Recurrent Clostridium difficile Infections in a Patient With Ulcerative Colitis: A Case Report
Osama Nadeem, Muhammad Soban Imran, Nasir Siddique

TL;DR
An elderly patient with ulcerative colitis experienced multiple Clostridium difficile infections despite antibiotic treatments, highlighting the challenges in managing this condition in high-risk patients.
Contribution
This case report emphasizes the severity and recurrence of CDI in elderly UC patients and suggests the need for alternative treatments like FMT.
Findings
An elderly UC patient had three CDI episodes during a four-month hospitalization.
Standard antibiotic treatments failed to prevent CDI recurrence in this patient.
The case underscores the need for alternative therapies like FMT in managing recurrent CDI.
Abstract
Clostridium difficile infection (CDI) poses a substantial clinical challenge, especially in patients with inflammatory bowel disease (IBD), particularly ulcerative colitis (UC). Patients with UC are at greater risk of CDI and tend to experience a more severe disease course and higher rates of recurrence than the general population. We report a case of an elderly man in his early 90s with a long-standing history of UC treated with mesalazine, who had a prior hospitalization for hyponatremia and a history of CDI. During his most recent four-month hospitalization, he developed three separate episodes of CDI, confirmed by stool PCR and toxin assays. Despite treatment with vancomycin, metronidazole, and fidaxomicin in succession, he experienced recurrent episodes of CDI that ultimately progressed to septic shock and death. This case highlights the nature of recurrent CDI in this patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
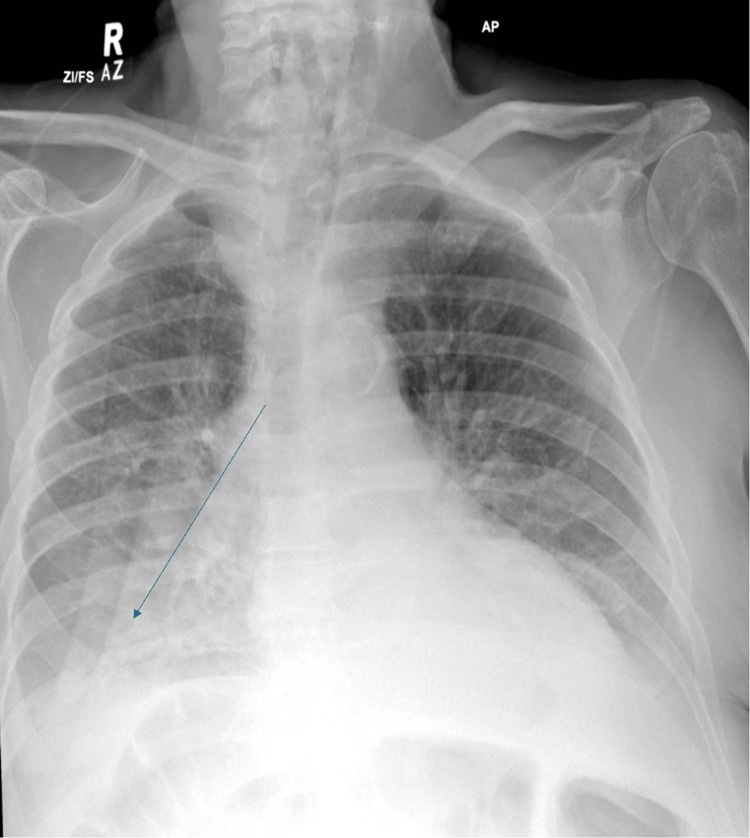 Figure 1
Figure 1 Figure 2
Figure 2| Test Name | Result | Out of Range | Reference Range |
| Neutrophils | 16.86 × 10⁹/L | Yes | 1.80-7.50 × 10⁹/L |
| WBC | 20.5 × 10⁹/L | Yes | 4.0-11.0 × 10⁹/L |
| CRP | 101 mg/L | Yes | 0-5 mg/L |
|
| Positive | Yes | Negative |
| Test Name | Result | Out of Range | Reference Range |
| Faecal calprotectin | 1,373 µg/g | Yes | 0-100 µg/g |
| Neutrophils | 14.10 × 10⁹/L | Yes | 1.80-7.50 × 10⁹/L |
| WBC | 16.6 × 10⁹/L | Yes | 4.0-11.0 × 10⁹/L |
| CRP | 202 mg/L | Yes | 0-5 mg/L |
|
| Positive | Yes | Negative |
| Vital Sign | Value |
| Blood pressure | 104/70 mmHg |
| Pulse | 90 bpm |
| Temperature | 38.0 °C (100.4 °F) |
| Respiratory rate | 17 breaths/min |
| Height | 1.89 m |
| Weight | 60.1 kg |
| Oxygen saturation (SpO₂) | 97% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Microscopic Colitis · Gastrointestinal motility and disorders
Introduction
Clostridioides difficile infection (CDI) is defined as a symptomatic infection of the large intestine caused by the anaerobic, spore-forming, gram-positive bacterium C. difficile. Recurrent CDI is defined as an episode of CDI occurring within eight weeks of a previous episode. CDI is widely recognized as the leading cause of antibiotic-associated diarrhoea, with increasing frequency and severity worldwide [1,2]. Inflammatory bowel disease (IBD), particularly ulcerative colitis (UC), occurs in the setting of a heightened risk of CDI due to alterations in the gut microbiota and impaired intestinal immunity [1,3]. CDI can negatively impact the clinical course of UC, leading to increased flares, hospitalizations, morbidity, and mortality [1,2]. The elderly with UC may be particularly at risk for CDI due to age-related changes in immunity, greater exposure to antibiotics, and the presence of comorbidities [1,3]. Recurrence remains a significant concern despite the use of recommended antimicrobial treatments, including vancomycin, metronidazole, and fidaxomicin [2,4]. New therapies have shown promise, such as faecal microbiota transplantation (FMT), which may provide new therapeutic options for complicated CDI in patients with UC [4-6]. This report draws attention to recurrent CDI as a persistent clinical challenge in elderly patients with UC and underscores the need for innovative strategies to improve management.
Case presentation
We present a case of an elderly male (in his early 90s) with UC who was being treated with mesalazine and was brought to the hospital with severe hyponatraemia, delirium, and a fall. He was admitted for four months and had three separate episodes of CDI, all confirmed by stool studies. The CDI persisted through treatment with vancomycin, metronidazole, and fidaxomicin, and ultimately progressed to septic shock and death.
First CDI episode (September 20, 2024): The patient presented with loose stool, and stool assays confirmed CDI via stool PCR (in-house PCR from an MFT hospital laboratory). He was febrile at 38.2°C (Table 1). A stat dose of IV gentamicin 320 mg was administered, along with IV co-amoxiclav 1.2 g three times daily for an unknown infection source, likely urinary in origin. This was later stepped down to oral co-amoxiclav 500 mg/125 mg three times daily for a total of seven days. During this time, the patient was also started on oral vancomycin 125 mg four times daily. Following this treatment, symptoms showed minimal improvement.
Second CDI episode (October 20, 2024): The patient presented with several episodes of black, loose stool (types 6/7 on the Bristol Stool Chart). Again, stool assays confirmed CDI (Table 2). WBC count was 16.6 × 10⁹/L; lactate was 2.4 mmol/L; CRP increased from 115 mg/L (October 16) to 202 mg/L (October 20); temperature was 38.5°C; and BP was 99/51 mmHg (Table 3). He was treated with fidaxomicin 200 mg twice daily for a 10-day course. Faecal calprotectin was also significantly elevated at 1,373 µg/g. An important concurrent development was the onset of hospital-acquired pneumonia on October 26, based on clinical findings and chest X-ray (Figure 1). He was initially treated with IV co-amoxiclav, followed by escalation to tazocin for five days. It is worth noting that immunosuppressive therapy for UC was not escalated during this period.
Chest X-ray taken on 24 October 2024 showing right-sided haziness and blunting of the costophrenic angle, suggestive of pneumonia. The patient was subsequently started on antibiotics on October 26, 2024.
Third CDI episode (November 16-17, 2024): Despite ongoing treatment, the patient’s symptoms did not improve, and he experienced recurrent bouts of diarrhoea and melena. He was hypotensive (BP 74/42 mmHg), febrile (38.5°C), and had an elevated lactate of 2.7 mmol/L. Toxic megacolon was ruled out by abdominal X-ray (Figure 2). He rapidly deteriorated despite initiation of IV metronidazole 500 mg every eight hours and oral vancomycin 125 mg every six hours, and he passed away on November 17, 2024, likely due to Type 2 myocardial infarction (MI) secondary to sepsis.
Abdominal X-ray showing a non-specific bowel gas pattern.
Discussion
This case highlights a subset of elderly patients with UC who are at greater risk and experience more complications from recurrent CDI. Distinguishing UC flares from CDI episodes is clinically challenging, in part due to overlap in symptomatology, including diarrhoea and abdominal pain [1-3]. An elevated faecal calprotectin level is indicative of inflammation in the colon but is not specific for differentiating CDI from exacerbations of UC [2,6]. This diagnostic overlap often leads to delays in appropriate therapy, emphasizing the importance of stool toxin assays or PCR testing in any UC patient experiencing worsening symptoms. The risk of CDI is higher in individuals with prior antibiotic exposure, particularly with broad-spectrum antibiotics, due to the disruption of balanced gut flora and subsequent colonization by pathogens [2,4]. Immunosuppressive therapy, often required in UC, further compounds this risk by altering host immune responses. Furthermore, frailty, comorbidities, and hospitalization are recognized predictors of recurrent CDI, which may partly explain the clinical course observed in this patient [7].
Vancomycin remains the current first-line treatment, with fidaxomicin as a second-line option. However, the recurrent nature of CDI in this patient indicates that alternative approaches are warranted [4,6]. The literature provides evidence that FMT yields favourable outcomes in treating recurrent CDI [8] and may be safely used in patients with recurrent CDI, particularly when standard antimicrobial therapy options are exhausted [4,6]. Another therapeutic option is bezlotoxumab, a human monoclonal antitoxin antibody that binds to C. difficile toxin B and neutralises its activity, thereby preventing recurrence of infection [9].
The findings of this case report align with previous literature [6]. This case underscores the critical importance of timely identification, appropriate stool-based diagnostics, and coordinated multidisciplinary care in older patients with UC who develop recurrent diarrhoea. For this vulnerable group, distinguishing CDI from a UC flare is essential to ensure prompt and effective management. It also emphasizes the need to consider advanced therapeutic strategies, such as faecal microbiota transplantation, bezlotoxumab, antimicrobial stewardship, and patient-specific risk assessment, to reduce both the occurrence and recurrence of CDI in individuals with underlying UC.
Conclusions
This case demonstrates the significant risk and complexity of managing recurrent CDI in older patients with UC. Patients with UC are at an increased risk of developing recurrent CDIs, which pose substantial challenges in clinical management and are associated with higher mortality. Complications such as septic shock can arise even when an appropriate antibiotic regimen is prescribed. This reinforces the importance of close monitoring, judicious antibiotic stewardship, and consideration of alternative approaches, such as FMT, to help reduce morbidity and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clostridium difficile infection and inflammatory bowel disease: understanding the evolving relationship World J Gastroenterol Navaneethan U Venkatesh PG Shen B 489249041620102095427510.3748/wjg.v 16.i 39.4892 PMC 2957597 · doi ↗ · pubmed ↗
- 2Clostridium difficile infection in patients with ulcerative colitis treated with tofacitinib in the Ulcerative Colitis Program Inflamm Bowel Dis Loftus EV Baumgart DC Gecse K 7447512920233579249310.1093/ibd/izac 139PMC 10152280 · doi ↗ · pubmed ↗
- 3Clostridium difficile and inflammatory bowel disease: role in pathogenesis and implications in treatment World J Gastroenterol Nitzan O Elias M Chazan B Raz R Saliba W 757775851920132428234810.3748/wjg.v 19.i 43.7577 PMC 3837256 · doi ↗ · pubmed ↗
- 4Management of Clostridioides difficile infection in patients with inflammatory bowel disease Intest Res Khanna S 2652741920213280687310.5217/ir.2020.00045 PMC 8322030 · doi ↗ · pubmed ↗
- 5Clostridioides difficile infection: update on management Am Fam Physician Mounsey A Lacy Smith K Reddy VC Nickolich S 1681751012020 https://pubmed.ncbi.nlm.nih.gov/32003951/32003951 · pubmed ↗
- 6Recurrence of Clostridium difficile infection in patients with inflammatory bowel disease: the RECIDIVISM study Am J Gastroenterol Razik R Rumman A Bahreini Z Mc Geer A Nguyen GC 1141114611120162721592410.1038/ajg.2016.187 · doi ↗ · pubmed ↗
- 7Frailty is a predictor for worse outcomes in patients hospitalized with Clostridioides difficile infection Ann Gastroenterol Chaar A Yoo JW Nawaz A Rizwan R Agha OQ Feuerstadt P 442448372024 http://www.annalsgastro.gr/index.php/annalsgastro/article/view/74373897408710.20524/aog.2024.0898 PMC 11226747 · doi ↗ · pubmed ↗
- 8Systematic review with meta-analysis: long-term outcomes of faecal microbiota transplantation for Clostridium difficile infection Aliment Pharmacol Ther Li YT Cai HF Wang ZH Xu J Fang JY 4454574320162666264310.1111/apt.13492 · doi ↗ · pubmed ↗