Uropathogenic Microorganisms After Pelvic Floor Surgery and Mid-Urethral Sling Application: Detection Under Different Culture Conditions
Georgios Balaouras, Polychronis Kostoulas, Vassiliki Koulourida, Paraskevas Ioannidis, Iakovos Theodoulidis, Eleni Siskou, Artemis Kolynou, Maria Paraskeva, Dimitrios Balaouras, Olympia Lioupi, Dimitrios Chitzios, Themistoklis Mikos

TL;DR
This study compares two urine culture methods to detect uropathogens after mid-urethral sling surgery, suggesting a more sensitive method could improve diagnostics and treatment.
Contribution
The study evaluates enhanced quantitative urine culture's potential for better pathogen detection after mid-urethral sling procedures.
Findings
Enhanced quantitative urine culture detected more uropathogens than conventional methods, though not statistically significant.
Key pathogens identified include Escherichia coli and Klebsiella pneumoniae with variable antibiotic resistance patterns.
The study suggests EQUC could improve postoperative diagnostics and targeted antibiotic therapy for mid-urethral sling patients.
Abstract
Urinary incontinence (UI) is a prevalent condition that significantly affects quality of life and healthcare systems. Stress urinary incontinence (SUI) is often treated with mid-urethral sling (MUS), a procedure associated with a risk of postoperative urinary tract infections. This study aimed to evaluate the effectiveness of enhanced quantitative urine culture (EQUC) for detecting uropathogens after MUS compared to conventional culture techniques. In total, 104 women of reproductive age and postmenopausal status were included. Thirty-five women with UI underwent MUS (cases), while 69 undergoing other pelvic floor reconstructions served as controls. Catheterized urine samples were collected preoperatively for both groups and postoperatively only for cases, yielding a total of 139 samples. Each sample was cultured using both conventional and EQUC methods. EQUC detected 66.6% (12 vs. 8…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
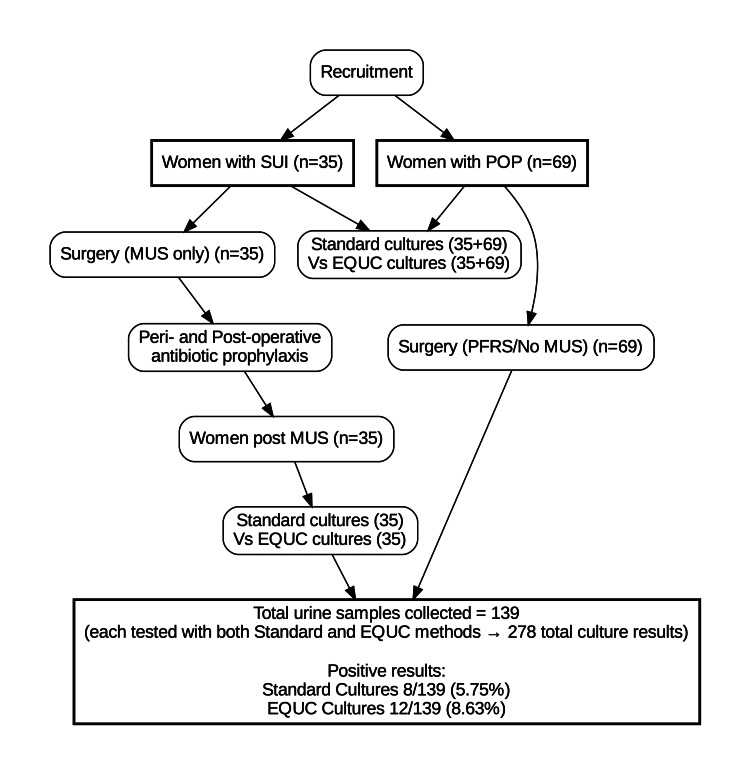 Figure 1
Figure 1| Variable | Study Group (MUS, n=35) | Control Group (POP, n=69) |
| Mean age (years) | 62.2 ± 11.3 | 65.7 ± 10.1 |
| Mean BMI (kg/m²) | 29.5 ± 5.4 | 27.5 ± 4.8 |
| Mean parity (n) | 2.3 ± 0.8 | 2.4 ± 0.9 |
| Postmenopausal, n (%) | 6 (16.7%) | 5 (7.2%) |
| Pathogen | Study Group (MUS, n=35) | Control Group (POP, n=69) | Total (n=104) |
| Escherichia coli | 2 (5.7%) | 2 (2.9%) | 4 (3.8%) |
| Klebsiella pneumoniae | 2 (5.7%) | – | 2 (1.9%) |
| Enterobacter cloacae | 1 (2.9%) | – | 1 (1.0%) |
| Enterococcus faecalis | – | 3 (4.3%) | 3 (2.9%) |
| Micrococcus luteus | 1 (2.9%) | – | 1 (1.0%) |
| Bacillus simplex | – | 1 (1.4%) | 1 (1.0%) |
| Total positive samples | 6 (17.1%) | 6 (8.7%) | 12 (11.5%) |
| Pathogen/Antibiotic | C1 | C2 | C3 | C4 | C5 | P1 | P2 | P3 | P3 | P1 |
| Pre-op. | Pre-op. | Pre-op. | Post-op. | Post-op. | ||||||
| Enterococcus faecalis | Escherichia coli | Klebsiella pneumoniae | Enterobacter cloacae | |||||||
| Ampicillin/Sulbactam | S | S | S | R | S | R | S | R | - | R |
| Amoxycillin/Clavulanic | S | S | - | - | - | - | - | R | R | - |
| Amikacin | R | R | - | S | S | S | S | R | R | S |
| Aztreonam | - | - | - | S | S | S | S | R | - | S |
| Cephalothin | - | - | R | - | - | - | - | - | - | - |
| Cefazolin | R | R | - | - | - | - | - | - | - | - |
| Cefepime | - | - | - | S | S | S | S | R | R | S |
| Cefixime | - | - | - | - | - | - | - | R | - | - |
| Cefotaxime | - | - | - | - | - | - | - | R | R | - |
| Cefoxitin | - | - | - | S | S | S | S | R | R | R |
| Ceftazidime | - | - | - | S | S | S | S | R | R | S |
| Ceftazidime/Avibactam | - | - | - | - | - | - | - | S | S | - |
| Ceftolozane/Tazobactam | - | - | - | - | - | - | - | R | R | - |
| Ceftriaxone | - | - | - | S | S | S | S | R | - | S |
| Chloramphenicol | - | - | - | - | - | - | - | S | - | - |
| Ciprofloxacin | R | R | S | S | S | R | S | R | R | S |
| Cinopristin/Dalfopristin | R | R | - | - | - | - | - | - | - | - |
| Clindamycin | - | - | R | - | - | - | - | - | - | - |
| Colistin | - | - | - | S | S | S | S | S | S | S |
| Daptomycin | S | S | S | - | - | - | - | - | - | - |
| Ertapenem | - | - | - | - | - | - | - | R | R | - |
| Erythromycin | - | - | I | - | - | - | - | - | - | - |
| Fosfomycin | - | - | - | S | S | R | S | R | R | S |
| Imipenem | I | I | S | S | S | S | S | R | - | S |
| Gentamycin | - | - | S | S | S | S | S | S | S | |
| Gentamycin-500 | SYN-R | SYN-R | S | - | - | - | - | - | - | - |
| Levofloxacin | - | - | - | S | S | R | S | R | - | S |
| Linezolid | S | S | I | - | - | - | - | - | - | - |
| Meropenem | - | - | - | S | S | S | S | R | R | S |
| Minicycline | - | - | - | - | - | - | - | - | - | - |
| Moxifloxacin | - | - | S | - | - | - | - | R | - | - |
| Nitrofurantoin | - | - | - | - | - | - | - | I | I | - |
| Piperacillin/Tazobactam | - | - | - | S | S | S | S | R | R | S |
| Streptomycin 2000 | SYN-S | SYN-S | S | - | - | - | - | - | - | - |
| Teicoplanin | S | S | S | - | - | - | - | - | - | - |
| Tetracycline | - | - | R | - | - | - | - | - | - | - |
| Tigecycline | S | S | S | S | S | S | S | ΙΕ | IE | IE |
| Tobramycin | - | - | - | - | - | - | - | R | - | - |
| Trimethorpim/Sulfamethoxazole | - | - | R | R | S | S | S | R | R | S |
| Vancomycin | S | S | S | - | - | - | - | - | - | - |
| EQUC + | EQUC – | Total | p-Value | |
| Standard + | 8 | 0 | 8 | - |
| Standard – | 4 | 127 | 131 | - |
| Total | 12 | 127 | 139 | Two-sided: 0.125; one-sided: 0.063 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Urinary Tract Infections Management · Urinary Bladder and Prostate Research
Introduction
Urinary incontinence (UI), defined as any complaint of involuntary loss of urine, is a prevalent and clinically significant condition [1-2] that affects millions worldwide, leading to substantial impacts on quality of life and health systems [3]. The World Health Organization recognizes UI as an international health problem [4], which affects approximately 17% of women aged ≥20 years and over 30-40% of elderly women [5-6]. Nearly half of all women who have given birth will experience some form of incontinence during their lifetime [7]. Furthermore, stress urinary incontinence (SUI) is the most common subtype with considerable economic and psychosocial burdens [8], while urge UI, often linked to detrusor overactivity, and mixed or overflow types account for additional cases [9]. Since the introduction of the retropubic tension-free vaginal tape (TVT) in 1996 [10], the mid-urethral sling (MUS) has become the gold standard surgical treatment for SUI and stress-dominant mixed incontinence. Long-term data demonstrate high subjective and objective cure rates and patient satisfaction up to five years post-surgery [11-13].
When MUS is performed, often in combination with other pelvic reconstruction procedures, the postoperative risk of urinary tract infection (UTI) increases [14-16]. Surgical-specific factors such as intraoperative catheterization, tissue trauma, and the presence of a synthetic foreign body further predispose to infection, with reported postoperative UTI rates after MUS varying widely from 7-13% in some series to as high as 30-40% within the first six weeks [17-19]. Although international guidelines recommend preoperative antibiotic prophylaxis in clean-contaminated pelvic procedures, there has been little consensus on optimal postoperative regimens, including antibiotic type, route, or duration. In a retrospective observational Greek study, Escherichia coli was the most frequently isolated pathogen, alongside Klebsiella pneumoniae, Proteus mirabilis, and Enterococcus faecalis. This indicates a diverse microbial profile of postoperative infections following MUS placement [20]. However, no studies have yet examined the optimal microbiological conditions for detecting such uropathogens. Unlike standard urine culture techniques, which use conventional media and 24-hour incubation, the enhanced quantitative urine culture (EQUC) method employs extended incubation and multiple media and could have the potential to improve the recovery of low-concentration or fastidious organisms.
The aim of this study was to evaluate whether the modification of traditional urine culture conditions and the use of EQUC enhance the detection of uropathogenic microorganisms in comparison to conventional culture techniques in women undergoing MUS surgery and pelvic floor reconstruction.
Materials and methods
Study design and participants
This was a prospective case-control study conducted from August 2023 to September 2024 in a tertiary university hospital, with close collaboration of the Microbiology and the Urogynecology departments. Local ethics committee approval was obtained as appropriately (Protocol No 2023-B2015-271). A community control group was not included because the study was restricted, by design, to women undergoing pelvic surgery.
Inclusion criteria were (1) women with SUI who did not have clinically significant pelvic organ prolapse (POP) (the study group) and (2) women with POP who did not have USI (the control group).
Exclusion criteria were (1) age <18 years, (2) women who did not consent for any surgical intervention, (3) patients with SUI who had previous incontinence surgery, (4) patients with POP who had previous prolapse surgery, (5) women unsuitable for regional/general anesthesia, and (6) women with history of recurrent UTI. Controls were age-matched at recruitment.
A total of 104 women, both of reproductive age and postmenopausal, participated in the study. Specifically, it included 35 women with UI (cases), who underwent the application of free-tension synthetic slings (MUS), and 69 age-matched women (controls), who had undergone pelvic floor reconstruction surgery (PFRS), including anterior and posterior colporrhaphy, as well as vaginal hysterectomy. Sample size reflected all consecutive eligible patients within the 13-month period.
In both the group of women, demographic data and clinical history were recorded, and the necessary clinical examinations and urodynamic testing were performed. In the control group, only demographic data and clinical history were recorded. The collection and analysis of the data were conducted in accordance with the Declaration of Helsinki of 1975.
For the women who underwent synthetic MUS tape application and PFRS other than hysterectomy, patients were discharged the day after surgery, while those who PFRS and vaginal hysterectomy were discharged after three days. In both groups of patients, a seven-day course of chemoprophylaxis (second-generation cefalosporin, or clindamycin in cases of allergies) was prescribed. This extended regimen reflects our institutional infection-control protocol for gynecologic reconstructive procedures involving the placement of foreign material. The choice of second-generation cephalosporins aligns with their broad coverage of common Gram-negative and Gram-positive uropathogens and their established efficacy in pelvic surgery prophylaxis.
Broad-spectrum antibiotics were used, while the selection took into account the resistance profile presented by strains isolated from nosocomial infections at the given time. According to the CLSI (Clinical and Laboratory Standards Institute), three categories are recognized to characterize the effect of the antibiotic on the microbe under examination: sensitive, intermediate sensitivity, and resistant [21]. The flow of participants through the study is illustrated in Figure 1.
Flow diagram of participant selection, group classification, and urine sample collection.A total of 139 urine samples were collected (104 preoperative and 35 postoperative). Each sample was cultured using both Standard and EQUC methods, resulting in 278 total culture results.EQUC, expanded quantitative urine culture; MUS, mid-urethral sling; POP, pelvic organ prolapse; PFRS, pelvic floor reconstructive surgery; SUI, stress urinary incontinence
Urine sample collection and culture techniques
Post-operative urine collection was standardized at one to three weeks after completion of prophylaxis. Laboratory personnel performing cultures were blinded to patient group. A urinalysis was performed (taking a catheterized urine sample and carrying out a urine culture) in each patient, as part of the regular outpatient clinic check, as well as a comparison of these results. A urine sample was taken as part of the preoperative control in both groups under observation, while a urine sample was taken again postoperatively (at the post-operative visit one to three weeks after the completion of the post-operative prophylactic treatment) only for the study group (cases). All urine samples were transported immediately to the microbiology laboratory and processed within 1 hour of collection. In total, 139 urine samples were collected: 104 preoperative (one per patient) and 35 postoperative from the MUS group. Each sample was processed with both Standard and EQUC methods, yielding 278 total culture results.
Urine culture is the criterion standard for the diagnosis of UTI. The quantitative urine culture consists of inoculating 1 μL of urine using a calibrated loop or 5 μL of urine, depending on the diameter of the loop, into a citrate lactose electrolyte deficient (CLED) agar plate. Selective and differential mediums, such as MacConkey agar and Columbia colistin-nalidixic agar (CNA), can be used also. After 24-hour incubation at 35°C, the number of colonies is counted in order to calculate the number of microorganisms per milliliter.
In this study, a “positive” urine culture was defined as ≥10³ CFU/mL, consistent with the Infectious Diseases Society of America (IDSA) and European Association of Urology (EAU) recommendations for catheterized urine specimens in symptomatic patients. Urine cultures were classified as “negative” if they yielded growth of a uropathogen(s) at a count <10^3^ CFU/mL, or showed mixed growth of normal flora (staphylococci, or streptococci etc.).
All participants provided catheterized urine samples following a standardized collection protocol to minimize contamination. Samples were promptly processed and cultured using both conventional and enhanced urine culture techniques. The conventional method involved plating 1 μL of urine on blood agar plates (BAPs) and MacConkey agar, followed by aerobic incubation at 35°C for 24 hours.
For enhanced detection, a more comprehensive set of conditions (EQUC) was utilized. This included plating (a) 1 μL of urine on BAPs (BAP) and MacConkey agar, followed by incubation at 35°C, in 5% CO_2_, for 24 hours at first and for extra 24 hours, if bacterial growth was observed, and (b) 100 μL of urine on BAP, chocolate agar, and CNA agar, incubated in 5% CO_2_ at 35°C for 48 hours.
Microbial identification
Bacterial colonies were quantified and identified using standard microbiological techniques, including matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Only clinically relevant uropathogens were included in the analysis.
Statistical analysis
Data were analyzed using descriptive statistics to compare outcomes between the two groups. Because of the exploratory sample size, formal multivariable adjustment was not feasible. For paired comparison of culture methods (standard vs. EQUC), McNemar’s exact test was used. Both two-sided and one-sided tests were performed: the two-sided p-value assessed overall discordance between methods, while the one-sided test specifically evaluated whether EQUC detected significantly more positives than the standard method, reflecting its hypothesized higher sensitivity. P-values <0.05 were considered statistically significant. Analyses were performed in R (version 4.4.0, R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 104 Caucasian women were consecutively enrolled in the study. Baseline characteristics are summarized in Table 1.
In the study group, all patients had SUI or mixed UI, whereas in the control group, no patient had SUI. All patients in the study group underwent MUS placement: 31 had a mini-sling under local anesthesia, 3 had a trans-obturator tape under local anesthesia, and 1 had a retropubic tape under regional anesthesia. In the control group, all women underwent prolapse surgery without any anti-incontinence procedure: 18 (26.1%) had anterior-posterior colporrhaphy only, 33 (47.8%) had vaginal hysterectomy and anterior-posterior colporrhaphy, 7 (10.1%) had sacrospinous ligament fixation of the vaginal vault and anterior-posterior colporrhaphy, and 5 (7.2%) had colpocleisis.
The results from the cases group are presented below, separated into both preoperative and postoperative findings across conventional and enhanced culture conditions.
Preoperative findings
In the cases group, six positive samples were identified, four of which were preoperative. Specifically, three samples showed positive results across all conditions, both conventional and EQUC. These included two Escherichia coli isolates and one Klebsiella pneumoniae isolate. All of them, with bacterial growth at a count >10^5^ CFU/mL of urine, while one sample was positive only under EQUC conditions. This was a Micrococcus luteus isolate, with bacterial growth equal to 10^3^ CFU/mL.
Postoperative findings
Additionally, two postoperative samples were positive under both conventional and EQUC conditions: one Enterobacter cloacae isolate and one Klebsiella pneumoniae isolate, both with bacterial growth at a count >10^5^ CFU/mL.
Similarly, in the control group, six positive samples were identified. Three of these samples were positive under all conditions, both conventional and EQUC, including two (2) Escherichia coli isolates and one (1) Enterococcus faecalis isolate. All of them had bacterial growth at a count >10^5^ CFU/mL. Additionally, three samples were positive only under EQUC conditions, comprising two Enterococcus faecalis isolates, with bacterial growth at a count >10^5^ CFU/mL and one Bacillus simplex isolate, with bacterial growth equal to 10^3^ CFU/mL.
The microorganisms detected in this study were all clinically relevant, as the women reported symptomatic UTIs. These pathogens are considered opportunistic, meaning they can cause infections when the body’s defenses are compromised, such as after surgical procedures such as MUS. Even the patients in whom Micrococcus luteus and Bacillus simplex isolates were detected manifested clinical symptoms of UTI and had a positive urine test preoperatively (WBCs=63/μL and WBCs=742/μL, NR: 0-25/μL, respectively). The detection of these opportunistic pathogens underscores the importance of accurate microbial identification, as these organisms, although not always harmful, can lead to clinically significant infections in susceptible individuals, particularly in a postoperative setting. This highlights the need for thorough pathogen evaluation to ensure appropriate treatment and management of UTIs in these patients.
The microorganisms identified in both the cases and control groups, as mentioned above, included Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Enterococcus faecalis, Micrococcus luteus, and Bacillus simplex (Table 2), most of which are known to be clinically relevant uropathogens, whereas Micrococcus luteus and *Bacillus simplex *are considered opportunistic or environmental species. Their detection underscores the sensitivity of the EQUC method, yet their pathogenic role in postoperative urinary infections should be interpreted cautiously.
More specifically, the uropathogenic microorganisms identified in this study included Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae, Enterococcus faecalis, Micrococcus luteus, and Bacillus simplex:
*Escherichia coli *was identified under all conditions in both the case and control groups (four samples, all preoperatively, >10^5^ CFU/mL). It is a Gram-negative bacterium that colonizes the gastrointestinal tract. *Escherichia coli *is the most common cause of UTIs, leading to symptoms such as dysuria, urinary frequency, and, in severe cases, pyelonephritis.
Klebsiella pneumoniae was identified in the case group under all conditions (two samples, one preoperatively and the other postoperatively, both >10^5^ CFU/mL). It is a Gram-negative bacterium commonly found in the gastrointestinal tract and also responsible for UTIs [22-23]. It is frequently associated with hospital-acquired infections and is known for its multidrug resistance, complicating treatment efforts [24].
Enterobacter cloacae was identified in the case group under all conditions (one postoperative sample, >10^5^ CFU/mL). It is a Gram-negative bacterium commonly found in the gastrointestinal tract and a known causative agent of UTIs [25]. It is frequently associated with nosocomial infections, particularly in catheterized patients, and exhibits significant antibiotic resistance, complicating treatment [26].
*Enterococcus faecalis *was identified in the control group (three samples, >10^5^ CFU/mL). One sample was detected under all conditions, while the other two were identified after the inoculation of 100 μL of urine on MacConkey agar, blood agar, and CNA agar, incubated at 35°C in 5% CO₂ for 48 hours, as part of the enhanced urine culture protocol (EQUC). This Gram-positive bacterium, commonly residing in the gastrointestinal tract, is frequently associated with UTIs [27]. It poses significant challenges due to its antibiotic resistance, including resistance to vancomycin [28].
*Micrococcus luteus *was identified in the case group (one sample, 10^3^ CFU/mL) after the inoculation of 100 μL of urine on MacConkey agar, blood agar, and CNA agar, incubated at 35°C in 5% CO₂ for 48 hours, as part of the enhanced urine culture protocol (EQUC). Micrococcus luteus is a Gram-positive coccus of the Micrococcaceae family, widely distributed in the environment, including soil, air, water, and animals. It can also be found on human skin and mucous membranes [29]. Although Micrococcus luteus is rarely reported in clinical cases, it has been known to affect vulnerable patient groups, such as malnourished individuals and those with weakened immune systems [30].
Bacillus simplex was identified in the control group (one sample, 10^3^ CFU/mL) following the inoculation of 1 μL of urine on MacConkey agar and blood agar, incubated at 35°C in 5% CO₂ for 24 hours, with an additional 24-hour incubation (48 hours total), as part of the enhanced urine culture protocol (EQUC). This Gram-positive, spore-forming, rod-shaped bacterium is primarily found in the environment. Bacillus species are aerobic or facultatively anaerobic and, while typically environmental organisms, can cause opportunistic infections under certain conditions, particularly in immunocompromised individuals [31]. Although rare, Bacillus simplex may lead to UTIs in susceptible patients. To further examine the effectiveness of antibiotic treatments and the prevalence of resistance among detected uropathogens, Table 3 provides a comparative summary of antibiotic treatments and the corresponding sensitivity profiles for pathogens identified in MUS patients and control participants. This table highlights the antibiotics used, treatment timing, and sensitivity or resistance patterns observed, facilitating an analysis of resistance trends in each group. By distinguishing preoperative and postoperative phases, these data help illustrate the influence of MUS procedures on microbial sensitivity and resistance, offering essential insights for targeted antibiotic management. These results underscore the variability in resistance patterns and the necessity of selecting appropriate antibiotics, as further explored in the pathogen-specific analysis below.
These resistance profiles (Table 3) reveal that Klebsiella pneumoniae and Enterobacter cloacae exhibited multidrug-resistant patterns against several β-lactams and fluoroquinolones, while maintaining sensitivity to carbapenems and colistin, while Escherichia coli isolates demonstrated more variable resistance, particularly to ciprofloxacin and trimethoprim-sulfamethoxazole. These patterns are consistent with globally recognized nosocomial multidrug-resistant lineages and emphasize the clinical need for postoperative antimicrobial stewardship and culture-guided therapy following MUS procedures. These findings are clinically relevant, as they highlight the need for individualized antibiotic therapy based on culture results rather than empirical postoperative regimens.
To further evaluate differences between culture methods, a paired analysis was performed across all 139 urine samples. Considering all 139 paired urine samples, standard culture detected eight (5.75%) positives and EQUC detected 12 (8.63%) positives. The paired cross-classification is shown in Table 4. Eight samples were positive by both methods, four were positive only by EQUC, and none were positive only by standard culture (127 were negative by both). Notably, no samples were positive on standard culture but negative on EQUC, consistent with the broader conditions of EQUC. McNemar’s exact test on the discordant pairs indicated a non-significant trend toward higher sensitivity of EQUC (two-sided p = 0.125; one-sided p = 0.063).
Overall, the antibiotic sensitivity profiles observed in Table 3 underscore the necessity for personalized antibiotic selection in managing UTIs, especially in postoperative MUS patients, to enhance treatment efficacy and mitigate resistance development. Although Table 3 illustrates variable resistance across the isolated uropathogens, with multidrug-resistant profiles in Klebsiella pneumoniae and Enterobacter cloacae, these findings should be interpreted with caution due to the limited number of isolates per species. The observed resistance to multiple β-lactams and fluoroquinolones in these organisms aligns with their known hospital-acquired multidrug-resistant phenotypes. However, a detailed statistical or genotypic resistance analysis was beyond the scope of this work and will be presented in a forthcoming study focusing specifically on antimicrobial susceptibility trends in postoperative pelvic surgery patients.
Discussion
The results of this study provide significant insights into the effectiveness of EQUC methods for detecting uropathogens. When comparing EQUC with standard culture, McNemar’s exact test showed that the increase in detection with EQUC was not statistically significant in the two-sided test (p = 0.125). However, the one-sided test, performed to evaluate the specific hypothesis that EQUC is more sensitive, yielded a p-value of 0.063, suggesting a trend toward superior detection by EQUC. Although under-powered, this finding supports the biological plausibility of EQUC offering enhanced sensitivity, as the expanded culture conditions are designed to detect fastidious or low-concentration organisms. Larger studies will be needed to confirm whether this trend reflects a true diagnostic advantage. In the cases group, both preoperative and postoperative infections were identified through EQUC, confirming its ability to detect clinically significant pathogens such as *Enterobacter cloacae *and Klebsiella pneumoniae. These pathogens are known to contribute to postoperative complications, particularly in women who have undergone MUS procedures [23,25]. Both Klebsiella pneumoniae and Enterobacter cloacae exhibited multidrug-resistant profiles in our isolates, which is consistent with their well-established role as hospital-acquired pathogens. This resistance to several β-lactams and fluoroquinolones, combined with preserved susceptibility to carbapenems and colistin, underscores the need for postoperative antimicrobial stewardship and culture-guided therapy following MUS procedures. Furthermore, no cases were observed where standard culture was positive and EQUC was negative, consistent with the expanded methodological basis of EQUC and suggesting that EQUC could encompass the diagnostic capacity of standard culture.
In both groups (cases and controls), the EQUC revealed positive results in four samples that were not detected using conventional methods. Pathogens such as Enterococcus faecalis, Micrococcus luteus, and Bacillus simplex were isolated only through the EQUC process, suggesting that these microorganisms, particularly when present in lower concentrations or requiring specific growth conditions, may be missed with traditional culture techniques. This highlights the limitations of conventional methods and underscores the importance of adopting more comprehensive diagnostic approaches such as EQUC. The detection of low-concentration pathogens such as Micrococcus luteus and Bacillus simplex is clinically significant, particularly in postoperative or immunocompromised patients. While these microorganisms are often considered part of the normal flora or environmental contaminants, their presence in catheterized urine samples and their association with elevated leukocyte counts suggest a potential role in postoperative UTIs. It should also be noted that the broader sensitivity of EQUC inherently increases the likelihood of detecting environmental or commensal organisms. Hence, distinguishing true pathogens from contaminants remains an important consideration for clinical application.
Specifically, Micrococcus luteus, although rarely pathogenic, has been reported in immunosuppressed individuals and malnourished patients, where it can cause opportunistic infections. Similarly, Bacillus simplex, typically an environmental organism, may lead to clinically significant infections in vulnerable populations. Their detection underscores the importance of advanced diagnostic methods such as EQUC, which are capable of identifying these pathogens in scenarios where traditional methods might miss them.
This capability is crucial in tailoring appropriate antimicrobial therapies, as low-concentration pathogens might contribute to persistent or recurrent infections if left untreated. Moreover, understanding the clinical relevance of such organisms can help refine postoperative management protocols, minimizing the risk of complications. These findings further highlight the diagnostic advantages of EQUC. Specifically, the EQUC cultures isolated microorganisms more frequently than conventional cultures, with a higher frequency observed among controls (3/69) compared to cases (1/70). Although this finding was not statistically significant, it underscores EQUC’s enhanced sensitivity, particularly in detecting pathogens present in lower bacterial loads or requiring specific growth conditions. This capability is crucial for ensuring accurate diagnosis and optimizing clinical management in challenging cases.
The increased pathogen detection in both groups, particularly the control group, emphasizes the potential for underdiagnosis when relying solely on conventional cultures. The ability to identify additional uropathogens has critical implications for improving diagnostic accuracy and ensuring appropriate clinical management. In particular, EQUC proves vital in detecting opportunistic pathogens that may not always be pathogenic in healthy individuals but can cause significant infections in postoperative patients, where immune defenses are often compromised. No association was found between the presence of uropathogens (detected by either method) and preoperative or postoperative clinical symptoms, including stress incontinence, overactive bladder symptoms, or postoperative tape erosion.
Moreover, this study is pioneering in Greece, as it introduces the use of varied culture conditions that have not previously been applied. Until now, standard urine culture methods in Greece have consistently used the same culture conditions, potentially overlooking key pathogens. By incorporating EQUC into the study design, this research marks a significant step forward in enhancing diagnostic capabilities and providing a more comprehensive understanding of UTIs in clinical settings. Furthermore, adopting more sensitive diagnostic techniques such as EQUC can be seen as a clinically and ethically relevant consideration, as it may enhance diagnostic accuracy and reduce complications through more targeted treatment. While improved detection does not automatically translate into superior outcomes, implementing more comprehensive testing aligns with good clinical practice and patient-centered care principles [32-33]. However, EQUC also presents practical challenges, including increased laboratory workload, higher costs, and the need for standardized interpretation criteria, which may currently limit its widespread clinical adoption. Timely and precise diagnosis of infections allows healthcare provides to administer targeted treatments, minimizing unnecessary antibiotic use and reducing risk of antimicrobial resistance.
This study further underscores the value of thorough culturing in postoperative patients. The detection of opportunistic pathogens in both the cases and control groups highlights the need for comprehensive microbiological assessments in patients undergoing procedures such as MUS. Although many of these pathogens may be part of the normal flora, in immunocompromised or postoperative patients, they can lead to severe UTIs. Therefore, the use of enhanced detection methods, such as EQUC, is crucial in identifying and managing these infections early. An increased prevalence of positive urine cultures (both conventional and EQUC) was observed in older women, potentially reflecting the known higher incidence of asymptomatic bacteriuria in this population. The clinical relevance of this finding remains unclear, as bacterial isolation did not correlate with clinical symptoms or pathology, suggesting that further investigation is warranted.
The link between the detected pathogens and the clinical manifestations of UTIs further supports the importance of advanced culture techniques. All detected microorganisms were clinically relevant, as the women presented with urinary symptoms consistent with infection. This association underlines the need for more detailed microbial analysis, particularly in cases where conventional methods might fail to detect low-level or fastidious pathogens, leading to underdiagnosis and, consequently, inappropriate or delayed treatment.
Given these findings, there is a clear need to revisit and improve diagnostic protocols for UTIs, particularly in postoperative patients. The integration of enhanced culture techniques such as EQUC into routine clinical practice could lead to more accurate identification of uropathogens, enabling targeted antibiotic treatments and reducing the risk of persistent or recurrent infections. This is especially relevant in surgical contexts such as MUS, where the early and precise detection of pathogens can prevent complications and improve patient outcomes. From a clinical perspective, the application of EQUC could refine several aspects of perioperative care. Preoperatively, EQUC may help identify low-level colonization that could inform tailored antibiotic prophylaxis, particularly in women with prior urinary symptoms or risk factors for infection, while, postoperatively, its use could enable earlier detection of subclinical or persistent infections and, hence, allow more precise and timely interventions. Beyond these practical implications, an additional interesting observation was that all positive EQUC cultures were found in patients with a BMI below 27, the cohort’s mean BMI. This preliminary observation may reflect hormonal or metabolic factors associated with BMI that influence susceptibility to bladder colonization. However, this remains speculative, and further studies are required to validate this hypothesis.
Despite its strengths, this single-center feasibility study has that should be acknowledged. The relatively small sample size and unequal group sizes, without lack of full matching, may limit the generalizability of the findings. Nevertheless, key demographic characteristics such as age and menopausal status were comparable between groups. Postoperative urine cultures were not obtained from the control group, thus restricting the ability to assess potential asymptomatic or delayed infections after prolapse repair without MUS placement. Furthermore, the absence of a non-surgical, community-based control group also limits comparison with baseline urinary tract colonization in the general population. Finally, the extended seven-day antibiotic prophylaxis reflects institutional infection-control policy for reconstructive pelvic surgery and may have influenced postoperative infection rates. Although EQUC demonstrated technical feasibility within a routine clinical laboratory, larger multicenter studies with broader control groups are required to validate and extend these observations.
In conclusion, this study highlights the enhanced sensitivity of the EQUC method over conventional urine culture techniques in detecting clinically relevant uropathogens [34], particularly in postoperative MUS patients. Nevertheless, as EQUC remains a resource-intensive technique, further research should evaluate its cost-effectiveness, reproducibility across laboratories, and potential impact on clinical decision-making before routine implementation. The findings demonstrate the ability of EQUC to identify uropathogens that may be missed by traditional methods, emphasizing the potential for improved diagnostic accuracy in clinical practice. The EQUC’s demonstrated ability to detect low-concentration and fastidious pathogens highlights its potential to improve diagnostic accuracy and guide targeted antimicrobial therapy, ultimately reducing postoperative complications and antibiotic resistance. Future studies with larger cohorts and diverse populations are essential to validate these findings and establish EQUC as a gold standard in uropathogen detection.
Conclusions
The antibiotic sensitivity profiles observed underscore the variability of resistance among detected uropathogens, particularly *Escherichia coli *and Klebsiella pneumoniae. Such findings highlight the potential of EQUC to provide a more detailed microbiological picture than conventional methods. EQUC may improve pathogen detection and thereby inform antibiotic selection. However, further studies with larger cohorts are required to determine whether these microbiological advantages translate into clinical benefit. There is need of multicenter studies to evaluate further the feasibility, cost-effectiveness, and patient impact of EQUC-guided diagnostics in postoperative care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Consensus document on the management of urinary incontinence in older people Eur Geriatr Med Aharony L De Cock J Nuotio MS 21021582017
- 2An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction Int Urogynecol J Haylen BT de Ridder D Freeman RM 5262120101993731510.1007/s 00192-009-0976-9 · doi ↗ · pubmed ↗
- 3Urinary incontinence prevalence: results from the National Health and Nutrition Examination Survey J Urol Dooley Y Kenton K Cao G Luke A Durazo-Arvizu R Kramer H Brubaker L 65666117920081808221110.1016/j.juro.2007.09.081 · doi ↗ · pubmed ↗
- 4A quality of life survey of individuals with urinary incontinence who visit a self-help website: implications for those seeking healthcare information J Clin Psychol Med Settings Rozensky RH Tovian SM Gartley CB Nichols TR Layton M 2752832020132361586010.1007/s 10880-013-9361-4 · doi ↗ · pubmed ↗
- 5Prevalence and trends of symptomatic pelvic floor disorders in U.S. women Obstet Gynecol Wu JM Vaughan CP Goode PS Redden DT Burgio KL Richter HE Markland AD 14114812320142446367410.1097/AOG.0000000000000057 PMC 3970401 · doi ↗ · pubmed ↗
- 6Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI)Int Continence Soc Altman D Cartwright R Lapitan MC Milsom I Nelson R Sjöström S Tikkinen KAO 1735 Tokyoincontinence: 6th International Consultation on Incontinence 2016 https://researchportal.helsinki.fi/en/publications/epidemiology-of-urinary-incontinence-ui-and-other-lower-urinary-t
- 7The prevalence of urinary incontinence 20 years after childbirth: a national cohort study in singleton primiparae after vaginal or caesarean delivery BJOG Gyhagen M Bullarbo M Nielsen TF Milsom I 14415112020132241383110.1111/j.1471-0528.2012.03301.x · doi ↗ · pubmed ↗
- 8High costs of urinary incontinence among women electing surgery to treat stress incontinence Obstet Gynecol Subak LL Brubaker L Chai TC 89990711120081837874910.1097/AOG.0b 013e 31816 a 1e 12PMC 2593129 · doi ↗ · pubmed ↗