Understanding Oral Lichen Planus and Its Malignant Potential in the Saudi Arabian Population: A Systematic Review
Ali Alqarni, Shaimaa M. Alarabi, Muhannad A. Alamri, Abdullah A. Alzamil, Ibrahim A. Alhebshi, Murayziq A. Algethami, Khalid Aljohani, / Khlood A. Alkurdi, Abdullah F. Alshammari

TL;DR
This review examines oral lichen planus in Saudi Arabia, focusing on its prevalence, clinical features, and cancer risk.
Contribution
The study provides a systematic review of OLP in the Saudi Arabian population, highlighting gaps in diagnosis and malignant transformation rates.
Findings
OLP prevalence in Saudi Arabia ranges from 0.35% to 11.08%.
Dysplastic changes were observed in up to 12% of cases.
Malignant transformation rates ranged from 0.2% to 5.6%.
Abstract
Oral lichen planus (OLP) is a chronic inflammatory disorder recognised as a potentially malignant disorder of the oral cavity. This review aimed to synthesize available evidence from Saudi Arabia regarding OLP prevalence, clinical presentation, associated factors, and risk of malignant transformation. A systematic search was conducted across several electronic databases (e.g., PubMed, Scopus, Saudi Digital Library) up to February 2024. Eligible studies were original clinical investigations on OLP in Saudi Arabia, reporting at least one of the following: prevalence, clinical presentation, treatment, or malignant transformation. Study quality was appraised using the Joanna Briggs Institute (JBI) checklists. Eleven studies — eight cross-sectional and three case–control — met the inclusion criteria. Reported prevalence of OLP across Saudi Arabian populations ranged from 0.35% to 11.08%.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
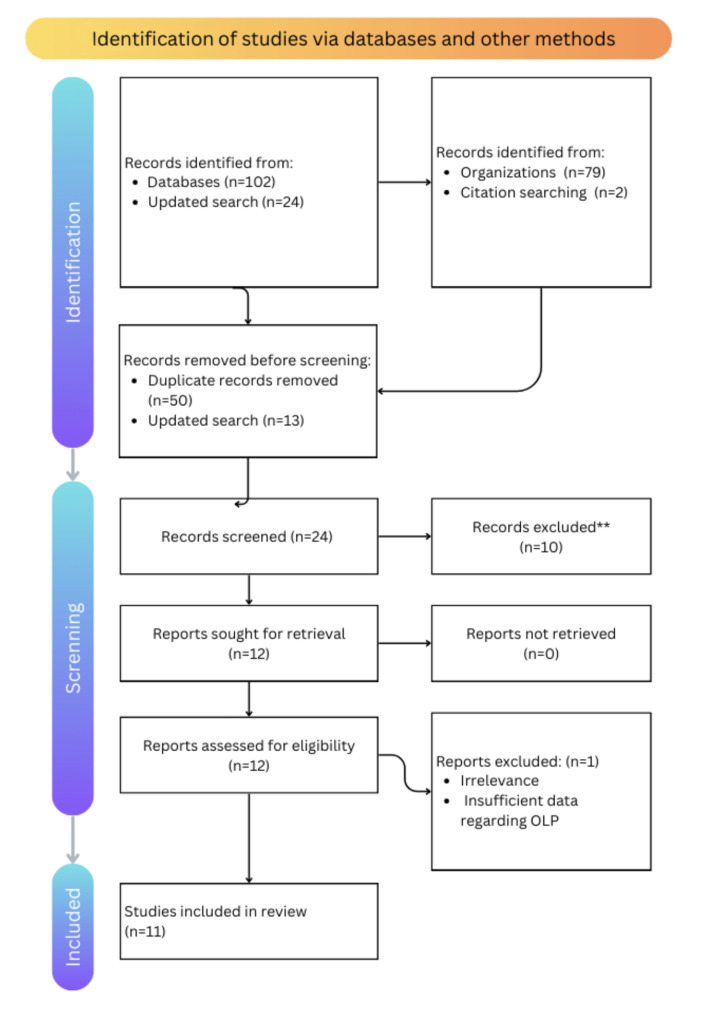 Fig 1
Fig 1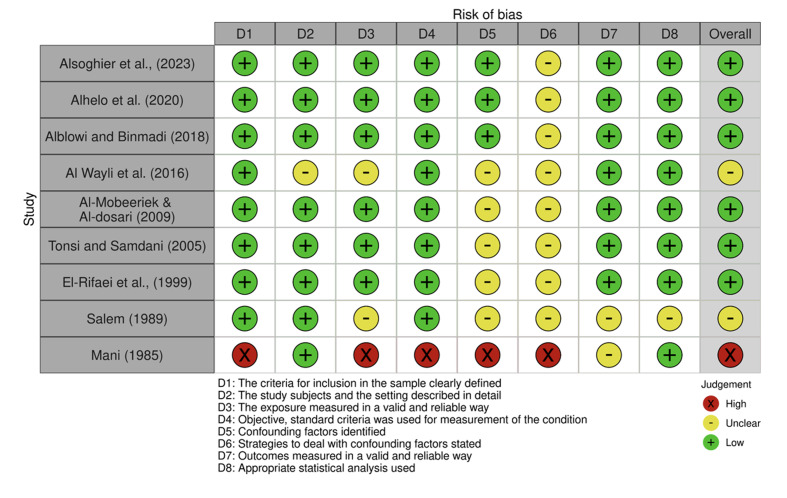 Fig 2
Fig 2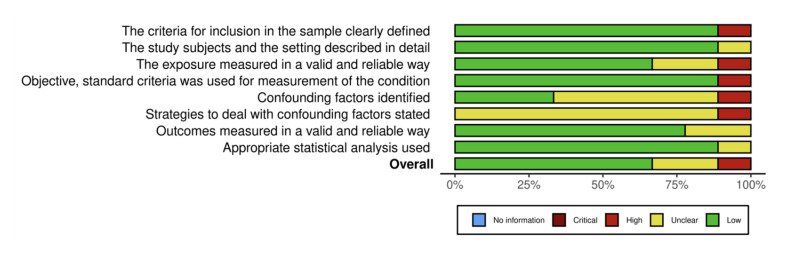 Fig 3
Fig 3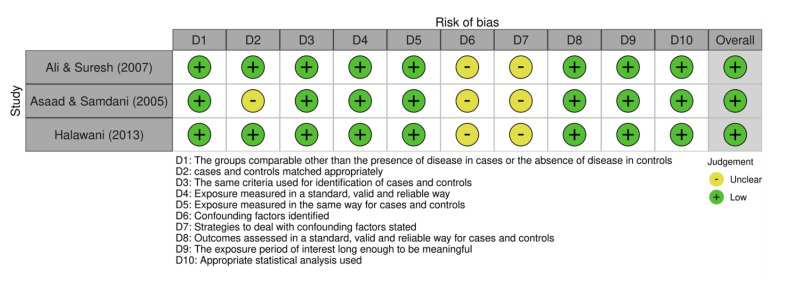 Fig 4
Fig 4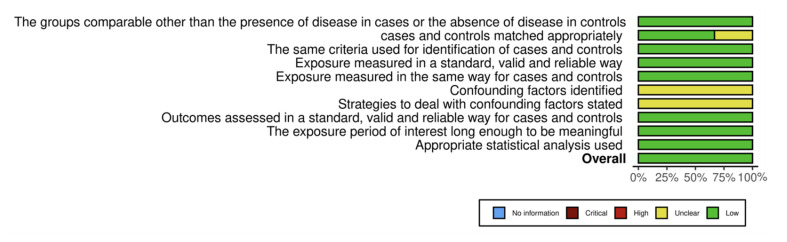 Fig 5
Fig 5|
Author (year) |
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Q7 |
Q8 |
Total (/8) |
|---|---|---|---|---|---|---|---|---|---|
|
*JBI crosssectional study criteria: Q1: Inclusion criteria defined; Q2: Subjects and setting described; Q3: Exposure measured validly; Q4: Objective criteria used; Q5: Confounding factors identified; Q6: Confounders addressed; Q7: Outcomes measured validly; Q8: Appropriate statistical analysis. | |||||||||
|
Alsoghier et al (2023) |
Yes |
Yes |
Yes |
Yes |
Yes |
Unclear |
Yes |
Yes |
7.5 |
|
Alhelo et al (2020) |
Yes |
Yes |
Yes |
Yes |
Yes |
Unclear |
Yes |
Yes |
7.5 |
|
Alblowi and Binmadi (2018) |
Yes |
Yes |
Yes |
Yes |
Yes |
Unclear |
Yes |
Yes |
7.5 |
|
Al Wayli et al (2016) |
Yes |
Unclear |
Unclear |
Yes |
Unclear |
Unclear |
Yes |
Yes |
6.0 |
|
AlMobeeriek and Aldosari (2009) |
Yes |
Yes |
Yes |
Yes |
Unclear |
Unclear |
Yes |
Yes |
7.0 |
|
Tonsi and Samdani (2005) |
Yes |
Yes |
Yes |
Yes |
Unclear |
Unclear |
Yes |
Yes |
7.0 |
|
ElRifaei et al (1999) |
Yes |
Yes |
Yes |
Yes |
Unclear |
Unclear |
Yes |
Yes |
7.0 |
|
Salem (1989) |
Yes |
Yes |
Unclear |
Yes |
Unclear |
Unclear |
Unclear |
Unclear |
5.5 |
|
Mani (1985) |
No |
Yes |
No |
No |
No |
No |
Unclear |
Yes |
2.5 |
|
Author (year) |
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Q7 |
Q8 |
Q9 |
Q10 |
Total (/10) |
|
*JBI case–control study criteria: Q1: Groups comparable; Q2: Appropriate matching; Q3: Same criteria for cases/controls; Q4: Exposure measured validly; Q5: Same method for cases and controls; Q6: Confounders identified; Q7: Confounders addressed; Q8: Outcomes assessed validly; Q9: Exposure period adequate; Q10: Appropriate statistical analysis. | |||||||||||
|
Ali and Suresh (2007) |
Yes |
Yes |
Yes |
Yes |
Yes |
Unclear |
Unclear |
Yes |
Yes |
Yes |
9.0 |
|
Halawani (2013) |
Yes |
Yes |
Yes |
Yes |
Yes |
Unclear |
Unclear |
Yes |
Yes |
Yes |
9.0 |
|
Author year |
n patients |
Mean age in years ± SD |
F:M ratio |
Prevalence OLP |
Systemic disease comorbidities |
Clinical types |
Sites involved |
Treatments |
Improvement (%) |
Malignant transformation (%) |
|---|---|---|---|---|---|---|---|---|---|---|
|
NR = not reported; DM = diabetes mellitus; HTN = hypertension; HBV/HCV = hepatitis B/C virus. | ||||||||||
|
Alsoghier 2023 |
140 |
47 ± 13 |
4:3 |
Not stated |
Diabetes common (40% ≥ 1 condition) |
Not stated |
Buccal mucosa (52%) |
Not stated |
Not stated |
12% dysplasia |
|
Alhelo 2020 |
50 |
48 |
2.5:1 |
N/A |
Multiple incl. DM (30%), HTN, HCV |
Reticular (98%), erythematous (66%), ulcerative |
Buccal (90%), tongue (50%), gingiva, lips, palate |
Topical corticosteroids, systemic + topical, reassurance |
68% |
NR |
|
Alblowi and Binmadi 2018 |
4/1248 |
47.5 ± 13.5 |
1:1 |
0.3% |
NR |
NR |
NR |
NR |
NR |
NR |
|
Al Wayli 2016 |
42 |
24–63 |
Female only |
0.8% |
NR |
Reticular most common |
Buccal mucosa |
NR |
NR |
NR |
|
Halawani 2013 |
47 |
49 ± 12.8 |
39:8 |
44.7% OLP in LP |
HCV infection |
NR |
NR |
NR |
NR |
NR |
|
AlMobeeriek and Aldosari 2009 |
9 |
38.2 |
1.36:1 |
0.3% |
NR |
Reticular (98%), erosive (66%), plaquelike (8%) |
Buccal (80%), tongue (38%) |
NR |
NR |
NR |
|
Ali and Suresh 2007 |
80 |
43.4 |
1:3 |
NR |
DM: 35% study vs 15% control |
Reticular, erosive, atrophic, vesicular, multiple |
Buccal most common |
NR |
NR |
NR |
|
Tonsi and Samdani 2005 |
12/114 |
40.7 |
0.9:1 |
10.5% |
HCV 10.5% vs 4.6% control |
NR |
NR |
NR |
NR |
NR |
|
ElRifaei 1999 |
34 |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
NR |
|
Salem 1989 |
72/4277 |
49 |
0.8:1 |
1.7% |
DM (30%), heart disease, CKD, HBV |
Reticular, plaque, atrophic, erosive |
Buccal (86%), gingiva, tongue, palate, lips |
Topical steroid + anaesthetic |
NR |
5.6% |
|
Mani 1985 |
4/674 |
NR |
0.76:1 |
0.6% |
None |
NR |
NR |
NR |
NR |
0.2% |
|
Author (year) |
Study aim |
Study design |
Location |
Period |
Sample size |
Sampling method |
|---|---|---|---|---|---|---|
|
Alsoghier et al (2023) |
Assess demographics and clinicohistological characteristics of OLP and dysplasia relevance |
Cross-sectional retrospective |
King Saud University, Riyadh |
Sept. 2022 – Sept. 2023 |
140 |
Convenience sampling of available records |
|
Alhelo et al (2020) |
Describe epidemiology and clinicopathology of OLP |
Cross-sectional retrospective |
King Abdulaziz University Dental Hospital (KAUDH), Jeddah |
June 2012 – June 2018 |
50 OLP patients from 10,000 dental patients |
Convenience sampling from oral medicine referrals |
|
Alblowi and Binmadi (2018) |
Frequency and distribution of gingival lesions biopsied (19962016) |
Cross-sectional retrospective |
KAUDH Oral Pathology Lab, Jeddah |
1996 – 2016 |
1,248 oralmaxillofacial lesions (119 gingival) |
Possibly convenience sampling of all biopsy submissions |
|
Al Wayli et al. (2016) |
Prevalence and distribution of oral mucosal lesions among Saudi female patients |
Cross-sectional |
AlYamamah Hospital, Riyadh |
2005 – 2010 |
5,543 females (379 lesions; 42 OLP) |
Consecutive clinical attendees |
|
Halawani (2013) |
Prevalence of anti-HCV antibodies and genotypes in LP patients |
Case–control |
King Khalid University Hospital, Riyadh |
2008 – 2010 |
47 (45 Saudis) |
Convenience sampling of LP patients and controls |
|
AlMobeeriek and Aldosari (2009) |
Type and extent of oral lesions |
Cross-sectional |
College of Dentistry, Riyadh |
~2006 – 2009 |
2,552 outpatients (383 lesions; 9 OLP) |
Consecutive attendees |
|
Ali and Suresh (2007) |
Relationship between OLP, transaminase, and HCV |
Case–control |
King Faisal University, Dammam |
2006 – 2007 (est.) |
80 confirmed OLP |
Not specified |
|
Tonsi and Samdani (2005) |
AntiHCV antibodies and clinical LP |
Cross-sectional |
Alawi Tonsi Hospital, Makkah |
1999 – 2001 |
114 LP patients (12 OLP) |
Not specified |
|
ElRifaei (1999) |
HBV/HCV and aminotransferase in OLP |
Cross-sectional |
Dammam Central Hospital |
Not specified |
34 OLP patients; 32 controls |
Convenience sampling |
|
Salem (1989) |
OLP prevalence |
Cross-sectional |
King Fahd Central Hospital, Jizan |
1982 – 1987 |
4,277 patients (72 OLP) |
Likely consecutive attendees |
|
Mani (1985) |
Oral cancer and precancerous lesion prevalence |
Cross-sectional |
King Saud University, Riyadh |
Jan. – Dec. 1983 |
674 patients |
Consecutive first visits |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Head and Neck Cancer Studies · Oral and Maxillofacial Pathology
Oral lichen planus (OLP) is a chronic T-cell mediated inflammatory disease that predominantly affects mucous membranes, with the oral cavity being the most frequently involved site.^17,38 ^ First described by Wilson in 1868,^45^ OLP presents clinically as reticular, erosive, or atrophic lesions, often causing significant pain and impacting quality of life.^16,20,33,34 ^ Unlike its cutaneous counterpart, which is typically self-limiting, OLP persists chronically in most patients and has been classified by the World Health Organization as an oral potentially malignant disorder (OPMD) with a transformation risk ranging from 0.4% to 5.6%.^44^
The pathogenesis of OLP remains incompletely understood but involves a complex interplay of genetic, immunological, and environmental factors.^19,20,21,25,29,30 ^ Notably, associations with hepatitis C virus (HCV) infection have been reported globally, though with significant geographical variation.^4,31 ^ In Saudi Arabia, where HCV prevalence is estimated at 5.6%,^4^ this potential link warrants particular attention given its implications for screening and management.
Despite numerous epidemiological studies of OLP worldwide,^24,25,34,44 ^ data from Saudi Arabia remain limited and heterogeneous.^2,3,5,6,7,10,12,13,14,22,26,32,39,40,42 ^ Reported prevalence rates in Saudi Arabia vary dramatically from 0.35% to 11.08%,^3, 5,6,10,13,14,22,26,32,40,42^ likely reflecting differences in diagnostic criteria, study populations, and regional factors.^3,5,10,13,14,22, 32,40,42^ This variability underscores the need for a comprehensive synthesis of existing evidence to clarify disease patterns and guide clinical practice.
The current systematic review addresses three critical gaps:
By systematically evaluating available evidence, this study aims to provide clinicians and researchers with a clearer understanding of OLP’s epidemiology, clinical characteristics, and malignant potential in Saudi Arabia. The findings will inform both clinical decision-making and future research priorities in the region.
MATERIALS AND METHODS
A rigorous systematic approach was employed to identify and synthesize evidence on oral lichen planus (OLP) in the Saudi population. The review protocol was registered prospectively with PROSPERO (registration number: CRD42024567890) and adhered to PRISMA guidelines.^35^
Search Strategy and Data Sources
A comprehensive literature search was conducted across multiple electronic databases, including PubMed, Scopus, Web of Science, Cochrane Library, Saudi Digital Library, BMC Oral Health, and others. The search encompassed articles published up to February 2024 and utilized key terms related to OLP and Saudi Arabia, including “oral lichen planus,” “lichen planus,” “oral mucosal lesions,” and “Saudi Arabia.” Search restrictions included language (English and Arabic) and study type (clinical studies).
Study Selection and Eligibility Criteria
Studies were selected based on predefined inclusion and exclusion criteria. Eligible studies were original clinical investigations reporting on:
Prevalence, epidemiology, or incidence of OLP in Saudi ArabiaClinical and histopathological characteristicsRisk factors, including systemic comorbiditiesMalignant transformation or cancer risk.
Exclusion criteria encompassed case reports, reviews, and studies with fewer than 10 patients. Two independent reviewers conducted the study screening and selection, resolving disagreements by consensus or consultation with a third reviewer. Figure 1 illustrates the screening process.
The PRISMA flowchart showing the selection process of the articles retrieved from different online databases.
Data Extraction and Calibration
Data extraction was performed independently by two reviewers using a standardized data extraction form. Extracted items included study design, location, patient demographics, diagnostic criteria, clinical presentation, treatment modalities, and outcomes related to malignant transformation. Prior to full extraction, reviewers calibrated their approach by independently extracting data from a subset of studies to ensure consistency (Cohen’s Kappa: 0.89).
Quality Assessment and Risk of Bias
Each included study’s methodological quality was appraised using the Joanna Briggs Institute (JBI) checklists tailored for cross-sectional and case-control studies.^27^ Scoring assigned 1 point for “Yes,” 0 for “No,” and 0.5 for “Unclear.” Quality scores for included studies ranged from 2.5 to 7.7 for cross-sectional designs and 9 or 10 for case-control studies. Detailed results of quality assessment are presented in Tables 1 and 2. Risk of bias was also depicted graphically through traffic-light plots to visually highlight areas of concern, notably confounding factors (Figs 2 to 5).
Traffic-light plot of the risk of bias assessment for cross-sectional studies.
Summary plot for risk of bias assessment results for cross- sectional studies.
Traffic-light plot of the risk of bias assessment for case control studies.
Summary plot for risk of bias assessment results for case control studies.
Data Synthesis
Due to heterogeneity in study designs, diagnostic methodologies, and reported outcomes, a narrative synthesis approach was adopted. Where possible, subgroup analyses were performed based on diagnostic criteria (clinical vs histopathological), geographic region within Saudi Arabia, and study period (pre- and post-year 2000). Summarized clinical and epidemiological data were tabulated for comparison (Table 4).
RESULTS
Study Selection and Characteristics
The systematic search initially identified 126 records through a comprehensive search of multiple electronic databases including PubMed, Scopus, and the Saudi Digital Library. After removal of duplicates and application of inclusion and exclusion criteria, 11 studies met the eligibility criteria for detailed analysis (Fig 1). These comprised eight cross-sectional studies, predominantly retrospective in nature, and three case-control studies. The included studies spanned a wide period from 1985 to 2023 and were conducted across multiple regions of Saudi Arabia, including Riyadh, Jeddah, Makkah, Dammam, and Jizan, reflecting a reasonable geographical diversity, albeit with an urban and tertiary care center bias (Table 3).
Sample sizes of the studies varied substantially. The largest cohort included more than 5500 participants,^14^ mainly female, whereas the smallest case series reported 34 patients.^22^ Several studies sourced data from dental or dermatology clinics, with sampling predominantly based on convenience or consecutive patient attendance rather than random sampling.^3,5,10,13,32,40,42 ^ This introduces potential bias but reflects real-world clinical populations in Saudi Arabia.
Quality Assessment and Risk of Bias
The methodological quality of included studies was appraised using Joanna Briggs Institute checklists, tailored to study design differences (Tables 1 and 2). Most cross-sectional studies demonstrated moderate to high methodological rigor, with scores ranging from 5.5 to 7.7 out of 8. However, one older study^32^ scored significantly lower (2.5), indicating considerable risk of bias related to unclear inclusion criteria and inadequately described exposure measurements. Common limitations across the newer studies included unclear handling of confounding variables and insufficient description of participant recruitment, which may affect internal validity.
The two case-control studies^6,26 ^ were similarly robust, each scoring 9 out of 10, with minor concerns regarding confounding control strategies (Table 2). Risk-of-bias assessments visualized in traffic-light plots and summary figures further corroborated these findings, highlighting overall acceptable quality but identifying particular weaknesses in confounder mitigation and participant description (Figs 2 to 5).
Prevalence and Demographic Features of OLP
The prevalence of oral lichen planus reported in Saudi Arabia exhibited notable heterogeneity, ranging from as low as 0.3% in studies involving broad dental patient populations^3,10 ^ to as high as 11.1% within cohorts selectively enriched for lichen planus or hepatitis C virus (HCV) infection risk^26,42 ^ (Table 4). This disparity is linked in part to differences in study population characteristics, sampling methodologies, and diagnostic criteria—some studies relied purely on clinical diagnosis while others integrated histopathological confirmation.^3,5,6,10,13,14,22,26,32,40,42 ^
Age distributions across cohorts averaged in mid-to-late middle adulthood (approximately 38 to 49 years), consistent with international epidemiological patterns of OLP. Sex ratios mostly favored females, with female:male ratios generally ranging from 1.3:1 to 2.5:1, confirming the known higher incidence of OLP in women, although exceptions existed in HCV-focused studies,^5,26,42 ^ which showed a slight male predominance (Table 4).
Clinical Presentation and Diagnostic Approaches
Clinical features of OLP reported in these studies largely align with global observations. The reticular form was consistently the most common subtype, observed in up to 98% of cases,^5,10 ^ followed by erythematous and erosive variants. Lesion distribution predominantly involved the buccal mucosa, with secondary sites including the tongue, gingiva, lips, and palate—a pattern consistent with OLP’s typical anatomical predilection (Table 4).
Diagnostic approaches differed across studies. Several incorporated histopathological assessments to confirm OLP diagnoses and exclude mimicking conditions such as lichenoid drug reactions or autoimmune blistering disorders.^3,5 ^ Others relied on clinical criteria alone, which may increase diagnostic uncertainty. Notably, the application of contemporary diagnostic guidelines such as those from the American Academy of Oral and Maxillofacial Pathology was limited, although newer studies increasingly emphasized combined clinical and microscopic diagnosis for accuracy (Table 4).^13^ Notable symptoms were frequently pain or burning sensations, with symptomatic cases representing an estimated 54% to 68% of patients in some cohorts,^5^ underscoring the clinical relevance and impact on quality of life.
Associated Systemic Conditions
A wide range of systemic comorbidities were reported among OLP patients, with diabetes mellitus and hypertension being most common. Several studies also detailed a notable prevalence of thyroid disorders and hyperlipidemia among participants.^5,40 ^ Importantly, hepatitis C virus infection appeared frequently associated with OLP in Saudi cohorts. The seroprevalence of HCV among OLP patients in included case-control studies ranged from 10.5% to 44.7%, markedly higher than the national average prevalence of about 0.8%^6,26 ^ (Table 4). These findings highlight a probable etiological or associative link warranting routine HCV screening in OLP patients, especially in regions with higher endemicity. Other environmental or behavioral risk factors such as tobacco use, local dietary habits, or exposure to allergens and dental materials were insufficiently explored, marking an area for further investigation.
Management and Response to Treatment
Treatment modalities for OLP across Saudi studies varied. The most frequent therapeutic approach involved topical corticosteroids, employed either alone or in combination with systemic steroids or other immunomodulatory agents.^5,40 ^ Supportive measures, including patient education and reassurance, were also common.
Clinical response rates to treatments were generally moderate. For instance, Alhelo et al^5^ observed clinical improvement in approximately 68% of treated patients, while a substantial proportion remained refractory or experienced no significant symptom relief. However, patient adherence and follow-up rates were often inadequate, with up to 34% of patients refusing or discontinuing treatment, reflecting gaps in patient engagement or potential lack of standardized care pathways.
Malignant Transformation and Dysplasia Prevalence
Malignant transformation rates of OLP among Saudi patients fell within the expected global range but exhibited variability, reported between 0.2% and 5.6%.^32,40 ^ Alsoghier et al^13^ reported the presence of epithelial dysplasia in up to 12% of cases based on histopathological assessment. These figures reinforce that OLP, particularly erosive and atrophic subtypes, carry a non-negligible risk of progression to oral squamous cell carcinoma.
Follow-up durations necessary to capture malignant progression were generally limited or absent in most studies, impeding robust risk stratification. Salem^40^ uniquely provided longitudinal data with a mean follow-up of approximately 3.5 years. The influence of confounders, notably tobacco use, systemic health status, and treatment regimens, was insufficiently adjusted for, again limiting conclusions regarding independent malignant risk.
Subgroup and Comparative Analyses
Analysis stratified by diagnostic methodology revealed that studies incorporating histopathological confirmation tended to report lower OLP prevalence rates (0.3% to 5.6%) relative to those relying solely on clinical diagnosis (up to 11.1%). This discrepancy reinforces the importance of standardized diagnosis for epidemiological precision. Geographically, higher prevalence and stronger HCV associations were observed in western regions (Jeddah, Makkah), areas known for higher hepatitis C endemicity, compared to relatively lower rates in central regions (Riyadh) (Table 4).
DISCUSSION
The present systematic narrative review synthesizes evidence from 11 clinical studies^3,5,6,10,13,14,22,26,32,40,42 ^ examining oral lichen planus (OLP) within the Saudi Arabian population. Three key findings emerge prominently: the wide variability in reported prevalence rates, a notable association between OLP and hepatitis C virus (HCV) infection, and the documented rates of malignant transformation.
Prevalence Variability and Diagnostic Challenges
The reported prevalence of OLP in Saudi Arabia spans a striking range—from as low as 0.3% to as high as 11.08%,^3,5,6,10,13,14,22,26,32,40,42 ^ which is considerably broader than global estimates, typically ranging from 1% to 1.5%.^24^ Such heterogeneity likely stems from several intertwined factors. First, variation in diagnostic criteria creates substantial inconsistency; some studies rely solely on clinical diagnosis, while others incorporate histopathological confirmation.^3,5,6,10,13,14,22,26,32,40,42 ^ Histopathologically confirmed cases tend to report lower prevalence compared to clinical-only diagnoses, potentially reflecting over-diagnosis or misclassification when strict tissue-based criteria are not applied.^18^ Second, study settings differ—population-based screening is limited, with most data derived from hospital-based or specialty clinic cohorts, often leading to selection bias toward symptomatic or referred cases.^13,40 ^ Third, geographic disparities within Saudi Arabia, emerging from distinct environmental exposures or genetic variations, may influence disease distribution; Western regions like Jeddah and Makkah show higher reported prevalence, possibly correlated with increased exposure to HCV or other region-specific risk factors.^8,9,26 ^ These findings underscore the urgent need for standardized diagnostic protocols adopting the internationally recognized histopathological and clinical criteria, aiming to unify case definitions and enable comparability across future Saudi studies.
Association of OLP and Hepatitis C Virus
A salient and recurrent theme in the reviewed literature is the elevated seroprevalence of HCV among OLP patients in Saudi studies relative to the general population’s baseline HCV rate.^4^ Specifically, seropositivity in OLP cohorts varies between 10.5% and 44.7%, significantly exceeding population norms.^5,26,42 ^ Mechanistically, HCV infection may provoke aberrant immune responses, including molecular mimicry or chronic antigenic stimulation, leading to the persistent T-cell mediated epithelial injury characteristic of OLP.^31^ The implications for clinical practice in Saudi Arabia are profound: routine HCV screening for patients presenting with OLP could facilitate early identification of viral comorbidity and allow tailored antiviral therapies that may influence OLP course and malignant potential. Nevertheless, the predominance of data from single-center studies cautions against overgeneralization; multicenter, prospective investigations are warranted to validate this association and unravel its clinical significance within diverse Saudi subpopulations. This also aligns with the global discourse identifying regional variation in the OLP-HCV nexus.^44^
Malignant Transformation Potential
Malignant transformation of OLP into oral squamous cell carcinoma remains a clinical concern, with rates globally reported between 0.4% and 5%.^23,44 ^ Within Saudi studies, observed transformation rates ranged from 0.2% to 5.6%, consistent with global figures but highlighting the necessity for cautious surveillance.^28,32,40,43 ^ Importantly, these rates derive primarily from retrospective studies with limited longitudinal follow-up, typically averaging around 3–5 years, a timeframe potentially insufficient to capture all cases of malignant progression.^40^ Furthermore, certain clinical subtypes—especially erosive and atrophic forms—demonstrate a predilection for dysplastic changes and transformation, though subtype-specific risk stratification remains underexplored in Saudi cohorts.^8,13 ^ Another complicating factor is the relative paucity of adjustment for confounding exposures such as tobacco and alcohol use, which independently increase oral cancer risk and may synergistically elevate transformation likelihood in OLP patients.^8,10, 15,35,37^ This insufficiency necessitates augmented prospective monitoring frameworks incorporating clinical, histopathological, and molecular parameters to refine risk prediction models and optimize patient management pathways.
Therapeutic Landscape and Patient Management
The therapeutic approaches across Saudi studies reveal a predominant reliance on topical corticosteroids, which remain the mainstay for symptom control in OLP.^5,41 ^ Nevertheless, variations in treatment regimens and patient adherence patterns introduce complexity to efficacy assessments. For instance, nearly half of the patients either do not commence treatment or discontinue follow-up, indicating gaps in patient education, motivation, or access.^5^ Notably, psychological comorbidities such as anxiety and depression, recognized internationally as exacerbating factors for pain perception and quality of life in OLP, remain under-addressed in Saudi clinical settings despite their likely relevance.^1^ Optimizing patient counseling, integrating psychosocial support, and standardized treatment protocols—including possibly antiviral therapy in HCV-positive cases—could improve adherence and clinical outcomes.^1^ A proposed management algorithm prioritizing initial HCV screening, histological diagnosis, corticosteroid therapy, structured follow-ups every 3–6 months for high-risk patients, and specialist referrals for dysplastic lesions or refractory disease is timely and warranted.
Study Strengths, Limitations, and Future Directions
This review represents the first comprehensive synthesis of OLP data specific to Saudi Arabia and benefits from rigorous methodological critique using standardized risk of bias tools. The inclusion of both cross-sectional and case-control studies provides a balanced perspective on prevalence, risk factors, and outcomes.^3,5,6,10,13,14,22,26,32,40,42 ^ Nevertheless, limitations permeate. The substantial heterogeneity across regions, diagnostic criteria, and study designs precluded formal meta-analysis and accentuated interpretative challenges. Additionally, rural and underserved populations remain largely unstudied, limiting generalizability. Finally, a lack of prospective longitudinal data restricts insight into disease progression and malignant transformation trajectories.
Future research should prioritize well-designed multicenter cohort studies employing validated diagnostic criteria and incorporating comprehensive assessments of systemic comorbidities, lifestyle exposures, and psychosocial factors. Molecular profiling, including cytokine expression, genetic polymorphisms, and viral-host interactions, holds promise for elucidating pathogenesis and refining personalized risk stratification. Additionally, the development of a national registry for OLP patients would facilitate robust surveillance, early detection of malignancy, and improved care coordination. Patient-reported outcomes and quality-of-life metrics should also be integrated into research and clinical practice to holistically address the burden of OLP within Saudi Arabia.
CONCLUSION
OLP in Saudi Arabia demonstrates considerable epidemiological diversity and is associated with significant comorbidity, including an elevated prevalence of HCV infection and a comparable risk of malignant transformation to global reports. The findings highlight the imperative for harmonized diagnostic criteria, routine HCV screening, and enhanced patient management frameworks. Moving forward, multicenter prospective research with longitudinal follow-up and integrated molecular and psychosocial assessments will be essential to optimize clinical outcomes and inform public health strategies targeting this chronic, potentially malignant oral condition within the Saudi context.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adamo D Calabria E Coppola N Lo Muzio L Giuliani M Bizzoca ME et al Psychological profile and unexpected pain in oral lichen planus: A case-control multicenter SIPMO study Oral Dis 202228239841410.1111/odi.1378733512068 · doi ↗ · pubmed ↗
- 2Al-Attas SA Ibrahim SS Amer HA Darwish ZE Hassan MH Prevalence of potentially malignant oral mucosal lesions among tobacco users in Jeddah, Saudi Arabia Asian Pac J Cancer Prev 20141527577622456849110.7314/apjcp.2014.15.2.757 · doi ↗ · pubmed ↗
- 3Alblowi J, Binmadi N. Histopathologic analysis of gingival lesions: A 20-year retrospective study at one academic center. J Clin Exp Dent 2018;10(6..10.4317/jced.54766 PMC 600508729930774 · doi ↗ · pubmed ↗
- 4Alhaydar N Abusaris R Alwatban N Prevalence and factors associated with hepatitis C virus in Riyadh, Saudi Arabia: a large cross-sectional study J Epidemiol Glob Health 2025151424007279510.1007/s 44197-025-00383-0PMC 11903971 · doi ↗ · pubmed ↗
- 5Alhelo A Almazrooa S Mansour G et al Characterization of oral lichen planus in a subset of patients Saudi J Oral Sci 202073199
- 6Ali AA Suresh CS Oral lichen planus in relation to transaminase levels and hepatitis C virus J Oral Pathol Med 200736106046081794475310.1111/j.1600-0714.2007.00581.x · doi ↗ · pubmed ↗
- 7Aljabab M. Evaluation of oral changes among tobacco users of Aljouf Province, Saudi Arabia. J Clin Diagn Res 2015;9(5):ZC 58–ZC 61.10.7860/JCDR/2015/13683.5950 PMC 448415626155564 · doi ↗ · pubmed ↗
- 8Aljohani K Alqarni A Harte M et al Oral potentially malignant disorders and oral cancer in Saudi Arabia: an epidemiological review J Clin Med 2024 Feb 28135137610.3390/jcm 13051376 PMC 1093232738592216 · doi ↗ · pubmed ↗