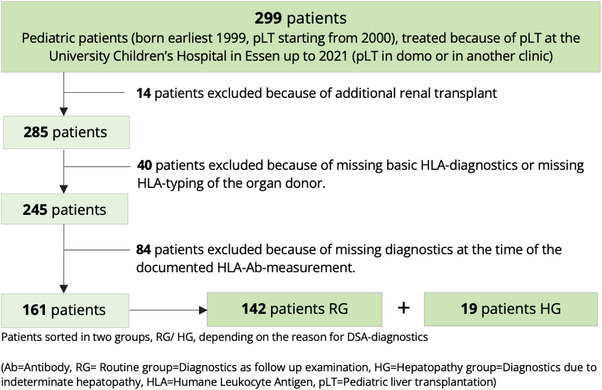 FIGURE 1
FIGURE 1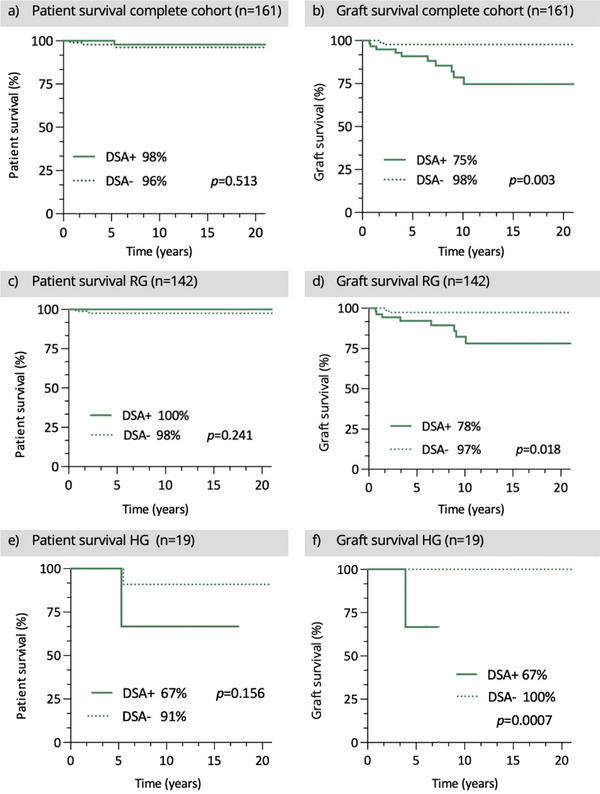 FIGURE 2
FIGURE 2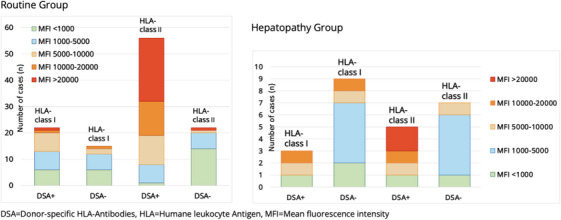 FIGURE 3
FIGURE 3| Routine group | Hepatopathy group | Complete cohort | |
|---|---|---|---|
| Number of patients ( | 142 | 19 | 161 |
| Sex |
73 male (51%) 69 female (49%) |
9 male (47%) 10 female (53%) |
82 male (51%) 79 female (49%) |
|
| |||
| Age at first pLT (months) |
42.4 ± 55.7 Median 13 Range 3–204 |
54.8 ± 71.65 Median 14 Range 5–205 |
43.9 ± 57.7 Median 12 Range 3–205 |
| Mean height (cm) |
86.3 ± 32.1 Median 70.5 Range 49–183 |
94.9 ± 39.7 Median 76.5 Range 58–173 |
87.3 ± 33.1 Median 71 Range 49–183 |
| Mean weight (kg) |
15 ± 17.8 Median 8 Range 4–119 |
21.2 ± 25.1 Median 10.2 Range 4.5–86 |
15.9 ± 18.7 Median 8 Range 4.5—119 |
| Body surface area (m2) |
0.62 ± 0.48 Median 0.4 Range 0.24–3.4 |
0.7 ± 0.56 Median 0.49 Range 0.27–1.99 |
0.63 ± 0.49 Median 0.4 Range 0.24–3.4 |
| Death following pLT ( | 2/142 (1%) | 2/19 (11%) | 4/161 (3%) |
| Cold ischemia time <8 h ( | 77/129 (60%) | 11/17 (65%) | 88/146 (60%) |
| Warm ischemia time <45 min ( | 93/126 (74%) | 15/18 (83%) | 108/144 (75%) |
| AB0‐BG‐ | 6/142 (4.2%) | 4 /19 (21.1%) | 10/161 (6.2%) |
| Full organ ( | 53/141 (38%) | 8 /19 (42%) | 61/160 (38%) |
| Deceased donor organ ( | 93/141 (66%) | 12/19 (63%) | 105/160 (66%) |
| Re–pLT ( | 15/142 (11%) | 2 /19 (11%) | 17/161 (11%) |
|
| |||
| Time since pLT (months) |
64.7 ± 61.5 Median 36 Range 2–205 |
47 ± 55.6 Median 24 Range 0–183 |
63 ± 61 Median 35 Range 0–205 |
| Hepatopathy at the time ( | 22/142 (16%) | 19/19 (100%) | 4/142 (28%) |
| Hepatopathy at any time, up to 2021 ( | 79/140 (56%) | 19/19 (100%) | 95/159 (60%) |
| Binding HLA Ab ( | 84/142 (59%) | 17/19 (90%) | 101/161 (63%) |
| HLA‐class I Ab (MFI >1000, | 25/142 (18%) | 10/19 (53%) | 35/161 (22%) |
| HLA‐class II Ab (MFI >1000, | 64/142 (45%) | 10/19 (53%) | 74/161 (46%) |
| DSA+ in this examination ( | 57/142 (40%) | 6/19 (32%) | 63/161 (39%) |
| DSA+ at any time, up to 2021 ( | 67/142 (47%) | 8/19 (42%) | 75/161 (47%) |
| GGT (U/l) |
31.6 ± 64.9 Median 15 Range 4–498 |
262.1 ± 247.3 Median 212 Range 7–866 |
58.8 ± 127.1 Median 16 Range 4–866 |
| GOT (U/l) |
39.6 ± 40.3 Median 31 Range 8–393 |
163.2 ± 166.3 Median 108 Range 35–663 |
54.2 ± 78.4 Median 33 Range 8–663 |
| GPT (U/l) |
35 ± 34.2 Median 25 Range 7–215 |
227.8 ± 253.8 Median 132 Range 24–1049 |
57.8 ± 110.3 Median 27 Range 7–1049 |
| Total bilirubin (mg/dL) |
0.8 ± 2.2 Median 0.5 Range 0–25.1 |
4 ± 7.4 Median 0.6 Range 0.2–26.2 |
1.2 ± 3.4 Median 0.5 Range 0–26.2 |
| Direct bilirubin (mg/dL) |
0.4 ± 1.6 Median 0.2 Range 0–18.6 |
3.3 ± 6.4 Median 0.3 Range 0.1–21.6 |
0.7 ± 2.8 Median 0.2 Range 0–21.6 |
| Quick value (%) |
85.2 ± 13.5 Median 86 Range 51–119 |
84.3 ± 19.6 Median 83 Range 38–112 |
85.1 ± 14.3 Median 86 Range 38–119 |
| Albumin (g/dL) |
4.4 ± 0.4 Median 4.5 Range 2.3‐5.4 |
4 ± 0.6 Median 4.1 Range 2.1–4.7 |
4.4 ± 0.4 Median 4.4 Range 2.1–5.4 |
| Creatinine (µmol/L) |
51.8 ± 20.5 Median 51 Range 17–136 |
54.9 ± 43.1 Median 49.5 Range 17–217 |
52.2 ± 23.9 Median 50.5 Range 17–217 |
| Immunoglobulin G (g/L) |
10 ± 3.6 Median 9.9 Range 1.4–19.8 |
14 ± 7.3 Median 12.4 Range 5.7–30.2 |
10.3 ± 4.2 Median 10 Range 1.4–30.2 |
|
| |||
| Valid liver elastography result ( | 70/142 (49%) | 9/19 (47%) | 79/161 (49%) |
| Pathologic elastograpy result (kPa) |
>5 = 36/70 (51%) >7.3 = 10/70 (14%) >9.6 = 3/70 (4%) Mean 5.7 ± 2.3 Median 5 Range 0.5–17.6 |
>5 = 8/9 (89%) >7.3 = 4/9 (44%) >9.6 = 2/9 (22%) Mean 9.1 ± 7.7 Median 6.6 Range 0.6–27.4 |
>5 = 44/79 (56%) >7.3 = 14/79 (18%) >9.6 = 5/79 (6%) Mean 6.1 ± 3.5 Median 5.2 Range 0.5–27.4 |
| Liver biopsy performed ( | 35/142 (25%) | 19/19 (100%) | 54/161 (34%) |
|
Fibrosis detected (F ≥ 1) ( Fibrosis scoring |
22/35 (63%) Mean 1.9 ± 0.8 Median 2 Range 1‐4 |
18/19 (95%) Mean 1.9 ± 1.1 Median 1.5 Range 1–4 |
40/54 (74%) Mean 1.9 ± 0.9 Median 1.8 Range 1‐4 |
| Fatty degeneration ( | 5/35 (14%) | 2/19 (11%) | 7/54 (13%) |
| Rejection ( | 3/35 (9%) | 5/19 (27%) | 5/54 (9%) |
|
Inflammation detected (Score ≥ 1) ( Inflammation score |
16/35 (46%) Mean 2.2 ± 0.8 Median 2 Range 1–3 |
13/19 (68%) Mean 1.6 ± 0.8 Median 1 Range 1–3 |
29/54 (54%) Mean 1.9 ± 0.8 Median 2 Range 1–3 |
| ITBL | 3/35 (9%) | 4/19 (21%) | 7/54 (13%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Renal Transplantation Outcomes and Treatments · Liver Disease and Transplantation
Introduction
1
In recent years, donor‐specific antibodies (DSA) against human leukocyte antigen (HLA) after pediatric liver transplantation (pLT) has attracted increasing scientific attention. Nevertheless, the number and significance of related studies, especially concerning pediatric patients, are limited. Most studies examine adult patients, and although one meta‐analysis demonstrated a higher prevalence of DSA in pLT recipients than in adults [1], only patient populations from individual centers are analyzed and reported. The available literature underlines the need for more data, as DSA have been shown to be associated with liver graft fibrosis progression, rejection, and detrimental outcomes [2, 3].
The liver is known to be the immunologically most “tolerogenic” transplant organ. This is one reason why fewer rejections occur and smaller dosages of immunosuppressants are needed compared to other organ transplantations [4]. The liver parenchyma is protected by various immunological mechanisms, the immense capillary surface and good regenerative capacity [5]. Hence, impact of DSA on the transplant organ can be reduced, but not prevented entirely. Until recently, HLA‐compatibility and DSA were not considered relevant in pLT. Antibody‐mediated rejection (AMR) has increasingly become the object of investigation and discussion. Meanwhile, operational tolerance by complete weaning from immunosuppressants is also increasingly under discussion, as it is an aspirational goal in future patient care. Feng et al. showed that the presence of DSAs does not necessarily indicate unsuccessful operational tolerance in pLT [6].
In AMR, antibodies (Ab) of the recipient against the AB0 blood group antigens in AB0‐incompatible transplants or against the organ donor's HLA antigens (DSA) cause damage to the donor organ [7]. Ab can be performed prior to pLT, for example, through previous contact with foreign antigens via blood transfusions, or develop de novo after contact with the donor organ [8]. Endothelial cells and the arterial capillary plexus around the bile ducts appear to be particularly affected by AMR, resulting in ischemic cholangiopathies [9, 10]. It is assumed that acute AMR, especially after prior existing DSA, often progresses rapidly to T‐cell mediated rejection (TCMR) [11, 12, 13]. Chronic rejection rather leads to slowly progressive symptoms of graft dysfunction. Persistent DSA levels and poorly adjusted immunosuppression seem to play a role here [14].
Although AMR and DSA have been subject of scientific research more frequently, there are still many unanswered questions, especially around the lack of recommendations regarding practical clinical management. The intention of this study was to investigate the occurrence of DSA, to obtain more information on potential predictors for their development after pLT, as well as possible protective factors as indicators for potential measures to prevent AMR. By analyzing survival rates, our aim was to investigate the impact of DSA, as their clinical relevance in pLT is still a point of controversy.
Patients and Methods
2
Patients
2.1
This retrospective monocentric study included 161 children after pLT who were treated between 2000 and 2021. Inclusion criterion was an available HLA Ab measurement. Patients with both kidney and liver transplantation were excluded as well as patients with incomplete diagnostics (e.g., missing HLA typing of the organ donor) (Figure 1).
Patient exclusion criteria.
Two groups were formed: (1) Routine group (RG, n = 142, DSA screening performed as part of routine follow‐up after pLT), (2) Hepatopathy group (HG, n = 19, DSA diagnostics performed due to indeterminate hepatopathy). Hepatopathy was defined as transaminases elevated over twice the upper value, fibrosis ≥F2 or a definite liver disease diagnosis. Within the two patient groups (RG, HG), subgroups were formed regarding the presence of DSA (DSA+, DSA−). General patient characteristics and key information regarding the pLT (e.g. deceased donor, ischemia time) were documented as well as various clinical and laboratory results including immunosuppressive medication and liver enzymes. Additionally, sonography, liver elastography and results of the liver biopsy were collected (Table 1). These findings were documented for two points in time – 1. surrounding the date of the pLT and 2. at the time of a later HLA‐Ab measurement (e.g., at routine follow‐up 1 year after pLT). The setting of the study thus is one timepoint cross sectional. The study was approved by the ethics committee of the faculty of medicine of the University Duisburg‐Essen (18‐8231‐BO).
HLA Typing and Testing for Antibodies
2.2
Patient deoxyribonucleic acid (DNA) was isolated from peripheral blood samples. DNA was extracted using spin columns (Qiagen, Hilden, Germany) or by an automated system, using magnetic beads (Chemagen/Perkin Elmer, Baesweiler, Germany). HLA typing of the recipients and living donors was performed for the HLA‐A, B, C, DRB1 and DQA1/DQB1 loci by PCR‐SSO (polymerase chain reaction with sequence‐specific oligonucleotide probes) in single‐field resolution and a Luminex system (LABType by One Lambda/Thermo Fisher, Canoga Park, CA, USA). Deceased donors were typed according the Eurotransplant allocation procedures [15]. Patient post transplantation serum samples were tested for IgG Ab against HLA class I and II using Luminex‐technology (LABScreen‐Mixed Beads, One Lambda/Thermo Fisher, Canoga Park, CA, USA) according to the manufacturer's instructions and as described in detail previously [16, 17]. If results for HLA class I or II Ab were positive, the Luminex Single Antigen Beads LABScreen assay was used, provided by the same manufacturer, to confirm if HLA Ab were donor specific. Mean fluorescence intensity (MFI) of ≥1.000 was considered positive regarding evidence for DSA. The focus of this study was exclusively on DSA after liver transplantation. HLA antibody analyses for preformed DSA had not been performed regularly and pre‐TX antibody data was not included.
Data Collection and Statistical Analysis
2.3
All data were collected retrospectively by reviewing the patient files in electronic (CGM MEDICO, Koblenz, Germany), paper‐based documentation systems and the pLT database of the University Children's Hospital Essen. Statistical analysis was carried out using GraphPad Prism, version 9.3.1 (1994–2023 GraphPad Software, LLC) and Microsoft Excel for Mac version 16, 2021 (Microsoft Corporation, Washington, USA). Data collected from both groups were analyzed descriptively. The t‐test, Mann–Whitney U test or Chi‐square test were used for comparisons between groups. The Pearson correlation coefficient was calculated to identify possible correlations. To investigate patient and graft survival Kaplan–Meier curves were created, combined with the log‐rank test to analyze significant differences. If one patient showed DSA against multiple HLA‐specificities, the highest found MFI strength was used for calculations, not the sum or mean of all values. Significance was always assumed at a p value < 0.05.
Results
3
Patient Cohort
3.1
One hundred and sixty‐one children (51% male, 49% female) were a median of 12 months old (range 3–205 months) at pLT (Table 1). The main indication for pLT was biliary atresia 50%, followed by progressive familial intrahepatic cholestasis types I–III 11%, acute liver failure with unknown cause 7%, several diseases of the biliary tract (e.g., primary sclerosing cholangitis, choledochal cyst) 7%, metabolic diseases 5%, Alagille‐syndrome 4%, hepatoblastoma 3%, cystic fibrosis (CF) 4%, and others.
Survival
3.2
Overall graft survival was significantly higher in the DSA− than in the DSA+ subgroup, p = 0.003. Graft survival was lower when DSA+ were present (RG 78% DSA+ vs. 97% DSA−, p = 0.018, HG 67% DSA+ vs. 100% DSA−, *p *= 0.0007). Patient survival showed no significant difference, RG *p *= 0.241, HG *p *= 0.156. Patient survival of the entire cohort (n = 161) was higher for DSA+ than for DSA−, but not significantly, *p *= 0.513 (Figure 2). Four children died over time: two children from the HG (1 DSA−, 1 DSA+), two children from the RG (both DSA−).
Patient and graft survival, comparison DSA+ versus DSA−.
Routine Group (RG)
3.3
DSA Screening
3.3.1
One hundred and forty‐two patients had been tested for DSA in a routine follow‐up setting. DSA+ were found in 40%, 57 patients; 60%, 85 patients were DSA−. The most frequent DSA specificity was HLA‐DQ3, 33% [19/57], including the splits ‐DQ7, ‐DQ8, ‐DQ9. Among these, Ab against HLA‐DQ7 were the most frequent (n = 12). Next were HLA‐DQ1 (including the splits HLA‐DQ5 and ‐DQ6) 32% [18/57] and HLA‐DQ2 16% [9/57]. 98% [56/57] of all DSA+ had HLA class II Ab, only 28% [16/57] of which showed HLA class I Ab.
MFI was ≥5000 in 86% [48/56] of the cases with donor‐specific HLA class II Ab, and in 66% [37/56] MFI was ≥10 000. For donor‐specific HLA class II Ab, the mean MFI was 15 257, significantly higher than without donor specificity 5500, *p *= 0.005. For HLA class I Ab, the difference in MFI between DSA+ (mean MFI 6013) and DSA− (mean MFI 4900) was not significant.
Thirty‐two patients showed DSA+ and MFI ≥ 15 000.19% [6/32] patients suffered from hepatopathy.67% [4/6] cases were diagnosed with AMR. DSA+ and MFI < 15 000 were detected in 25 patients.16% [4/25] children suffered from hepatopathy, of which one case was an AMR (25%, [1/4]). Even though the proportion of those with AMR was higher for MFI ≥ 15 000, this difference was not significant. Conversely, 79% of DSA+ and MFI ≥ 5000 showed no hepatopathy, 81% of DSA+ and MFI ≥ 15 000 and 83% of DSA+ and MFI ≥20 000 had no clinical problems (Figure 3).
Strength of MFI for antibodies against HLA molecules depending on donor specificity.
16% [22/142] of all RG patients, 39% [22/57] of all DSA+ showed hepatopathy, the most frequent underlying diagnosis being DSA‐related AMR 23% [5/22], fibrosis 23% [5/22] and cholangitis 18% [4/22], followed by other biliary tract related problems and blood vessel complications both 9% [2/22].
Basic Characteristics
3.3.2
Patients with DSA+ were significantly older (DSA+ 52.6 ± 61.5 months vs. DSA− 35.5 ± 59.6 months, *p *= 0.004) and taller at the time of pLT (DSA+ 95.4 ± 35 cm vs. DSA− with 84.6 ± 30.8 cm, *p *= 0.03). Age and height correlated, as assumed (r = 0.933). In DSA+ patients, deceased donor liver transplants (DDLT) were significantly more common (DSA+ 80% [45/56] vs. DSA− 56% [48/85], *p *= 0.003). If cold ischemia time had been less than 8 h, DSA were significantly less frequently detected (DSA+ 49% [25/51] vs. DSA− 67% [52/78], *p *= 0.028). Re‐pLT was more common in DSA+ than in DSA− (DSA+ 19% [11/57] vs. DSA− 5% [4/85], *p *= 0.004). CF was the only underlying disease with a significantly higher proportion of affected patients among DSA+ (DSA+ 9% [5/57] vs. DSA− 1% [1/85], *p *= 0.025). The time from pLT to documented time of DSA testing was significantly higher for DSA+ (DSA+ 77 ± 61 months vs. 52 ± 56 months, *p *= 0.006).
Immunosuppressive Medication
3.3.3
The proportion of patients taking cyclosporine A (CSA) at the time of the DSA screening was significantly higher in DSA+ cases than in those with DSA− (DSA+ 19% [11/57] vs. DSA− 7% [6/85], *p *= 0.028). No significant differences were detected for the use of tacrolimus (TAC), predniso(lo)ne or mycophenolic acid (MPA).
Hepatopathy Group (HG)
3.4
DSA Diagnostics
3.4.1
DSA+ were detected in 32% [6/19] patients and DSA− in 68% [13/19]. If DSA+ were found, they were most frequently directed against HLA‐DQ2 16% [3/19], followed by HLA‐DR15 11% [2/19]. The average time between pLT and HLA Ab examination was 47 ± 55 months. The proportions of Ab against HLA class I and II did not differ significantly between DSA+ and DSA−. HLA−Ab against class II showed a significantly higher MFI with donor specificity than without (DSA+ 18 700 vs. DSA− 3567, *p *= 0.019) (Figure 3). 16% [3/19] patients suffered from hepatopathy with underlying DSA‐related AMR. The following most frequent reasons for hepatopathy were biliary tract complications 21% [4/19] (e.g., stenosis, mismatch), HLA‐unrelated rejection, Epstein Barr virus infection and autoimmune hepatitis, each 11% [2/19].
Basic Characteristics
3.4.2
Similar to the RG cohort, patients were significantly older at pLT, when DSA were detected (DSA+ 101 ± 89 months vs. DSA− 33 ± 53 months, *p *= 0.028). DSA+ were more frequent in patients after re‐transplantation (DSA+ 33% [2/6] vs. DSA− [0/13] *p *= 0.028). No other significant differences were found for basic characteristics.
Immunosuppressive Medication
3.4.3
Predniso(lo)ne was taken significantly more frequently at the time of the DSA diagnostics, if DSA+ were detected (DSA+ 100% [6/6] vs. DSA− 54% [7/13], *p *= 0.044). For MPA, similar results were found (DSA+ 100% [6/6] vs. DSA− 23% [3/13], *p *= 0.002). There was no significant difference in the use of CSA and TAC.
Discussion
4
Due to the scarcity of liver donors and the significantly worse outcomes associated with re‐transplantation, there is an unmet need to prolong graft survival by diagnosing rejections promptly and improving patient management after pLT. The literature on DSA is not only sparse, but often also controversial, as in our study.
In our cohort, DSA+ were detected in 39% [63/161] patients. This is close to the average prevalence among pediatric patients of 41% reported in a meta‐analysis from 2016 [18].
Similar to other studies, DSA+ were significantly more often specified against HLA class II antigens than against HLA class I antigens. The predominant expression of HLA I molecules in the liver may lead to increased formation of Abs against these molecules but also appears to result in increased absorption of Abs in the transplant organ. Presumably, this reduces the concentration of DSA against HLA class I in peripheral blood. Intrahepatic soluble HLA class I molecules, forming immune complexes with class I DSA, which are then eliminated by Kupffer cells, play an important role here [19, 20]. This theory is also supported by the observation that the liver appears to have a protective effect on the transplanted kidney in simultaneous liver‐kidney transplantations from the same donor, at least regarding preformed DSA. In some such cases (in adults), complete disappearance of HLA class I DSA, and even DSA against both HLA classes, has been demonstrated after transplantation [21, 22].
A significantly higher mean MFI was found for HLA class II Ab, when donor specificity was present. Patients with AMR showed MFI values between 14 000 and 28 600, clearly above the cutoff of 1000. The comparison of MFI values between DSA+ with AMR present against those in DSA+ without AMR (for RG + HG, n = 161) showed significantly higher MFI values for the group with AMR (DSA+ and AMR mean MFI 21 000 ± 5224, DSA+ without AMR mean MFI 14 584 ± 8465, *p *= 0.0427). At the same time, around 77% of DSA+ with an MFI ≥ 5000 had no hepatopathy, and 79% of DSA+ with an MFI of ≥20 000 also showed no clinical problems. Thus, these results indicate AMR being unlikely at very low MFI, and the combination of hepatopathy and DSA+ with high MFI (≥15 000) should possibly lead to considering AMR as a diagnosis. At the same time, however, high MFI values alone do not seem to be a good marker for adverse clinical issues. On the one hand, more clinical problems such as fibrosis and higher mortality are reported to be associated with higher MFI values [23, 24], whilst on the other hand, association of low MFI values (500–4000) with clinical complications such as TCMR and AMR [25, 26] have been reported, as well as a clinical course completely independent from the MFI level [27, 28].
Another relevant factor is the HLA subtype. The fact that primarily DSA+ against the HLA subtypes ‐DR and ‐DQ were detected is consistent with the results of other pediatric studies [22, 28]. Melere et al. reported an association of HLA‐DQ DSA with a higher risk of rejection [29]. This is supported by our results, as rejection episodes occurred more often in patients with HLA‐DQ DSA than in those without (DQ+ 52% [22/42] vs. DQ− 7% [1/15], *p *= 0.002). All five patients with AMR were positive for HLA‐DQ DSA in the RG cohort and 2/3 AMR patients in the HG cohort. The frequency of the HLA alleles differs between populations (and thus among the donors), so the dominance of certain subtypes might not be expected in all populations. In addition, HLA‐DQ is particularly rarely expressed in the liver, leading to less absorption of the corresponding liver antibodies, which could be the reason for the predominant detection of HLA‐DQ Ab [20].
Potential Predictors
4.1
Patient Age and Height at pLT
Within the RG, patients with DSA+ were older and taller at the time of pLT than those without DSA−. It can be assumed that the patient's age played the decisive role here, considering that immunology changes over the course of the first years of life and body measurements depend on age. Other studies described that children with DSA+ were younger than those without DSA− [29]. In alignment with our results, Goto et al. found a higher age at DSA+ [23].
Cystic Fibrosis
In our study, CF was the only transplant indication associated with significantly more cases of DSA+. Theoretically, an increased probability of alloimmunization can be suspected due to the pronounced inflammatory processes already present in these patients before transplantation. After lung transplantation, CF was postulated as a risk factor for the development of DSA and AMR [31]. The adjustment of treatment is often more complex in patients with CF due to limited gastrointestinal absorption and increased renal elimination [32, 33].
Re‐Transplantation
Our results and those reported previously have identified re‐pLT as a risk factor for the development of DSA+ (adult patients) [34]. This is most likely related to the immunological processes stimulated by repeated transplants whereby the recipient's immune system has increased contact with foreign HLA antigens.
Potential protectors
4.2
Cold Ischemia Time < 8 h
In the RG, fewer DSA+ were detected if cold ischemia time during pLT had been <8 h. Other studies found no significant difference in ischemia time when comparing DSA+ and DSA− [23, 35, 36]. It is known that ischemia time is a significant risk factor for the stimulation of immunological processes in the transplant organ. Intrahepatic sinusoidal endothelial cells are particularly sensitive to cold ischemia [37]. The ischemia period creates an overall pro‐inflammatory situation, which increases the expression of both HLA class I and HLA class II antigens on hepatic and biliary endothelial cells and hepatocytes, potentially resulting in increased development of DSA [9]. Donor dendritic cells are increasingly transported from the transplant organ to the lymph nodes of the recipient, which in turn favors a corresponding immune response [10].
Living Donation
To date, there are discrepant findings on the role of the origin of transplant (DDLT vs. living donor liver transplant [LDLT]) on DSA development. DSA+ was found to be more frequent after DDLT than after LDLT in our RG. The fact that the immunological processes surrounding transplantation and the outcome differs between living and deceased donation have already been highlighted [38]. Besides the prolonged cold ischemia time, it is assumed that brain death, which precedes most DDLT, is one of the underlying reasons for this. Both factors lead to increased inflammation in the donor organ [39, 40]. DSA+ were detected less frequently in pediatric patients after living maternal donation. In addition to the higher probability for HLA compatibility due to the close relationship, maternal microchimerism, that is, the retention of maternal cells, including immune cells, in the child's organism, has been discussed [41]. Immunological processes surrounding DDLT thus may increase the risk of developing DSA.
Immunosuppressive Medication
It is hypothesized that suboptimal drug adjustment and poor adherence to therapy, leading to inadequate TAC target levels, favors the development of DSA+ and secondarily leads to therapy intensification [35, 42]. Finally, inadequate immunosuppression is known to increase the risk of alloimmune reactions, including the formation of DSA+ and the occurrence of rejection reactions [27, 43].
Patient and Graft Survival
The patient survival of our entire cohort was 97%, the time between pLT and the time point under consideration being on average about 5 years. Thus, patient survival is comparable to the result of 97.5% for patients treated in Hannover, Germany, 2014–2020 [44]. The graft survival for the whole cohort was 87%, which is closely in line with data from other studies, which vary from 72% to 93% at 5 years after pLT [45, 46]. It was significantly higher for DSA− than for DSA+ in both groups.
Thus, the present results therefore suggest that the detection of DSA+ represents a risk factor for graft survival probability. Schluckebier and colleagues describe an association between rejection reactions and DSA+ in children but found no change in graft survival [47]. In contrast, other authors have reported reduced graft survival in DSA+ in children [27] and adults [48, 49]. Kaneku et al. found worse values for both graft and patient survival in adults with DSA+ detection [20].
Limitations
4.3
The retrospective design and the small pediatric cohort limit this monocentric study. The patients are heterogeneous in terms of their age at pLT and the time between pLT and DSA screening. Missing HLA‐typing of the donor (e.g., after pLT in other countries) was frequently an exclusion criterion. Only a single HLA Ab examination and its ensuing results were documented rather than those over a long‐term course. Longitudinal HLA Ab tests may be used as noninvasive prognostic biomarkers for rejection in addition to liver enzymes and invasive liver biopsy. Modern precision post‐transplant care mandates comprehensive analysis of serological, histological, and functional biomarkers for optimal patient and graft management.
Conclusions
5
DSA+ were detectable in 39% of children after pLT and associated with AMR in 13%. DSA+ were associated with poorer graft survival. Predictors for DSA included age at pLT, re‐pLT, and CF. Living donation and cold ischemia time <8 h were found to have a protective role. Routine DSA diagnostics are therefore recommended, particularly in cases of hepatopathy.
Author contributions
Evelien Kanaan: study design, investigation, data preparation, statistical analysis, writing. Elke Lainka: investigation, writing, review, editing, supervision, conceptualization. Simone Kathemann: investigation, drafting of manuscript, critical review. Lars Pape: critical review. Sinja Ohlsson: investigation, statistical analyses. Maren Schulze: critical review. Falko M. Heinemann: investigation, data preparation. Andreas Heinold: investigation, data preparation. Benas Prusinskas: investigation, critical review. Sofia Tsaka: investigation, critical review. All authors have read and agreed to the published version of the manuscript.
Funding
The author has nothing to report.
Conflicts of Interest
There are no conflicts of interest. All authors declare that they have no known competing financial and not financial interests that could have appeared to influence the work in this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. Wesson , E. Etchill , and J. Garonzik‐Wang , “Application and Interpretation of Histocompatibility Data in Liver Transplantation,” Current Opinion in Organ Transplantation 22, no. 5 (2017): 499–504.28708813 10.1097/MOT.0000000000000450 · doi ↗ · pubmed ↗
- 2S. Varma , J. Ambroise , M. Komuta , et al., “Progressive Fibrosis Is Driven by Genetic Predisposition, Allo‐Immunity, and Inflammation in Pediatric Liver Transplant Recipients,” e Bio Medicine 9 (2016): 346–355.27333038 10.1016/j.ebiom.2016.05.040PMC 4972529 · doi ↗ · pubmed ↗
- 3A. Miyagawa‐Hayashino , A. Yoshizawa , Y. Uchida , et al., “Progressive Graft Fibrosis and Donor‐Specific Human Leukocyte Antigen Antibodies in Pediatric Late Liver Allografts,” Liver Transplantation 18, no. 11 (2012): 1333–1342.22888064 10.1002/lt.23534 · doi ↗ · pubmed ↗
- 4N. Safinia , T. Vaikunthanathan , R. I. Lechler , A. Sanchez‐Fueyo , and G. Lombardi , “Advances in Liver Transplantation: Where Are We in the Pursuit of Transplantation Tolerance?,” European Journal of Immunology 51, no. 10 (2021): 2373–2386.34375446 10.1002/eji.202048875 PMC 10015994 · doi ↗ · pubmed ↗
- 5P. T. Kim , A. J. Demetris , and J. G. O'Leary , “Prevention and Treatment of Liver Allograft Antibody‐Mediated Rejection and the Role of the 'Two‐Hit Hypothesis,” Current Opinion in Organ Transplantation 21, no. 2 (2016): 209–218.26918881 10.1097/MOT.0000000000000275 · doi ↗ · pubmed ↗
- 6S. Feng , J. C. Bucuvalas , G. V. Mazariegos , et al., “Efficacy and Safety of Immunosuppression Withdrawal in Pediatric Liver Transplant Recipients: Moving Toward Personalized Management,” Hepatology 73, no. 5 (2021): 1985–2004.32786149 10.1002/hep.31520 PMC 12105584 · doi ↗ · pubmed ↗
- 7A. Demetris , C. Bellamy , S. Hübscher , et al., “2016 Comprehensive Update of the Banff Working Group on Liver Allograft Pathology: Introduction of Antibody‐Mediated Rejection,” American Journal of Transplantation 16, no. 10 (2016): 2816–2835.27273869 10.1111/ajt.13909 · doi ↗ · pubmed ↗
- 8A. Sánchez‐Fueyo and T. B. Strom , “Immunologic Basis of Graft Rejection and Tolerance Following Transplantation of Liver or Other Solid Organs,” Gastroenterology 140, no. 1 (2011): 51–64.21073873 10.1053/j.gastro.2010.10.059PMC 3866688 · doi ↗ · pubmed ↗