Intravenous Albumin for Oedema in Children With Nephrotic Syndrome: A Systematic Review and Mapping of the Evidence Landscape
Sohaib B Nawaz, Muhammad Ashfaq Zafar

TL;DR
This study reviews evidence on using intravenous albumin to treat oedema in children with nephrotic syndrome, finding limited data and suggesting more research is needed.
Contribution
The study provides a systematic review and evidence mapping focused specifically on children, highlighting gaps in current research.
Findings
Only one eligible RCT was found, showing transient short-term benefits of albumin plus furosemide.
Evidence mapping revealed many excluded studies with methodological issues or inappropriate populations.
Current evidence is insufficient to justify routine use of IV albumin in children with nephrotic syndrome.
Abstract
Nephrotic syndrome is a common glomerular disorder in childhood, often complicated by oedema, which contributes to morbidity, discomfort and prolonged hospitalisation. Intravenous (IV) albumin is frequently used with diuretics in children with resistant oedema, but its effectiveness and safety remain uncertain. Previous reviews are limited by adult populations, small sample sizes or a lack of quantitative synthesis. Our aim was to systematically evaluate the effectiveness and safety of IV albumin, with or without diuretics, versus no albumin in hospitalised children with nephrotic syndrome and oedema, and to map excluded-but-relevant studies to identify evidence gaps. We searched PubMed, Cochrane CENTRAL, Google Scholar and Europe PMC from January 1, 1990, to June 30, 2025, using MeSH terms and free-text keywords for nephrotic syndrome, albumin and paediatric populations. Reference…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
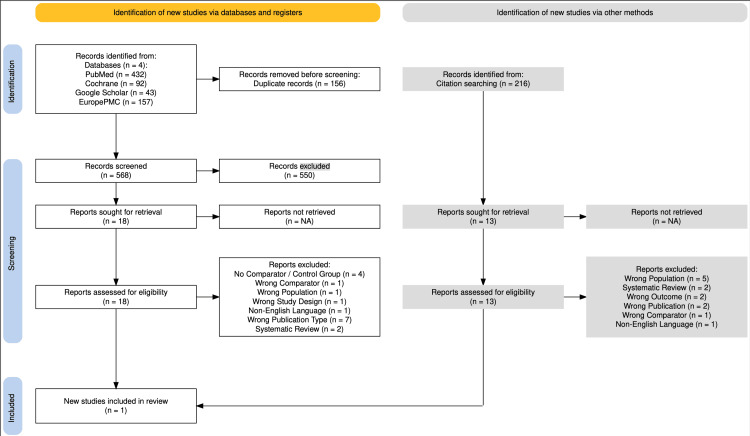 Figure 1
Figure 1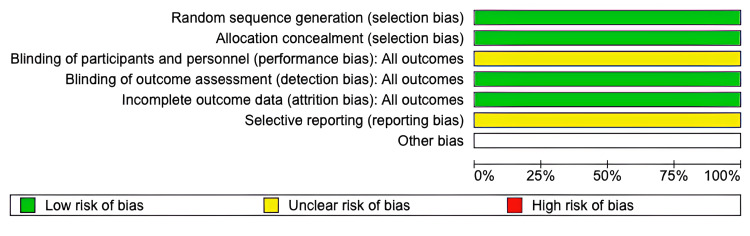 Figure 2
Figure 2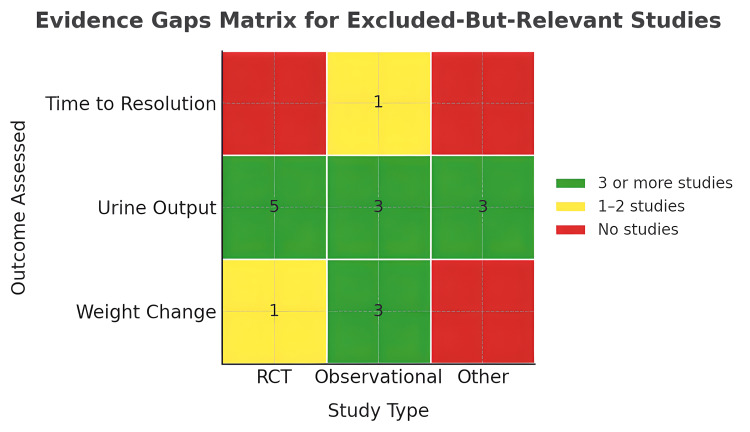 Figure 3
Figure 3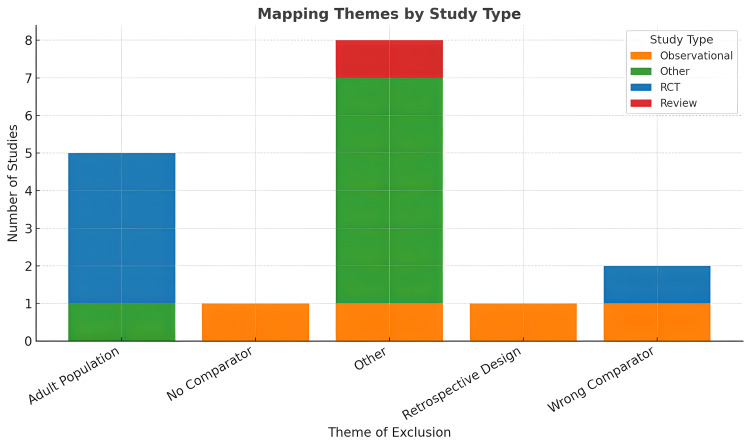 Figure 4
Figure 4| Criteria | Eligibility details |
| Population | Children aged 1-18 years with nephrotic syndrome and clinically evident oedema during hospitalisation. |
| Intervention | Intravenous albumin administered either alone or in combination with diuretics such as furosemide. |
| Comparator | Diuretics alone, placebo or supportive care without albumin. |
| Outcomes | Studies were eligible if they reported on at least one of the following: change in weight (primary), urine output (secondary), time to oedema resolution (secondary), length of hospital stay (secondary) or adverse events (primary). |
| Study Designs | We included RCTs, quasi-RCTs and comparative observational studies. |
| Timeframe | We screened studies reported from January 1, 1990, to June 30, 2025. |
| Studies meeting the following criteria were excluded from the review: |
| No comparator group (e.g., single-arm case series). |
| Studies where oedema is caused by conditions other than nephrotic syndrome, e.g., cirrhosis. |
| Studies where paediatric data is not separable from adults. |
| Studies on animal subjects. |
| Studies published in languages other than English. |
| Editorials, reviews, commentaries, case reports or case series without a comparator. |
| Reason for exclusion | Number of articles* |
| Wrong study design | 284 |
| Wrong intervention | 193 |
| Wrong outcome | 100 |
| Wrong population | 84 |
| Wrong publication type | 44 |
| Feature | Dharmaraj et al. (2009) [ |
| Country | India |
| Study design | Randomised crossover trial |
| Population | 16 children aged 3-18 years with nephrotic syndrome and persistent oedema despite diuretic therapy |
| Intervention | 20% human albumin infusion followed by furosemide, received by 14 patients |
| Comparator | Furosemide infusion alone, received by 13 patients |
| Primary outcomes | Change in urine output and urine sodium excretion |
| Secondary outcomes | Weight loss, change in urine osmolality, potassium and chloride excretion, osmolal clearance and free water clearance |
| Notes | Washout period: 48 hours between intervention phases, duration of each phase: 24-hour treatment + 48-hour washout, blinding: not blinded (open label), dropouts and deviations: two children excluded from the furosemide-only phase, three from the albumin + furosemide phase due to early recovery or adverse effects |
| Outcome | Furosemide infusion (FU) (n=13) | Albumin + furosemide infusion (HA+FU) (n=14) | p-value | Statistical significance |
| Weight loss (%) | 0.8 (-1.9 to 4.1) | 5.2 (3.1-8.8) | 0.006 | Yes |
| Urine volume (mL/kg per hour) | 1.33 (0.79-1.88) | 3.27 (2.04-4.50) | 0.01 | Yes |
| Urine osmolality (mOsm/kg) | 368 (318-446) | 315 (220-426) | 0.13 | No |
| Urine sodium (mEq/day) | 30 (10-122) | 58 (30-366) | 0.08 | No |
| Urine chloride (mEq/day) | 56 (16-168) | 104 (30-303) | 0.07 | No |
| Urine potassium (mEq/day) | 14.9 (5-20.5) | 30 (11-40.5) | 0.07 | No |
| Cosm (mL/day) | 880 (510-2105) | 1600 (916-4140) | 0.01 | Yes |
| Cfw (mL/day) | -162 (-446 to -70) | -190 (-960 to 280) | 0.18 | No |
| Adverse events | Metabolic alkalosis (n=1), peritonitis (n=1) | Hypokalaemia (n=1), oedema resolved early (n=2) | - | - |
| Outcome | Certainty of evidence (GRADE) | Explanation |
| Weight loss (%) | ⊕⊕⊝⊝ Low | Downgraded for risk of bias (no blinding, carryover bias and lack of published protocol), imprecision (wide CI) and publication bias (single included study) |
| Urine volume (mL/kg per hour) | ⊕⊕⊕⊝ Moderate | Downgraded for risk of bias and publication bias |
| Urine osmolality (mOsm/kg) | ⊕⊝⊝⊝ Very low | Downgraded for risk of bias, imprecision (CI include 0), publication bias and indirectness; graphs show fluctuation without a clear trend or benefit |
| Urine sodium (mEq/day) | ⊕⊝⊝⊝ Very low | Downgraded for risk of bias, imprecision (CI include 0), publication bias and indirectness |
| Urine chloride (mEq/day) | ⊕⊝⊝⊝ Very low | Downgraded for risk of bias, imprecision (CI include 0), publication bias and indirectness (clinical importance unclear) |
| Urine potassium (mEq/day) | ⊕⊝⊝⊝ Very low | Downgraded for risk of bias, imprecision (CI include 0), publication bias, indirectness and inconsistency |
| Cosm (mL/day) | ⊕⊕⊝⊝ Low | Downgraded for risk of bias, imprecision (wide CI) and publication bias (single included study) |
| Author (year) | Study design | Population | Intervention and comparator | Outcomes |
| Huque et al. (2014) [ | Descriptive cross-sectional study | 40 children with nephrotic syndrome and resistant oedema | Albumin + furosemide versus mannitol + furosemide | Weight, oedema, urine output |
| Singh et al. (2015) [ | Prospective comparative study | 54 children with idiopathic nephrotic syndrome | Albumin versus FFP | Time to oedema resolution and cost of treatment |
| Bircan et al. (2001) [ | Prospective observational study | 14 children with nephrotic syndrome | Albumin + furosemide (no comparator) | Plasma volume and similar parameters pre- and post-treatment |
| Garg et al. (2020) [ | Randomised crossover trial | 24 children with nephrotic syndrome | 20% albumin versus 5% albumin | Weight reduction, urine output, safety parameters |
| Akcicek et al. (1995) [ | Randomised crossover trial | 12 adults with nephrotic syndrome | Furosemide versus albumin versus furosemide + albumin combined | Urine output, Na/K excretion, serum albumin |
| Na et al. (2001) [ | Randomised crossover trial | 7 adults with nephrotic syndrome | Furosemide alone versus albumin + furosemide | Urine output, sodium excretion, diuretic response |
| Tabel et al. (2008) [ | Case series | 18 children with nephrotic syndrome | Observational study | Observational study |
| Tsuruga et al. (2009) [ | Report of case series | 6 children with nephrotic syndrome | Recombinant albumin (no comparator) | Safety, allergic reactions, diuretic response |
| Ghafari et al. (2011) [ | Randomised control trial | 10 adults with nephrotic syndrome | Furosemide versus albumin versus furosemide + albumin combined | Urine output, excretion of sodium, albumin and furosemide |
| Fliser et al. (1999) [ | Randomised crossover trial | 6 adults with nephrotic syndrome | Furosemide versus albumin versus furosemide + albumin combined | Urine output, sodium balance, GFR |
| Pasini et al. (2015) [ | Retrospective observational study | 231 children with nephrotic syndrome | Observational study on steroid use | Treatment trends, practice variation |
| Tanzi et al. (2003) [ | Drug use evaluation | 1649 adult and 23 paediatric inpatients receiving albumin | Audit of albumin use (observational) | Appropriateness of albumin prescriptions |
| Otukesh et al. (2024) [ | Quasi-randomised | 42 children with nephrotic syndrome | Albumins versus mannitol | Weight reduction |
| Lee et al. (2000) [ | Parallel RCT | 26 children with nephrotic syndrome | Albumin versus placebo | Weight loss, time to remission, serum electrolytes |
| Haws and Baum (1993) [ | Paediatric case series | 21 children with nephrotic syndrome | Albumin + 1 diuretic versus albumin + 2 diuretics | Urine output, weight loss |
| Author (year) | Reason for exclusion | Relevance to evidence gap |
| Huque et al. (2014) [ | Used mannitol rather than placebo or standard care | Explores albumin efficacy and safety and real-world alternative comparators |
| Singh et al. (2015) [ | Comparator not eligible (used FFP) | Supports albumin safety, clinical equipoise and need for placebo-controlled trials |
| Bircan et al. (2001) [ | No comparator, observational study | Demonstrates the mechanism of action and the need for RCTs |
| Garg et al. (2020) [ | No albumin-free control arm | Explores albimun’s dosing options and relativistic effects |
| Akcicek et al. (1995) [ | Adult population | Claims to be the first study to explore the pharmacokinetics of combined albumin + furosemide |
| Na et al. (2001) [ | Adult population | Demonstrates enhanced diuresis with albumin and foundational physiological response |
| Tabel et al. (2008) [ | Observational study | Explores volume status during oedema of nephrotic syndrome and negates the need for albumin |
| Tsuruga et al. (2009) [ | No comparator group | Explores novel albumin formulations and early paediatric safety profile |
| Ghafari et al. (2011) [ | Adult population | Supports rationale for albumin co-administration |
| Fliser et al. (1999) [ | Adult population | Highlights the transient benefit of albumin and the place for higher diuretic doses |
| Pasini et al. (2015) [ | Study question not relevant to our review | Illustrates variation in real-world practice and the need for standardised protocols |
| Tanzi et al. (2003) [ | Audit, not interventional or comparative | Reveals widespread off-label albumin use, supports the need for clearer paediatric guidelines |
| Otukesh et al. (2024) [ | Foreign language and ineligible comparator | Explores albumin efficacy and safety and real-world alternative comparators |
| Lee et al. (2000) [ | Foreign language | Explores the exact question as our review |
| Haws and Baum (1993) [ | Retrospective observational study with albumin in all groups | Early observational data demonstrating albumin use and a poor safety profile |
| Category | Details |
| Pre-registered protocol | The review was registered on PROSPERO prior to data extraction, enhancing transparency and reducing bias. |
| PRISMA adherence | All reporting followed PRISMA 2020 guidelines, including study selection flow diagrams and structured methods. |
| Hybrid methodology | We combined rigorous systematic review with narrative evidence mapping, allowing both synthesis and exploration of excluded-but-relevant literature. |
| Paediatric focus | Exclusively focused on children aged 1-18 years with nephrotic syndrome, improving clinical applicability. |
| Dual reviewer screening | Title/abstract and full-text screening were conducted independently by two reviewers to reduce selection bias. |
| Comprehensive literature base | We included peer-reviewed studies and prior systematic reviews, with additional full-text articles identified through snowballing and reference list screening, substantially expanding the evidence base beyond initial database results. |
| Category | Details |
| Single included RCT | Only one trial met full inclusion, limiting quantitative synthesis and meta-analysis. |
| Small sample size | The included RCT had only 16 participants, increasing imprecision and reducing generalisability. |
| Heterogeneous excluded studies | Excluded-but-relevant studies varied in design, outcomes and population, limiting comparability. |
| Language bias | Non-English studies without accessible full texts were excluded, which may omit valuable data. |
| Surrogate outcomes dominate | Most studies focused on physiological rather than patient-centred outcomes. |
| Short follow-up periods | Few studies assessed outcomes beyond 24-48 hours, limiting understanding of sustained effects. |
| Pragmatic mapping inclusion | Decisions to map rather than formally include certain studies may introduce indirectness. |
| Protocol deviation I | We adopted a hybrid approach by adding narrative evidence mapping layer, which was not originally planned. The study title was also amended to reflect this broader scope. |
| Protocol deviation II | Although our protocol did not plan for snowballing or reference screening, these methods were employed post hoc to identify additional relevant studies. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Diseases and Glomerulopathies · Chronic Kidney Disease and Diabetes · Lymphatic Disorders and Treatments
Introduction and background
Nephrotic syndrome is one of the most prevalent glomerular disorders in childhood, with an annual incidence ranging between one and seven per 100,000 children worldwide [1]. It is defined by the presence of heavy proteinuria, hypoalbuminaemia and oedema, often accompanied by hyperlipidaemia. Oedema is the most visible and distressing manifestation of the condition, with severity ranging from mild periorbital swelling to generalised anasarca [2]. In hospitalised children, oedema can cause significant morbidity, discomfort, delayed recovery and extended hospital stays [3].
The underlying mechanisms of oedema in nephrotic syndrome are multifactorial. Two dominant theories explain the pathogenesis of oedema [4-6]. The underfill hypothesis suggests that hypoalbuminaemia reduces plasma oncotic pressure, leading to intravascular volume depletion and secondary sodium and water retention via the renin-angiotensin-aldosterone system (RAAS). In contrast, the overfill hypothesis attributes oedema to primary renal sodium retention, driven by tubular dysfunction in the distal nephron [4-6]. Both mechanisms likely contribute to varying degrees depending on disease stage and severity [3].
Management of oedema in children with nephrotic syndrome typically involves fluid and salt restriction along with loop diuretics such as furosemide. However, diuretic resistance is commonly encountered, particularly in the setting of profound hypoalbuminaemia [7]. In such cases, intravenous (IV) albumin is frequently administered in combination with diuretics, with the rationale that albumin can temporarily increase plasma oncotic pressure, improve intravascular volume and enhance renal perfusion, thereby restoring the efficacy of loop diuretics [3,8].
This approach is widely used in clinical practice across many paediatric nephrology units [9,10]. However, its benefits remain uncertain. Some studies report short-term improvements in urine output and weight loss [11], but the effects appear transient unless remission of proteinuria is achieved. Importantly, albumin infusion is not without risk. Adverse events, including acute hypertension, hypokalaemia, hypernatraemia, fluid overload and respiratory distress, have been frequently documented [12]. In one retrospective study, hypertension requiring urgent management occurred in nearly half of albumin treatment episodes, and one child developed congestive heart failure [13]. Given its potential for harm and resource intensity, the use of IV albumin in this setting warrants a strong evidentiary foundation demonstrating both clinical benefit and safety.
However, the current literature does not provide the clarity required for paediatric clinical practice. Several previous systematic reviews have attempted to assess the role of intravenous albumin in oedematous or hypoalbuminaemic patients, but all have critical limitations that restrict their applicability to children with nephrotic syndrome. Elwell et al. (2003) conducted a narrative review that focused primarily on adult populations in critical care and cirrhotic settings. While they discussed pharmacological mechanisms, their findings were inconsistent and based on small studies, with limited relevance to paediatric nephrotic syndrome [7]. Kitsios et al. (2014) performed a meta-analysis of eight randomised controlled trials, largely in adults, and reported modest increases in urine output and sodium excretion at eight hours post-intervention but no sustained effects at 24 hours [14]. Their analysis excluded paediatric populations entirely. Hedin et al. (2022), although published in a paediatric nephrology journal, synthesised data from five studies, four of which were conducted in adults, and did not stratify findings by age group, making its conclusions difficult to extrapolate to children [3]. The Cochrane review by Ho et al. (2019) aimed to evaluate albumin therapy in nephrotic syndrome across all ages, but ultimately included only one paediatric study that was published in Korean and inaccessible to many readers [5]. Collectively, these reviews highlight a striking lack of focused, high-quality evidence to guide the use of IV albumin in hospitalised children with nephrotic syndrome and significant oedema, particularly in comparison to standard treatment without albumin.
This systematic review was designed to fill that gap. Following a registered protocol, it evaluates the effectiveness and safety of intravenous albumin, with or without diuretics, versus no albumin in hospitalised children aged 1-18 years with nephrotic syndrome and oedema. By focusing on comparative studies in this well-defined clinical context, the review aimed to support evidence-based decision-making and improve the management of a high-impact paediatric condition.
Review
Methods and materials
Protocol and Registration
This review was conducted according to a predefined protocol registered with the International Prospective Register of Systematic Reviews (PROSPERO: CRD420251102387), on July 11, 2025, which is available at https://www.crd.york.ac.uk/PROSPERO/view/CRD420251102387. The reporting of this systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Appendices).
Eligibility Criteria
Eligibility was defined using the Population, Intervention, Comparator, Outcomes, Study Designs and Timeframe (PICOST) framework, as shown in Table 1.
We excluded studies meeting any of the criteria shown in Table 2.
Information Sources
We searched the following databases from January 1, 1990, to June 30, 2025: PubMed, Cochrane CENTRAL, Google Scholar and Europe PMC.
Reference lists of eligible articles and previous systematic reviews were manually screened to identify additional studies, although this was deviation from our published protocol but ensured that search was rigorous and no eligible studies skipped.
Search Strategy
A comprehensive search strategy using a combination of MeSH terms and free-text keywords was developed. The full search strategy was published with the protocol on PROSPERO and is summarised in the Appendices.
Study Selection
Search results were imported into Rayyan (Rayyan Systems Inc., Cambridge, MA) for deduplication and screening. Two reviewers independently and blindly screened titles and abstracts for relevance. Conflicts were resolved by consensus, and the results were tracked (Appendices). Full texts were then assessed for eligibility based on the predefined criteria independently by both authors. Disagreements were resolved through discussion and consensus.
Data Extraction
A standardised data extraction form was used to collect information on study characteristics (design, setting and sample size), population demographics, albumin dosing and administration protocols, comparator interventions and outcomes. Two reviewers independently extracted data, and discrepancies were resolved by consensus.
Risk of Bias Assessment
For included studies, we assessed risk of bias using the appropriate tool based on study design. Included RCT was assessed using the Cochrane Risk of Bias 2.0 tool (ROB 2), and observational studies, if included, would have been assessed using ROBINS-I.
Data Synthesis
Due to the limited number of eligible studies and marked heterogeneity in study design and outcome reporting, meta-analysis was not feasible. Results from the included comparative study are reported descriptively.
Mapping Extension (Hybrid Layer)
Given the paucity of fully eligible studies, we extended the review to incorporate a structured evidence mapping exercise aimed at identifying excluded-but-relevant studies that could contribute contextual insight or highlight important evidence gaps. This was a planned deviation from the registered protocol, intended to support hypothesis generation and inform future research priorities. Relevance was defined a priori as studies involving children with nephrotic syndrome who received intravenous albumin, either with or without a comparator, regardless of study design, language or outcomes reported. Studies conducted exclusively in adults but otherwise meeting all inclusion criteria were also included to provide contextual breadth. Candidate studies were identified based on proximity to eligibility criteria, such as absence of a comparator arm, use of non-standard outcomes or inability to isolate paediatric data. All mapped studies were categorised into one of five predefined exclusion domains: (A) inappropriate comparator, (B) no comparator, (C) non-English language, (D) contextual or case series and (E) systematic reviews. Selection of studies for mapping was conducted after final exclusions were logged. The process was performed by one reviewer (SBN) and cross-checked narratively with the screening log by a second reviewer (MAZ). These studies were included in the mapping tables to illustrate key exclusion patterns and signal potential directions for future research.
Results
Systematic Review Findings
A comprehensive search of multiple databases yielded a substantial number of records. After deduplication, all remaining titles and abstracts were screened against predefined eligibility criteria. The majority of exclusions at this stage were due to clearly irrelevant populations (e.g., adults), interventions (e.g., non-albumin agents) or study types (e.g., reviews or case reports), as shown in Table 3.
Full-text review was conducted for studies included in the initial screening. Several were excluded at this stage for reasons such as lack of a comparator group or outcomes unrelated to our study question. Ultimately, only one study (Dharmaraj et al. (2009) [11]) met all eligibility criteria and was included in the systematic review. Figure 1 presents the PRISMA flow diagram.
PRISMA flow diagramCreated according to PRISMA 2020 Guidelines using the PRISMA creation tool: Creative Commons Attribution (CC BY 4.0) license [15]PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
The included study was an open-label, randomised crossover trial conducted in India, comparing IV albumin plus furosemide to furosemide alone in children with nephrotic syndrome and persistent oedema. Sixteen children aged 3-18 years were enrolled and received both interventions in sequence, separated by a 48-hour washout period. Key characteristics of the study design, population, intervention and outcomes are summarised in Table 4.
The primary outcome (change in urine output) favoured the albumin group, with a statistically significant increase compared to furosemide alone (p=0.01 for absolute rates and p=0.008 for percentage change in urine volume from baseline). For the primary outcome of weight loss as per our review question, this study reported a statistically significant difference (p=0.006), favouring the albumin group.
The study reported statistically significant improvements in several urinary parameters favouring the albumin plus furosemide group when measured as percentage change from the baseline. These included greater urine volume, higher urinary sodium, potassium and chloride excretion, increased urine osmolality and osmolal clearance. Blood pressure and serum electrolytes did not differ significantly between groups. The authors concluded that albumin may transiently enhance the diuretic response to furosemide in children with nephrotic syndrome and persistent or refractory oedema resulting in better weight loss, urine output and natriuresis but highlighted that the benefit was likely due to enhanced drug delivery rather than sustained intravascular volume expansion. Table 5 summarises the results of the included study.
These findings, while suggestive of a potential benefit, must be interpreted with caution due to methodological limitations. The study employed a 48-hour washout period, which is likely insufficient to eliminate residual pharmacological effects of albumin and furosemide, thereby introducing a serious risk of carryover bias. In addition, the trial was open-label, and the details provided regarding sequence generation or allocation concealment are minimal. These factors collectively limit the internal validity of the findings. A structured risk of bias assessment using the Cochrane ROB 2 tool judged the study as having “some concerns” overall, due to the open-label design, inadequate washout period and no publication of pre-designed protocol and outcome selection (Figure 2).
Cochrane ROB 2 tool
We assessed the certainty of evidence for the reported outcomes using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. As only one randomised trial contributed data, all outcomes began with a high certainty rating but were subsequently downgraded for risk of bias, imprecision, suspected publication bias, inconsistency and indirectness (Table 6). However, the application of the GRADE framework was constrained by the inclusion of only one study. Inconsistencies in reported statistics, absence of confidence intervals for several outcomes and discrepancies between absolute and percentage changes (e.g., in potassium levels) further limited the ability to apply the downgrading criteria with full rigour.
Table 6: GRADE summary of findingsGRADE: Grading of Recommendations, Assessment, Development and Evaluation Cosm (Osmolal Clearance) = (Urine Osmolality x Urine Volume) / Plasma Osmolality
Narrative Mapping and Evidence Gap Findings
While only one study met eligibility criteria for full inclusion, several additional studies were considered relevant to the research question and were mapped narratively to describe the broader evidence landscape. These studies were excluded due to methodological limitations, inappropriate comparators, lack of control groups or language restrictions. Their inclusion here highlights critical evidence gaps and patterns across study types (Tables 7, 8).
Comparator not suitable to assess efficacy of albumin: Two studies used comparators that were active agents with osmotic or diuretic properties, rendering them unsuitable as controls to isolate albumin’s effect. Singh et al. (2015) compared albumin to fresh frozen plasma (FFP) in a randomised trial of 54 children, with both groups receiving furosemide. The study was excluded because FFP itself is an albumin analogue and pharmacologically active, limiting interpretability [16]. Huque et al. (2014) compared albumin-furosemide with mannitol-furosemide in 40 children [2]. No statistically significant difference was observed between groups. The study was excluded because mannitol is an osmotic diuretic and thus an inappropriate comparator for assessing albumin’s efficacy in isolation.
No comparator: Two studies used albumin in all treatment arms or as part of an uncontrolled intervention, precluding comparative conclusions. Both studies demonstrated feasibility but could not inform on effectiveness. Garg et al. (2020) retrospectively studied 25 children who all received albumin plus furosemide, with differences in dosing protocols; hence, the study was excluded [18]. Bircan et al. (2001) evaluated albumin plus diuretics in children with minimal change nephrotic syndrome, but the study was excluded for not having a comparator arm, and the outcomes did not align with our research question either [17].
Language of publication: Two studies met some of the other eligibility criteria but were excluded due to non-English publication. Otukesh et al. (2004), published in Persian, compared albumin and mannitol, showing significant differences for some outcomes, while none for the other [24]. Lee et al. (2000), the only included study in the Cochrane review by Ho et al. (2019), was a Korean-language single-blind RCT comparing albumin with furosemide versus furosemide alone in a group of 26 patients [25]. It showed a shorter time to remission in the albumin group, but an earlier time of first relapse as well. There was no significant difference in relapse rate at one year and relapse frequency within the first year. These studies underscore the risk of language bias in evidence synthesis.
Contextual but ineligible for mapping: Nine studies were excluded due to population mismatch, non-comparative designs or focus on biochemical/pharmacokinetic outcomes (Figure 3). Fliser et al. (1999) [8], Ghafari et al. (2011) [10] and Na et al. (2001) [20] studied adult or mixed populations. Pasini et al. (2015) [23] and Tanzi et al. (2003) [9] reviewed the practices across various paediatric units. Tabel et al. (2008) [21] lacked a comparator, while Haws and Baum [13] (1993) was a retrospective observational study. Akcicek et al. (1995) [19] and Tsuruga et al. [22] (2009) were focused on albumin kinetics.
Outcomes reported by different study types among excluded studiesRCT: randomised controlled trial
Systematic reviews: Four previous reviews were identified that addressed the use of albumin in patients with oedema or hypalbuminaemia. None were eligible for formal inclusion as per our protocol. Elwell et al. (2003) [7] and Kitsios et al. (2014) [14] synthesised evidence primarily from adult populations in critical care or cirrhotic settings, without a specific focus on nephrotic syndrome or children. Hedin et al. (2022) did include one paediatric nephrotic syndrome study, but otherwise drew mainly on adult trials and did not stratify outcomes by age group [3]. Ho et al. (2019), a Cochrane review, aimed to assess the effects of albumin infusion in people with nephrotic syndrome [5]. Although the scope included both adults and children, only one eligible study (Lee et al. (2000) [25]) was identified and included. This study involved the paediatric population but was published in Korean and thus was excluded from our review due to language restrictions.
Together, these reviews highlight a critical gap in the evidence base: the near-complete absence of high-quality randomised trials evaluating intravenous albumin in children with nephrotic syndrome. They also demonstrate inconsistent population definitions, lack of paediatric subgroup analysis and variation in outcome reporting, all of which contribute to uncertainty about when and how albumin should be used in this setting (Figure 4).
Ineligibility mapped by study typesRCT: randomised controlled trial
Discussion
Summary of Main Findings
This systematic review identified only one randomised controlled trial (Dharmaraj et al. 2009 [11]) that met full inclusion criteria for assessing the effectiveness and safety of intravenous albumin in hospitalised children with nephrotic syndrome and oedema. In Dharmaraj et al. (2009), a crossover trial, the combination of 20% albumin and intravenous furosemide produced a statistically significant increase in urine output and weight loss compared to furosemide alone [11]. Secondary outcomes, including changes in urine sodium, potassium, osmolality and osmolal clearance, also significantly improved in the albumin + furosemide arm. However, these changes were transient, with peak effects observed within the first few hours, and no significant difference in the time to oedema resolution or in reported adverse events between arms. These results suggest short-term physiological benefits without strong evidence of sustained clinical outcomes. The neutral tone of the findings aligns with the study’s limited sample size and lack of blinding, necessitating cautious interpretation.
Interpretation of Evidence
The findings from Dharmaraj et al. (2009) support the hypothesis that albumin may augment the natriuretic and diuretic response to loop diuretics in hypoalbuminemia states [11]. Mechanistically, this is consistent with pharmacokinetic principles suggesting that albumin enhances furosemide delivery to its site of action in the nephron [7,14,26]. Albumin-bound furosemide is secreted into the proximal tubule via organic anion transporters, and hypoalbuminaemia may limit this process by increasing volume of distribution and decreasing renal delivery. Albumin infusion may transiently increase intravascular volume and perfusion, improving drug delivery [17].
However, the study by Dharmaraj et al. has notable limitations that temper interpretation. Its open-label design introduces performance and detection bias. The crossover nature raises concerns about carryover effects, although a 48-hour washout period was used. Furthermore, the small sample size (n=16), with further exclusions during the interventions, limits precision and generalisability. Importantly, while short-term urine output and electrolyte changes were documented, patient-centred outcomes such as hospital stay, symptom relief or time to resolution were not measured.
Evidence Mapping Insights
Our mapping exercise of excluded-but-relevant studies revealed several recurring themes that shed light on the fragmented nature of the current evidence base. A substantial proportion of studies employed uncontrolled, single-arm designs or lacked an appropriate comparator group altogether, making it difficult to isolate the effect of albumin from natural diuretic response or disease progression (e.g., Bircan et al. (2001) [17], Huque et al. (2014) [2] and Singh et al. (2015) [16]). Among studies that did include comparison arms, many were excluded due to mismatched interventions or use of non-standardised co-therapies, reflecting significant heterogeneity in study design. Language barriers also emerged as a noteworthy issue: relevant studies such as Lee et al. (2000) [25] and Otukesh et al. (2024) [24], published in Korean and Persian, respectively, could not be included, highlighting the ongoing challenge of evidence exclusion based on language rather than content.
Another consistent finding was the prevalence of mixed populations or adult-only cohorts (e.g., Akcicek et al. (1995) [19], Ghafari et al. (2011) [10] and Fliser et al. (1999) [8]), which limits the applicability of findings to paediatric nephrotic syndrome. Even when children were included, subgroup data were often not disaggregated, further reducing interpretability. Outcome heterogeneity posed an additional barrier to synthesis. Across the mapped studies, researchers variably measured weight loss, urine volume, serum albumin levels, fractional excretion of sodium, time to oedema resolution or plasma volume expansion, without consistent timing, units or definitions. Safety assessment was also poorly addressed: few studies systematically reported adverse events, volume overload or electrolyte disturbances, and definitions of “refractory oedema,” “severe hypoalbuminaemia” or “response to treatment” were either absent or used inconsistently.
Despite these limitations, the mapping process provided valuable insights into clinical practice patterns and evidence gaps. The persistent use of albumin in some studies despite weak or equivocal data suggests clinical equipoise remains unresolved. In particular, the concentration of studies around early diuretic response reflects a mechanistic focus, often decoupled from long-term patient-centred outcomes. Repeated albumin dosing, cost implications, discharge timing and quality of life remain largely unexplored in the mapped literature. Collectively, these mapped studies highlight the lack of standardised methodologies, uniform outcome reporting and paediatric-specific trials, reinforcing the urgent need for well-designed prospective studies that address these deficiencies.
Comparison With Previous Reviews
Prior reviews and meta-analyses have repeatedly examined the role of albumin in patients with hypoalbuminaemia and diuretic resistance, yet they have consistently arrived at low-certainty conclusions. Elwell et al. (2003) conducted a narrative review focusing on the pharmacological rationale for combining albumin with furosemide in diuretic-resistant oedema [7]. They suggested that while some small studies showed transient clinical benefit, particularly in nephrotic syndrome, the overall evidence was inconsistent, heterogeneous and limited in quality. Their review primarily emphasised theoretical mechanisms such as improved intravascular volume status and enhanced diuretic delivery, rather than robust clinical outcomes. This mechanistic lens closely parallels some of the rationale presented in our review, but their conclusions were largely speculative due to the absence of systematic methodology or paediatric stratification.
Kitsios et al. (2014) performed a more methodologically rigorous meta-analysis, including eight RCTs, the majority of which involved adult populations and used crossover or parallel trial designs [14]. They found statistically significant increases in urine output and sodium excretion within eight hours of albumin administration, but these effects did not persist beyond 24 hours. Importantly, they reported no significant benefits in terms of patient-centred outcomes such as symptom resolution, length of stay or need for further intervention. Their findings reinforce the notion of a short-term physiological benefit that may not translate into meaningful clinical improvement, an observation echoed by the included study in our review (Dharmaraj et al. (2009) [11]).
Ho et al. (2019) conducted a Cochrane systematic review specifically evaluating albumin for the treatment of oedema in nephrotic syndrome [5]. Their review was comprehensive in scope but identified only one eligible study (Lee et al. (2000) [25]) published in Korean, which limited their ability to perform meta-analysis or draw strong conclusions. They highlighted pervasive methodological limitations across available studies, including unclear definitions of outcomes, small sample sizes and poor reporting. Their ultimate conclusion, that there was insufficient evidence to recommend routine albumin use in nephrotic syndrome, remains in alignment with our findings, although their inclusion of a non-English language study diverges from our eligibility criteria.
Hedin et al. (2022) represent the most recent and expansive attempt to synthesise the evidence base, incorporating both paediatric and adult populations [3]. They reported some increases in urine output, particularly with early combination therapy, but noted inconsistent effects on sodium excretion, no clear trends in long-term outcomes and a lack of stratified analysis by age group. Although one paediatric study was included, the review did not differentiate paediatric findings from adult results in a meaningful way, limiting its direct applicability to child health contexts.
Across all these reviews, a consistent pattern emerges: transient improvements in physiological parameters, no sustained effect on patient-centred outcomes and methodological weaknesses that preclude strong recommendations. Despite this, albumin continues to be used in practice, raising important questions about the drivers of clinical behaviour. These may include institutional norms, clinician perceptions of benefit in specific subgroups (e.g., those with severe hypoalbuminaemia or refractory oedema), lack of alternative therapies or a risk-averse approach in complex cases. None of the previous reviews have directly addressed this disconnection between guideline uncertainty and real-world use.
Our review, while similarly constrained by the limited evidence base, offers unique contributions by focusing specifically on hospitalised children with nephrotic syndrome and clinically significant oedema. Furthermore, our structured evidence mapping of excluded studies sheds additional light on the landscape of partially relevant research and highlights specific gaps that future studies must address. While our conclusions are aligned with the cautionary stance of earlier reviews, our methodological approach aims to move the field closer to resolving the enduring uncertainty surrounding albumin use in this vulnerable population.
Strengths of This Review
Table 9 shows the strengths of our systematic review.
Limitations of This Review
Table 10 shows the limitations of this review.
Clinical Implications
Based on available evidence, routine use of intravenous albumin in all hospitalised children with nephrotic syndrome and oedema is not supported. The combination may be considered in select cases, particularly those with severe hypoalbuminaemia (e.g., serum albumin < 20 g/L), refractory oedema unresponsive to escalating diuretics and no contraindications to fluid expansion (e.g., absence of pulmonary congestion or cardiac dysfunction). Even in these cases, cautious monitoring of fluid status, electrolytes and renal function is essential. Alternative strategies such as mannitol-furosemide or sequential nephron blockade (e.g., thiazide + loop diuretics) may offer comparable benefit with potentially lower risk [2,27].
Directions for Future Research
Adequately powered, blinded RCTs should be conducted in children with nephrotic syndrome to evaluate the efficacy and safety of albumin + diuretic therapy. Standardised definitions for “diuretic resistance,” “hypoalbuminaemia” and “oedema resolution” need to be used. We also recommend comparing albumin + furosemide versus alternative strategies (e.g., mannitol, hypertonic saline or combination diuretics). Long-term outcomes, such as hospital length of stay, relapse rates, time to remission and quality of life, must be incorporated. Mandatory adverse event reporting, including cardiovascular outcomes, fluid overload and electrolyte disturbances, is essential. For low-resource settings, where albumin is expensive or scarce, cost-effectiveness analyses must be conducted. Lastly, it is necessary to develop consensus guidelines based on available evidence to guide albumin use in paediatric nephrotic syndrome.
Conclusions
Current evidence for intravenous albumin in hospitalised children with nephrotic syndrome is very limited. The single included trial shows transient improvements in urine output and weight, but patient-centred outcomes remain largely unassessed, and benefits are modest and short-lived. Narrative mapping and prior reviews highlight major evidence gaps, including heterogeneous populations, varied interventions, absent comparators and sparse safety data. Routine albumin use cannot be universally recommended; it may be considered only in severe hypoalbuminemia or refractory oedema, with careful monitoring.
There is an urgent need for well-designed, adequately powered paediatric RCTs with standardised outcomes and systematic safety reporting. Future studies should also assess alternative therapies and cost-effectiveness to inform clinical guidelines. In summary, current evidence confirms only modest, short-term effects with no established patient-centred benefits. Major uncertainties remain regarding long-term safety, subgroup responses and broad clinical outcomes. Until these gaps are addressed, use of albumin should be highly cautious and guided by careful risk-benefit assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nephrotic syndrome in childhood Lancet Eddy AA Symons JM 62963936220031294406410.1016/S 0140-6736(03)14184-0 · doi ↗ · pubmed ↗
- 2Albumin and furosemide versus mannitol and furosemide in the treatment of diuretic resistant oedema in childhood nephrotic syndrome Bangladesh J Child Health Huque SS Rahman MH Uddin GM Jahan S Begum A Roy RR Hossain MM 7478382014
- 3Furosemide and albumin for the treatment of nephrotic edema: a systematic review Pediatr Nephrol Hedin E BijelićV Barrowman N Geier P 174717573720223523903210.1007/s 00467-021-05358-4 · doi ↗ · pubmed ↗
- 4Sodium retention in nephrotic syndrome is due to an intrarenal defect: evidence from steroid-induced remission Nephron Brown EA Markandu N Sagnella GA Jones BE Mac Gregor GA 290295391985398257410.1159/000183392 · doi ↗ · pubmed ↗
- 5Human albumin infusion for treating oedema in people with nephrotic syndrome Cochrane Database Syst Rev Ho JJ Adnan AS Kueh YC Ambak NJ Van Rostenberghe H Jummaat F 07201910.1002/14651858.CD 009692.pub 2PMC 669968031425606 · doi ↗ · pubmed ↗
- 6Role for intrarenal mechanisms in the impaired salt excretion of experimental nephrotic syndrome J Clin Invest Ichikawa I Rennke HG Hoyer JR 91103711983684856310.1172/JCI 110756 PMC 436841 · doi ↗ · pubmed ↗
- 7Combined furosemide and human albumin treatment for diuretic-resistant edema Ann Pharmacother Elwell RJ Spencer AP Eisele G 6957003720031270894910.1345/aph.1C 320 · doi ↗ · pubmed ↗
- 8Coadministration of albumin and furosemide in patients with the nephrotic syndrome Kidney Int Fliser D Zurbrüggen I Mutschler E Bischoff I Nussberger J Franek E Ritz E 629634551999998708710.1046/j.1523-1755.1999.00298.x · doi ↗ · pubmed ↗