Improving renal transplant outcomes through the tubeless anesthesia technique in renal transplantation: a retrospective study
Chuanbao Chen, Jingfeng Ou, Guanyi Wu, Hui Liu, Hanyu Yang, Shaojie Fu, Zhihong Ran, Junbiao Xie, Xin Xu, Jianxing He, Chao Yang, Xiaoyou Liu

TL;DR
This study shows that using tubeless anesthesia in kidney transplants reduces drug use and speeds up recovery, with early benefits for graft function.
Contribution
The study introduces tubeless anesthesia as a feasible alternative in renal transplantation with demonstrated clinical benefits.
Findings
TA reduced cisatracurium and sufentanil doses and improved recovery times.
TA was associated with lower serum creatinine levels at 90 days post-transplant.
TA reduced airway complications and vasoactive agent use compared to ETT.
Abstract
To evaluate the feasibility and benefits of tubeless anesthesia (TA), using a laryngeal mask airway instead of endotracheal intubation (ETT), in renal transplantation, aligning with tubeless surgery principles. A single-center, retrospective matched-cohort study compared perioperative outcomes and 90-day graft function between TA and ETT in kidney transplantation. 52 adult recipients (26 TA, 26 ETT) operated between July-December 2024 were included. Groups were balanced for age, BMI, ASA classification, and dialysis duration. The Mann-Whitney U test and T test (SPSS 22.0) were used to analyze the outcome indicators: intraoperative anesthetic management, hemodynamics, recovery parameters, and graft function. The TA group required significantly lower median doses of cisatracurium (12.6 mg vs. 26.1 mg; p < 0.001) and sufentanil (22.3 µg vs. 28.7 µg; p = 0.026). Operative times were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
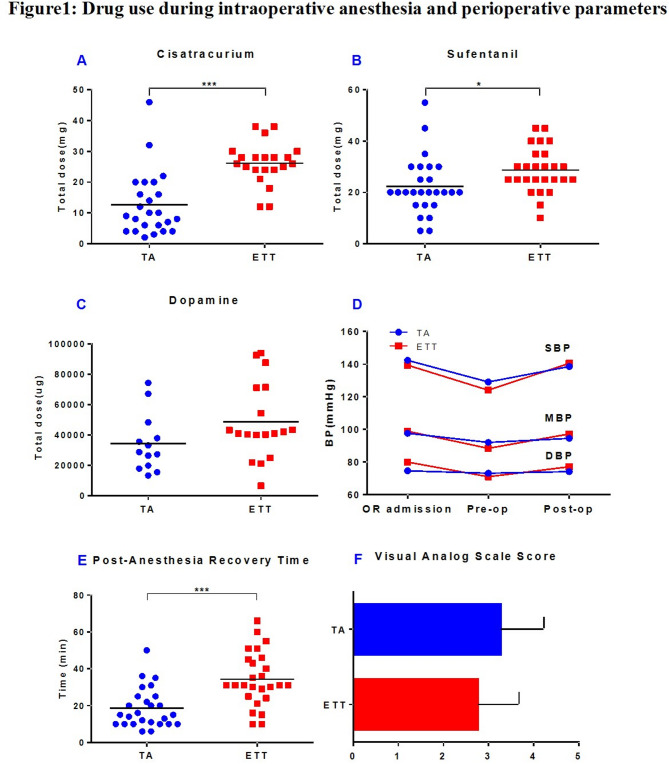 Figure 1
Figure 1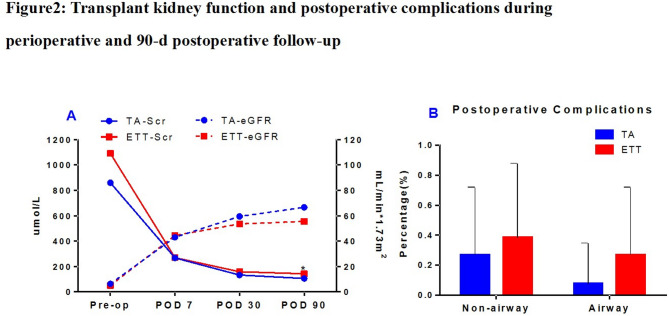 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Donation and Transplantation · Renal and Vascular Pathologies · Renal Transplantation Outcomes and Treatments
Introduction
Kidney transplantation is the optimal treatment for end-stage renal disease (ESRD), offering substantial improvements in patient survival and quality of life [1]. While advancements in surgical techniques have increased procedural success rates [2], anesthesia management continues to present significant challenges [3]. Endotracheal tube general anesthesia (ETT) remains the predominant approach for kidney transplantation globally [4] owing to its operational simplicity and safety profile. However, this method has notable drawbacks [5]. ETT elicits a pronounced stress response, which may lead to hemodynamic instability or cardiac complications [6–8] Furthermore, endotracheal intubation disrupts the respiratory mucosa’s natural barrier [7], and prolonged mechanical ventilation increases the risk of ventilator-associated pneumonia (VAP). ETT also necessitates high doses of anesthetic drugs, including muscle relaxants, sedatives, and opioids, drugs metabolized by the kidneys, potentially exacerbating toxicity to the transplanted organ [9]. Considering that it takes time for kidney transplant recipients to recover their renal function after surgery, postoperative recovery is usually long, and the awakening time is delayed. Frequent complications, such as sore throat and hoarseness [5], impair patient comfort and hinder rehabilitation.
The emerging paradigm of Tubeless surgery offers a transformative approach to surgical and perioperative management models [9–12] This strategy prioritizes physiological optimization and emphasizes precision medicine through individualized, physiologically driven management. Adapting this concept to kidney transplantation holds promise for refining anesthesia strategies, promoting patient early rehabilitation, and potentially improving long-term graft survival.
TA represents a pivotal innovation in this context. By replacing endotracheal intubation with a laryngeal mask, airway trauma can be prevented, and the hemodynamic stress response can be mitigated [13, 14]. In adult patients undergoing abdominal or head and cervicothoracic surgeries, ETT is associated with a higher incidence of postoperative complications such as hoarseness, cough, sore throat, and dysphagia [15, 16]. Regional nerve blocks, combined with titrated intravenous anesthesia, maintain adequate surgical conditions while reducing reliance on muscle relaxants and opioids [17]. In thoracic surgery, this anesthesia method helps maintain spontaneous breathing and rapid recovery after surgery and restores advanced cognitive functions as soon as possible, minimizing surgical trauma and anesthesia-related side effects, helping to shorten hospital stays and reduce medical costs [10, 18]. To date, only one study has briefly compared ventilation effectiveness and complications between ETT and TA in kidney transplantation [19]. No systematic analysis has been conducted regarding intraoperative anesthetic drug consumption, vital sign stability, or postoperative renal function. Considering the compromised renal function and immune status of transplant recipients, tubeless anesthesia may offer particular advantages in this setting.
In this study, we used a laryngeal mask airway instead of endotracheal intubation and combined intravenous anesthesia with regional blockade, which reduced the use of intraoperative anesthetic drugs (such as muscle relaxants and opioids), stabilized intraoperative hemodynamics, shortened the postoperative recovery time, effectively reduced the occurrence of respiratory complications, and improved the postoperative comfort of patients. This highlights the potential of the TA in optimizing transplant surgery and perioperative management.
Materials and methods
Case selection
We conducted a retrospective analysis of ESRD patients who underwent TA kidney transplantation at the First Affiliated Hospital of Guangzhou Medical University between July and December 2024. The donor kidneys were allocated via the China Organ Transplant Response System (COTRS). All the TA recipients met the predefined inclusion criteria during the preoperative anesthesia assessment. A total of 26 patients successfully underwent TA kidney transplantation. For comparative analysis, 26 contemporaneous ETT kidney transplant recipients were selected as controls. All the recipients who underwent TA kidney transplantation provided informed consent and signed the informed consent form.
Inclusion criteria for tubeless anesthesia
(1) Body mass index (BMI) < 28 kg/m²; (2) absence of severe pulmonary dysfunction, confirmed by preoperative pulmonary function assessment and chest CT; (3) normal cardiac function (ejection fraction >50%) without significant arrhythmias (e.g., frequent atrial fibrillation or ventricular ectopy); (4) American Society of Anesthesiologists (ASA) classification ≤ III [20]; (5) ethically approved eligibility for kidney transplantation per review by the hospital’s human organ transplantation ethics committee; (6) appropriate donor kidneys were matched according to the distribution principles of the COTRS system [21].
Anesthesia protocols
Tubeless anesthesia
Induction
Sufentanil (0.1–0.2 µg/kg, intravenous), propofol (target-controlled infusion [TCI] 2–3 µg/mL). A double-lumen laryngeal mask was inserted at Bispectral Index (BIS) < 40.
Maintenance
Propofol (TCI 0.5–2.0 µg/mL), remifentanil (0.03–0.1 µg/kg/min), and dexmedetomidine (0.3–1.0 µg/kg/h) were used to maintain stable anesthesia.
Regional block
Bilateral transversus abdominis plane (TAP) blocks under ultrasound guidance with 15–20 mL 0.375% ropivacaine per side [22, 23].
Muscle relaxants
Routinely use cisatracurium (initial bolus: 2–10 mg), titrated to surgical needs.
ETT anesthesia
Standard tracheal intubation with conventional general anesthesia was performed.
Intraoperative monitoring
Hemodynamics
Continuous ECG, heart rate (HR), invasive arterial pressure (IBP), and central venous pressure (CVP). Real-time monitoring of circulatory status is needed to ensure circulatory stability and reduce the impact on the perfusion of the transplanted kidney.
Respiratory metrics
Pulse oximetry (SpO₂), end-tidal CO₂ (EtCO₂), tidal volume (VT), respiratory rate (RR), and Fraction of Inspiration O₂(FiO₂). Monitor the patient’s oxygenation status, assess ventilatory function to avoid hypoxemia, hypercapnia, or hypocapnia, and maintain physiologic breathing patterns.
Arterial blood gas (ABG)
Regular measurements of pH, PaO₂, PaCO₂, and lactate.
Anesthesia depth
The BIS monitors the depth of anesthesia, and the BIS is maintained at 40–60.
Surgical technique
Kidney transplantation was performed extraperitoneally in the right iliac fossa with end-to-side arterial/venous anastomoses and Lich‒Gregoir ureteroneocystostomy. Intraoperative complications (such as intraoperative hemorrhage, hypotensive state, hypoxemia, hypercapnia, and cardiac arrest), operation time, and postoperative anesthesia recovery time were recorded for both groups.
Postoperative assessments
(1) Pain assessment Visual Analog Scale (VAS) [24] is used to quantify the degree of postoperative pain, guide the use of analgesic drugs and optimize pain management.
(2) Airway complications: airway-related complications such as sore throat, hoarseness, or hemoptysis in postoperative patients.
(3) Graft function and Non-airway complications: Record Serum creatinine (Scr) and estimated glomerular filtration rate (eGFR, Cockcroft-Gault) [25], and non-airway complication (e.g. delayed graft function [DGF], acute rejection, infection).
Follow-up
Graft function (Scr, eGFR) and complications (e.g., acute rejection, infections, cardiovascular events) were regularly monitored for 90 days of follow-up.
Statistical analysis
SPSS 22.0 was used for analyses. Normally distributed data (mean ± SD) were compared via t- tests; non-normally distributed data (median [IQR]) via Mann-Whitney U tests. Categorical variables (n [%]) were analyzed with χ² or Fisher’s exact tests. Two-sided p < 0.05 defined significance.
Results
Baseline characteristics
Groups were well matched (shown in Table 1). The mean BMI of the TA group was less than 24, the preoperative cardiac function was good, and the left ventricular ejection fraction (LVEF) was greater than 50% of all patients. In the donor category, there were 2 living donors in the TA group, 1 living donor in the ETT group, and the rest were deceased donors. There were 15 deceased donors in both groups, all of whom donated DBDs (Donors of Brain Death). In both groups, donors and recipients were fully matched for both ABO and Rh blood types. All patients who tested positive for panel reactive antibodies (PRA) were weakly positive, and during HLA matching, sensitized epitopes were intentionally avoided. Consequently, none of the patients required preoperative desensitization therapy. The immune induction strategy of both groups was antithymocyte globulin (ATG) and methylprednisolone (MP) or basiliximab and MP. The postoperative immune maintenance strategy for both groups was the classic calcineurin inhibitor + mycophenolate mofetil + prednisolone (CNI + MMF + PRED) triple regimen [26].
Table 1. Baseline characteristics in both groupsTA(N = 26)ETT(N = 26) P Gender (N) 0.061 Female10(38.5%)4(15.4%) Male16(61.5%)22(84.6%)Age (Years, M ± SD)42.3 ± 12.341.2 ± 9.9 0.738 BMI(Kg/m^2^, M ± SD)22.1 ± 3.623.0 ± 3.5 0.475 EF value(%, M ± SD)67.5 ± 6.565.2 ± 6.4 0.212 Blood type (N) 0.394 A6(23.1%)11(42.3%) B5(19.2%)3(11.5%) O10(38.5%)6(23.1%) AB5(19.2%)6(23.1%)Donor Type (N) 1.000 Living donor2(11.8%)1(6.3%) Deceased donor15(88.2%)15(93.8%)Donor gender (N) 0.915 Female4(23.5%)5(31.3%) Male13(76.5%)11(68.8%)Donor Age (Years, M ± SD)41.2 ± 14.140.9 ± 15.1 0.963 Donor cause of death(N) 0.417 Cerebrovascular accident8(53.3%)4(26.7%) Brain trauma6(40.0%)9(60.0%) Hypoxic-ischemic encephalopathy1(6.7%)2(13.3%)PRA(N) 0.193 Negative21(80.8%)25(96.2%) Positive5(19.2%)1(3.8%)HLA mismatch (N, M ± SD)4.0 ± 1.44.0 ± 1.1 0.874 Immune induction strategy (N) 0.165 ATG + MP16(61.5%)11(42.3%) Basiliximab + MP10(38.5%)15(57.7%)Immune maintenance strategy (N) 1.000 Tac + MMF/MPS + Pred23(88.5%)22(84.6%) CsA + MMF/MPS + Pred3(11.5%)4(15.4%)Warm ischemia time (min, M ± SD)0.4 ± 1.51.1 ± 3.1 0.567 Cold ischemia time (hour, M ± SD)6.3 ± 5.16.9 ± 5.7 0.389 (This table is referenced in line 152 of the text)*****BMI Body Mass Index, EF value Ejection Fraction valu, PRA Panel reactive antibodie, ATG Anti-thymocyte Globulin, MP Methylprednisolon, Tac Tacrolimus,MMF/MPS Mycophenolate Mofetil/Mycophenolic Acid Sodium, CsA Cyclosporine A, Pred Prednisone
Intraoperative outcomes
Kidney transplantation was successfully completed in both groups, and there were no cases of intraoperative conversion to endotracheal intubation in the TA group. TA reduced cisatracurium use by 51.7% (12.6 ± 10.3 vs. 26.1 ± 6.8 mg, p < 0.05) and sufentanil use by 22.3% (22.3 ± 11.2 vs. 28.7 ± 8.7 µg, p < 0.05). However, there were no significant differences in the operative time (211.5 ± 45.7 min vs. 200.8 ± 35.5 min, p > 0.05) or anesthesia time (296.6 ± 57.4 min vs. 292.7 ± 48.8 min, p > 0.05).
Intraoperative monitoring revealed that the vital signs of the patients in both groups were generally stable, and no serious complications, such as arrhythmia, hypoxemia, or hypercapnia, occurred. Vasopressor requirements tended to be lower in TA group (14 vs. 19 patients; Table 2), and only 1 patient needed to use two vasoactive drugs in combination (4 patients in the ETT group). The dosage of dopamine, the most commonly used drug, tended to decrease in the TA group, but p > 0.05 (Table 2; Fig. 1C/D). The incidence of intraoperative complications in both groups was 1 case (Table 2). In the TA group, one patient required emergency intervention due to graft subcapsular hemorrhage. And one patient in the TA group versus two in the ETT group were transfused for low hemoglobin on intraoperative blood gas analysis. Each received < 2 units. Transfusion rates did not differ significantly (p > 0.05). The patient’s vital signs were stable after surgery, but DGF occurred. In the ETT group, one patient experienced persistent hypotension (the lowest systolic blood pressure was 60 mmHg, which lasted for 15 min), and DGF also occurred postoperation. The postoperative anesthesia recovery time in the TA group was significantly shorter than that in the ETT group (18.5 ± 10.8 min vs. 34.4 ± 14.7 min, p < 0.05) (Table 2; Fig. 1E), but there was no significant difference in the postoperative pain score (VAS score) (Table 2; Fig. 1F).
Table 2. Intraoperative data and postoperative recovery data for both groupsTA(N = 26)ETT(N = 26) P Operative Time (min, M ± SD)211.5 ± 45.7200.8 ± 35.5 0.949 Anesthesia Time (min, M ± SD)296.6 ± 57.4292.7 ± 48.8 0.628 Blood Loss (mL, M ± SD)109.6 ± 133.772.7 ± 34.1 0.529 Urine Output (mL, M ± SD)236.5 ± 313.8224.1 ± 229.7 0.507 Anesthetic Drug UsageMuscle RelaxantCisatracurium (mg, M ± SD)12.6 ± 10.326.1 ± 6.8 0.000 Analgesics Remifentanil (mg, M ± SD)1460.4 ± 704.81365.6 ± 572.5 0.647 Sufentanil (mg, M ± SD)22.3 ± 11.228.7 ± 8.7 0.007 Sedatives Midazolam (mg, M ± SD)3.1 ± 1.32.8 ± 0.6 1.000 Dexmedetomidine (mg, M ± SD)87.2 ± 45.880.9 ± 39.8 0.597 Types of Vasoactive Drugs(N) 0.211 None12(46.2%)7(26.9%) One Type13(50%)15(57.7%) Two Types1(3.8%)4(15.4%)Dosage of Vasoactive DrugsDopamine (µg, M ± SD)34347.7 ± 18941.448785.5 ± 25196.9 0.093 #Intraoperative Complications(N)1(3.9%)1(3.9%)Postoperative Anesthesia Recovery Time (min, M ± SD)18.5 ± 10.834.4 ± 14.7 0.000 Postoperative Pain Score (VAS Score)3.3 ± 1.02.8 ± 0.9 0.066 DGF4(15.4%)3(11.5%) 1.000 Postoperative Complications(N) Airway Complications2(7.7%)7(26.9%) 0.143 Non airway Complications7(26.9%)10(38.5%) 0.375 Renal functionSerum Creation(umol/L, M ± SD)Preoperation860.8 ± 299.51091.5 ± 283.6 0.008 POD7267.8 ± 203.4245.0 ± 240.8 0.516 POD30132.6 ± 59.4158.4 ± 90.5 0.194 POD90105.6 ± 24.3142.6 ± 44.4 0.015 Estimated Glomerular Filtration Rat(Cockcroft-Gault, ml/min/1.73 m², M ± SD)Preoperation6.4 ± 2.15.1 ± 1.9 0.014 POD743.0 ± 35.246.0 ± 25.8 0.462 POD3059.5 ± 25.253.5 ± 22.2 0.378 POD9066.6 ± 14.655.6 ± 21.5 0.056 Rejection (within three months) 0.235 No rejection26(100%)23(88.5%) Acute rejection0(0)3(11.5%)Blood transfusion 1.000 None25(96.2%)24(92.3%) Yes1(3.8%)2(7.7%)(This table is referenced in line 174–199/229 of the text)*** **VAS Score Visual Analogue Scale Score, DGF Delayed Graft Function, POD Post Operative Day# Intraoperative Complications: TA group: Subcapsular hemorrhage in the transplanted kidney; ETT group: Intraoperative hypotension
Fig. 1. Drug use during intraoperative anesthesia and perioperative parameters.A The usage of intraoperative muscle relaxant drugs (cisatracurium) in the TA group decreased significantly (12.63 ± 10.34 mg vs. 26.14 ± 6.84 mg, p < 0.05). B The TA group also showed a significant reduction in the intraoperative dosage of the potent opioid analgesic sufentanil (22.31 ± 11.16 mg vs. 28.65 ± 8.67 mg, p < 0.05). C and D Both groups maintained stable blood pressure during the operation, the blood pressure fluctuations in the TA group were more straight and intraoperative dopamine dosage tended to decrease, but the difference was not statistically significant (P>0.05). E The postoperative anesthesia recovery time in the TA group was significantly shorter than ETT group (18.54 ± 10.75 min vs. 34.35 ± 14.69 min, p < 0.05). **F **There was no statistical difference in postoperative pain scores(VAS score) between the two groups(P>0.05)
Postoperative outcomes
DGF incidence was similar between the two groups (TA: 15.4% vs. ETT: 11.5%, p > 0.05) (Table 2), and recovery of renal function was observed in all DGF recipients. Postoperative follow-up at 7, 30, and 90 days revealed a gradual improvement in renal function, as indicated by serum creatinine levels and eGFRs in both groups. However, no significant differences were observed between groups except for serum creatine at 90 days (Table 2; Fig. 2A). At 90 days, serum creatine concentration was 105.6 ± 24.3 µmol/L in the TA group, which was significantly lower than that in the ETT group (142.6 ± 44.4 µmol/L, p < 0.05). The mean eGFR of the TA group at 90 days was also 11.04 mL/min higher than that of the ETT group (p > 0.05). No acute rejection occurred in the TA group versus 3 cases in the ETT group within 3 months and the difference was not statistically significant (p > 0.05). In addition, the overall perioperative and follow-up complication rates were similar in both groups (Table 2). The incidence of perioperative airway-related complications in the TA group was 2 (7.7%), which was lower than 7 (26.9%) that in the ETT group. The incidence rates of postoperative non-airway complications were 7 (26.9%) and 10 (38.5%), respectively, with no significant difference (p > 0.05).
Fig. 2. Transplant kidney function and postoperative complications during perioperative and 90-d postoperative follow-up.A The renal function of the transplanted kidneys (serum creatinine and estimated glomerular filtration rate [eGFR]) in both groups showed a gradual improvement trend after surgery, except for the blood creatinine value at pod90, there was no significant difference between the two groups for other parameters. B The postoperative complication rates during the perioperative period and follow-up were similar in both groups. The incidence of perioperative airway-related complications in the TA group was 2 cases (7.7%), which was lower than 7 cases (26.9%) in the ETT group. The incidence of postoperative non-airway complications was 7 cases (26.9%) and 10 cases (38.5%) respectively. No statistical difference was observed in both complications (p > 0.05)
Discussion
By minimizing airway trauma, reducing perioperative stress, and accelerating recovery, TA aligns with enhanced recovery after surgery (ERAS) protocols, offering tangible improvements in postoperative comfort and quality of life [18, 26]. The integration of the concept of tubeless surgery into renal transplantation represents both a technical innovation and a paradigm shift toward patient-centered treatment. Moreover, these advantages may have a positive impact on the long-term function of the transplanted kidney and the quality of life of patients, providing a new direction for the development of renal transplant surgery. Guided by the tubeless surgical concept, TA represents the initial step undertaken by our center toward achieving tubeless kidney transplantation (TKT), with preliminary clinical results demonstrating promising advantages. The advantages are multifaceted, encompassing both intraoperative and postoperative benefits.
Cisatracurium, a widely utilized muscle relaxant in clinical practice, results in reduced clearance in patients with ESRD [11], consequently increasing the risk of postoperative residual neuromuscular blockade [27–29] and prolonging anesthesia recovery time. Compared with the ETT group, the implementation of the tubeless anesthesia protocol achieved a 51.7% reduction in the average intraoperative cisatracurium dosage while maintaining satisfactory intraoperative neuromuscular blockade. Notably, no intergroup difference was observed in surgical duration. Postoperatively, the TA group demonstrated a 46.0% reduction in average anesthesia recovery time, accompanied by accelerated restoration of consciousness and orientation. Fenta nil, another commonly employed anesthetic agent, belongs to the class of potent opioid analgesics. Although primarily metabolized by the liver, cumulative dosing carries inherent risks of adverse effects, including respiratory depression, bradycardia, and hypotension [30, 31], which may compromise graft perfusion. TA protocol implementation resulted in a 22.3% reduction in intraoperative sufentanil consumption, enhanced hemodynamic stability [32], and reduced reliance on vasoactive agents (shown in Table 2). Notably, postoperative pain assessment via the VAS demonstrated no statistically significant differences in pain scores between the groups.
During surgery, patients in the TA group were managed with a laryngeal mask airway (LMA) instead of endotracheal intubation, avoiding invasive endotracheal injury and hemodynamic fluctuations associated with intubation stimuli. Compared with the ETT group, the TA group demonstrated effective ventilation, more stable circulatory parameters [33], and a reduced need for vasoactive agents, with no serious intraoperative complications observed. Postoperatively, patients reported improved comfort, with fewer endotracheal intubation-related complications, such as sore throat and hoarseness. These benefits facilitate early oral intake and ambulation, effectively accelerating gastrointestinal recovery and preventing deep vein thrombosis, thereby promoting overall postoperative recovery.
Notably, at the postoperative follow-up, the blood creatinine level in the TA group was significantly better than that in the ETT group at 90 days, indicating a potential advantage in improving the long-term eGFR. The TA technique may have a beneficial effect on the long-term prognosis of transplanted kidneys by optimizing perioperative management. The implementation of TA eliminates the use of inhalation anesthetics, substantially reduces the dosages of muscle relaxants and analgesics, and maintains greater intraoperative hemodynamic stability. Consequently, it minimizes the nephrotoxic effects of anesthetic agents on the transplanted kidney [34], resulting in significantly enhanced renal function at 90 days postoperation. However, as this study is retrospective, further validation through multicenter randomized controlled trials is warranted.
A series of issues are also faced during the execution of this study that need to be continuously refined and improved. First, the inclusion and exclusion criteria for TA kidney transplantation need to be optimized. The current inclusion criteria were adapted from thoracic surgery^[15]^, but renal transplantation is an abdominal surgery, which generally does not directly affect the function of thoracic organs. Renal transplantation patients who have received renal replacement therapy for a long period before surgery often have comorbidities such as hypertension, coronary artery disease, diabetes mellitus, and other underlying diseases. Therefore, successful application of the TA requires a multidisciplinary collaborative mechanism. Second, the effectiveness of TA depends on anesthetic expertise and team coordination, given that technical challenges such as respiratory depression, difficult airway management, and precise control of anesthetic depth all require close surgeon‒anesthesiologist collaboration and a high level of professional competence. Third, the safe implementation of TAs relies on the availability of advanced monitoring systems and emergency equipment to provide the necessary technical support.
Conclusions
The successful application of the TA technique in renal transplantation based on the tubeless surgery concept not only accelerates patient recovery and saves medical resources but also may have a positive effect on the long-term prognosis of renal transplant recipients. Moreover, the implementation of TA technology is a systems project that requires the establishment of standardized operating procedures and a multidisciplinary consensus mechanism at the hospital level to ensure the stability of the technology and the safety of the patients. In the future, preserving spontaneous breathing via the TA may reduce the degree of lung injury caused by mechanical ventilation [35] and further reduce the dosage of muscle relaxants and anesthetic drugs to achieve greater benefits for kidney transplant patients. Therefore, TA technology still needs to be continuously optimized and improved to promote its wide application in renal transplantation.
This study is a single-center, retrospective case‒control study with a short follow-up period and a lack of blinding, which may limit the generalizability of the findings. Therefore, the results should be interpreted with caution. Further large-scale, multicenter, prospective randomized controlled trials with longer follow-up periods are needed to validate these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nawabi A, Sullivan P, De Ruyter M, Pichoff A, King CD, Nawabi P. Surgical approach for kidney transplantation under spinal anesthesia. J Surg Case Rep. 2020 Dec 31;2020(12):rjaa 538.10.1093/jscr/rjaa 538PMC 777836133425319 · doi ↗ · pubmed ↗
- 2Li J, Liu J, Hamblin L, Liu H, Liang L, Dong Q, et al. Simple to simplest: the tubeless technique. J Thorac Dis. 2017 Feb;9(2):222–4.10.21037/jtd.2017.02.55PMC 533407928275463 · doi ↗ · pubmed ↗
- 3He J, Liu J, Zhu C, Dai T, Cai K, Zhang Z et al. Expert consensus on tubeless video-assisted thoracoscopic surgery (Gua ngzhou). J Thorac Dis. 11(10):4101–8.10.21037/jtd.2019.10.04PMC 683799131737292 · doi ↗ · pubmed ↗
- 4Ekberg H, Tedesco-Silva H, Demirbas A, Vítko S, Nashan B, Gürkan A, et al. Reduced exposure to calcineurin inhibitors in renal transplantation. N Engl J Med. 2007 Dec 20;357(25):2562–75.10.1056/NEJ Moa 06741118094377 · doi ↗ · pubmed ↗
- 5Della Rocca G, Pompei L, Coccia C, Costa MG, Cecchini V, Vilardi V, et al. Atracurium, cisatracurium, vecuronium and rocuronium in patients with renal failure. Minerva Anestesiol. 2003;69(7–8):605–11, 612, 5.14564242 · pubmed ↗
- 6Craig RG, Hunter JM. Neuromuscular blocking drugs and their antagonists in patients with or Gan disease. Anaesth. 64 Suppl 1:55–65.10.1111/j.1365-2044.2008.05871.x 19222432 · doi ↗ · pubmed ↗
- 7Khuenl-Brady KS, Pomaroli A, Pühringer F, Mitterschiffthaler G, Koller J. The use of Rocuronium (ORG 9426) in patients with chronic renal Failur e. Anaesthesia. 48(10):873–5.10.1111/j.1365-2044.1993.tb 07417.x 8238829 · doi ↗ · pubmed ↗
- 8Silva PL, Ball L, Rocco PRM, Pelosi P. Physiological and Pathophysiological Consequences of Mechanical Ventilation. Semin Respir Crit Care Med. 2022 Jun;43(3):321–34.10.1055/s-0042-174444735439832 · doi ↗ · pubmed ↗