Cognitive Behavior Therapy With and Without Narrative Assessment and Suicide Attempts: A Systematic Review and Meta-Analysis
Wilco C. Janssen, Saskia Y. M. Mérelle, Wouter van Ballegooijen, Renske Gilissen, Claudi L. H. Bockting

TL;DR
Adding narrative assessment to cognitive behavior therapy may reduce the risk of suicide attempts more effectively than therapy without it.
Contribution
This study is the first to show that narrative assessment in CBT significantly reduces suicide attempts compared to CBT without it.
Findings
CBT with narrative assessment reduced suicide attempts by 32% compared to controls.
CBT without narrative assessment showed no significant reduction in suicide attempts.
Interventions with narrative assessment had older participants and lower risk of bias.
Abstract
Are cognitive behavioral interventions that include a narrative assessment associated with a greater reduction in the risk of suicide attempts than those without? In this meta-analysis of 23 randomized clinical trials with 3262 participants, interventions incorporating a narrative assessment were associated with reduced suicide attempts, while those without were not. These findings suggest that including a narrative assessment may enhance the effectiveness of interventions in preventing suicide attempts. This systematic review and meta-analysis of randomized clinical trials examines the association between cognitive behavioral interventions with vs without a narrative assessment and risk of suicide attempt. There is currently no evidence-based method to identify the forces that may drive someone to attempt suicide. To examine whether cognitive behavior therapy (CBT) interventions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
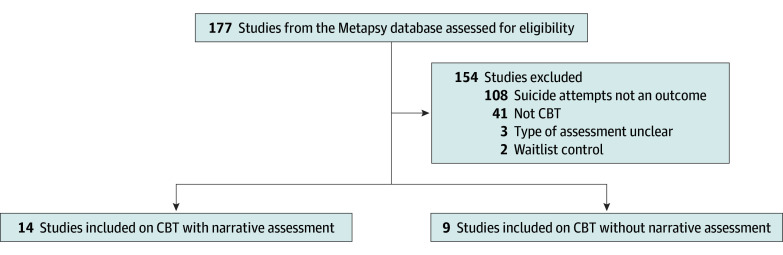 Figure 1
Figure 1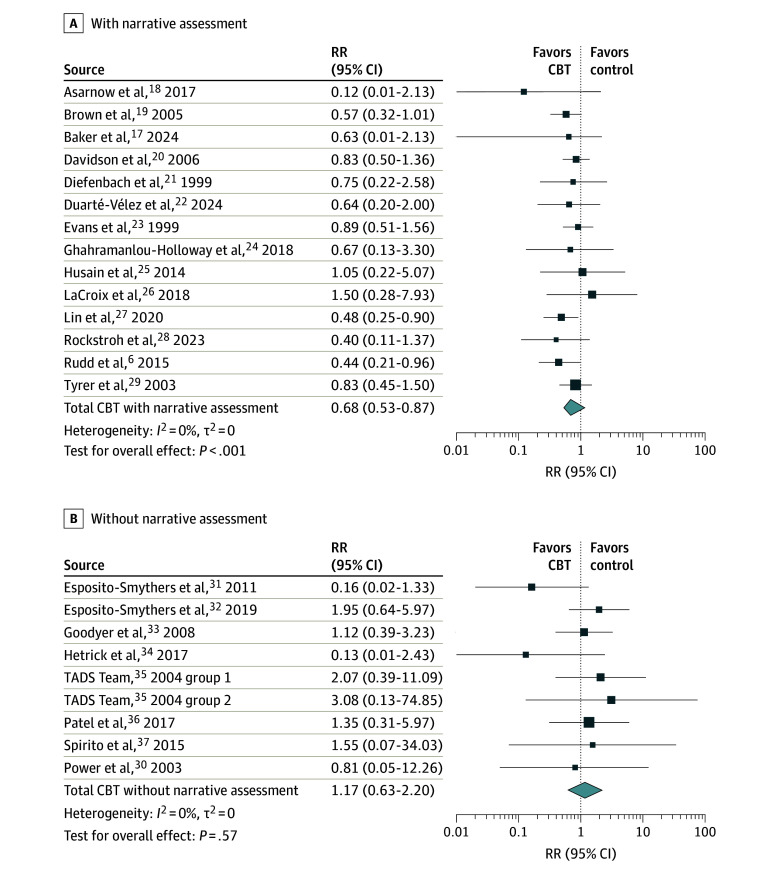 Figure 2
Figure 2| Variable | Narrative, mean (SD) | ||
|---|---|---|---|
| With | Without | ||
| Studies, No. | 14 | 9 | NA |
| Participants, No. | 1764 | 1498 | NA |
| Suicide attempts, No. | 258 | 52 | NA |
| Participant age, y | 27.08 (7.49) | 18.18 (9.82) | .03 |
| Sample size, No. | 58.86 (53.05) | 82.89 (68.44) | .36 |
| Event rate | 0.16 (0.14) | 0.05 (0.06) | .01 |
| Power | 0.24 (0.23) | 0.20 (0.17) | .68 |
| Study duration, wk | 27.38 (17.00) | 23.44 (17.69) | .79 |
| Treatment duration, sessions | 8.83 (3.96) | 12.87 (7.79) | .31 |
| Intervention type | |||
| Add-on, % | 46.67 | 37.50 | NA |
| Standalone, % | 53.33 | 62.50 | NA |
| Recruitment setting | |||
| Inpatient, % | 57, 14 | 22, 22 | NA |
| Partial hospitalization, % | 14, 29 | 11, 11 | |
| Outpatient, % | 35, 71 | 44, 44 | |
| Emergency department, % | 50, 00 | 00, 00 | |
| Primary care, % | 00, 00 | 11,11 | |
| School, % | 00, 00 | 11,11 | |
| Risk of bias | |||
| Randomization | 1.29 (0.47); low | 1.22 (0.44); low | .77 |
| Deviations | 1.36 (0.50); low | 1.56 (0.53); low | .38 |
| Missing data | 1.64 (0.93); low | 2.11 (1.05); some concern | .30 |
| Measurement | 1.50 (0.76); low | 1.38 (0.52); low | .90 |
| Reporting | 1.79 (0.70); low | 1.78 (0.67); low | .99 |
| Overall | 2.36 (0.50); some concern | 2.89 (0.33); some concern | .02 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSuicide and Self-Harm Studies · Mental Health via Writing · Posttraumatic Stress Disorder Research
Introduction
To reduce the risk of a suicide attempt, practitioners are often tasked with the challenge to identify the forces that might drive individuals to attempt suicide before they actually do. The only available method to aid clinicians in this task is the Collaborative Assessment and Management of Suicidality (CAMS^1^) framework, which has been specifically designed to identify suicidal drivers. Meta-analysis shows CAMS has a positive association with suicidal thoughts, hopelessness, and the therapeutic alliance, but does not reduce suicide attempts compared with controls.^2^ Although reducing suicidal thoughts and other risk factors for suicide is valuable, it remains uncertain whether this translates into the prevention of suicide attempts: ideation-to-action theories posit that both are influenced by different factors^3^ and interventions often decrease one or the other, not both.^2,4,5,6^ It is therefore important to develop new ways to identify risk and protective factors for suicide attempts and gear treatments toward their prevention.
Insights may be derived from the way in which interventions with proven efficacy in preventing suicide attempts select treatment targets. Brief cognitive behavior therapy for suicide prevention (BCBT)^6^ uses a procedure called a narrative assessment to this end, which also occurs in dialectical behavior therapy under the name chain analysis.^7^ During a narrative assessment, practitioner and patient first identify the specific moment in the past weeks in which the patient came closest to suicide (referred to as the index crisis or worst point). For someone who recently made a suicide attempt, the index crisis is this suicide attempt, for someone who has not made a suicide attempt, the index crisis is the moment at which they came closest to attempting suicide. Once the index crisis has been identified, the practitioner asks the patient to tell the story of this situation and practitioner and patient work together to gain a deeper understanding of the sequence of events, thoughts, emotions, and behaviors that lead up to this peak, including factors that helped delay or reduce it. The practitioner is careful to prevent the conversation from drifting toward issues that were not present during the index crisis.
This seems like a sensible approach to catch the factors in action that may one day drive a patient to make a (or another) suicide attempt. Preliminary support for the use of a narrative assessment comes from a study^8^ in which all participants were offered the same intervention, preceded by either a narrative assessment or a structured interview. Participants whose treatment began with the narrative assessment experienced fewer suicidal thoughts after their treatment than participants whose treatment started with the structured interview. However, the study did not examine the impact on suicide attempts. This study therefore aims to conduct a systematic review and meta-analysis, in which we investigate the association of comparable interventions with and without a narrative assessment with the incidence of suicide attempts.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline and was preregistered in PROSPERO (CRD42024604281). This systematic review and meta-analysis used the Metapsy.org Suicide Prevention database,^9^ a database of randomized clinical trials on psychological interventions, that is regularly updated on the basis of rigorous systematic reviews. This study used version 25.0.1, which will be released later this year and spans all trials up to April 2025, retrieved via PubMed, Embase, Web of science, Scopus, and the Cochrane Central Register of Controlled Trials. Unpublished studies and studies retrieved from the reference lists of relevant articles were also included. To construct and update the Metapsy database, 2 researchers independently searched and selected studies, extracted data from the trials, and assessed risk of bias. Any disagreements were resolved by discussion and, if necessary, in consultation with a third researcher. Decisions were recorded in Covidence. The full search string can be found in Supplement 1.
Study Selection
Studies were first screened for eligibility on titles and abstracts and then on full text. Studies were included in the MetaPsy database if they:
Had a randomized design comparing 2 or more groups;Reported suicide attempts, suicide, self-harm leading to hospitalization, or suicidal thoughts as an outcome (self-harm was only included if the study’s definition of self-harm included suicide attempts);Were written in English, Dutch, German, or Greek; andStudied a psychological intervention containing at least 1 psychotherapeutic technique.
For the purpose this systematic review and meta-analysis, studies were excluded if:
They only reported suicidal ideation, not suicide attempts;They studied psychological interventions other than cognitive behavioral therapy (CBT), since we wanted to limit variation between the groups, other than the presence or absence of a narrative assessment, and we expected there would be more studies on CBT than on other interventions;^10^They used a waiting list control, since this can lead to overestimation of effect sizes; orIt could not be established whether the intervention included a narrative assessment.
Data Extraction
The first author, year of publication, number of randomized participants, mean age of participants, percentage of females, setting, recruitment strategy, main Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) classification of participants, inclusion and exclusion criteria, type of psychotherapy, type of control condition, the number of suicide attempts, and effect size were recorded for each trial. In case any of these characteristics could not be extracted from the article, the authors were contacted twice via email before the data were considered unavailable. To limit the amount of variation between the interventions, other than the presence or absence of a narrative interview, trials of third-wave therapies and dialectical behavior therapy were excluded, although they are sometimes considered forms of CBT. For trials on CBT, researchers also recorded whether a narrative assessment was or was not included. If this information could not be extracted from the article, the corresponding and last author were each contacted via email once. Study characteristics were tabulated to assess their eligibility for each synthesis.
Risk of Bias Assessment and Data Preparation
During the construction and update of the Metapsy database, all studies were assessed for risk of bias by 2 researchers using version 2 of the Cochrane Collaboration Risk of Bias Tool for randomized trials, which assesses possible sources of bias due to the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results.Relative risk was calculated for each trial as an effect size.
Statistical Analysis
Mean age, sample size, number of sessions, study duration in weeks, and risk of bias were calculated for studies with and without a narrative assessment and compared using the Mann-Whitney U test. Three separate meta-analysis were conducted with the metapsyTools package in R (version 4.4.1) and R studio (version 2024.04.2 + 764) (R Project for Statistical Computing) and summarized in forest plots. First, the effect sizes of interventions with and without a narrative assessment were pooled in 2 separate meta-analyses. Both studies with and without a narrative assessment were then included in a third meta-analysis to directly compare their effect sizes in subgroup analysis.
Three-level models were estimated with effect sizes nested in studies to account for multiarm trials, applying robust variance estimation. We assumed an intrastudy correlation of 0.6. Relative risk ratios (RR) were pooled using the Mantel-Haenszel method to account for zero counts.. An RR of 0.90 to 0.70 was considered small; an RR of 0.69 to 0.50, medium; and an RR smaller than 0.50, large.^11^ Statistical significance was determined with a 2-sided *P *value of <.05
Prediction intervals, τ, the I^2^ statistic, and their 95% CIs were calculated as indicators of heterogeneity, with I^2^ values of 0%, 25%, 50%, and 75% considered to indicate no, low, moderate, and high heterogeneity, respectively.^12^ Outlier and influence analyses were performed if I^2^ was equal to or higher than 50%. The robustness of the findings was tested by (1) excluding outliers with a CI that did not overlap with that of the pooled effect size; (2) excluding influential cases according to the methods by Viechtbauer and Cheung^13^; (3) adjusting for publication bias with the limit meta-analysis method^14^; and (4) repeating the meta-analysis with studies with a low risk of bias.
Sensitivity analysis was performed to assess the influence of 4 factors, but only when at least 4 studies remained after accounting for the respective factor: (1) the exclusion of people with severe suicidal thoughts and behaviors from the trial,which might cause range restriction and other methodological issues; (2) age younger than 25 years, since interventions for young people tend to find smaller and more inconsistent results than interventions for adults^15^; (3) online interventions, since evidence that online interventions can be effective in preventing suicide attempts is sparse^16,17^; and (4) interventions with an above-average treatment length, since a quick treatment effect is of great importance in suicide prevention and longer treatments have been found to be somewhat more effective than shorter treatments.^10^ Differences in treatment length might therefore affect the outcomes of the meta-analysis.
Results
Study Selection
Figure 1 shows a flowchart of the study selection with reasons for exclusion. A total of 23 randomized clinical trials, with 3262 participants, were included in the meta-analysis. Of these, 14 studies incorporated a narrative assessment,^6,17,18,19,20,21,22,23,24,25,26,27,28,29^ and 9 studies did not include a narrative assessment.^30,31,32,33,34,35,36,37^
Study Selection FlowchartAbbreviations: CBT, cognitive behavioral therapy
Descriptive Statistics
Descriptive statistics and comparisons between studies with and without a narrative assessment are shown in the Table and Figure 2. The group of studies that incorporated a narrative assessment included 14 randomized clinical trials^6,17,18,19,20,21,22,23,24,25,26,27,28,29^with a total of 1764 participants. The group without a narrative assessment comprised 9 trials^30,31,32,33,34,35,36,37^ with a total of 1498 participants.
Association of CBT Interventions With and Without a Narrative Assessment With Risk of Suicide AttemptAbbreviations: RR, relative risk, TADS, Treatment for Adolescents With Depression Study
The mean age of participants in the studies without a narrative assessment was significantly lower than that of participants in the studies with a narrative assessment (mean [SD] age, 18.18 [9.82] years vs 27.08 [7.49] years; P = .02). The studies without a narrative assessment, vs those with a narrative assessment, also showed a slightly higher overall risk of bias (mean [SD] with some concerns, 2.89 [0.33] vs 2.36 [0.05]; P = .01) and had a lower event rate (mean [SD], 0.05 [0.06] vs 0.16 [0.14]; P = .01). Most studies on CBT with a narrative assessment recruited participants through inpatient facilities and emergency departments, whereas studies on CBT without a narrative assessments predominantly recruited participants through outpatient facilities, schools, and in primary care. Other variables, including sample size, study duration, and treatment length, did not differ significantly between the groups.
Meta-Analyses
Separate Meta-Analysis of CBT With a Narrative Assessment
CBT with a narrative assessment was associated with a significantly lower risk of suicide attempt compared with controls (RR, 0.68; 95% CI, 0.56-0.81; P < .001), with low heterogeneity between the 14 studies (1764 participants; τ = 0.00; 95% CI, 0.00-0.78; I^2^ = 0.00%; 95% CI, 0.00%-55.03%). The results of the meta-analysis remained unchanged when sensitivity analyses were conducted to account for outliers, influential cases, risk of bias, publication bias, age, the exclusion of people with severe suicidality, and online interventions. When excluding all studies with above-average treatment length, only 4 studies, with 207 participants, remained,^23,24,25,27^ and the finding was no longer statistically significant (RR, 0.69; 95% CI, 0.39-1.22; P = .13).
Separate Meta-Analysis of CBT Without a Narrative Assessment
CBT without a narrative assessment was not associated with the risk of suicide attempts (RR, 1.17; 95% CI, 0.63-2.20; P = .57). Again, heterogeneity between the 9 studies (with 1498 participants) was low (τ^2^ = 0; 95% CI, 0.00-1.71; I^2^ = 0.00%; 95% CI, 0.00%-64.80%), and the results were not impacted by accounting for outliers, influential cases, publication bias, risk of bias, online studies, and treatment length. When the 3 studies^33,35^ that excluded people with severe suicidality were removed from the analysis, the RR dropped below 1, but the result remained nonsignificant. Since only 1 of the studies^36^ without a narrative assessment was conducted among adults, it was not possible to conduct a sensitivity analysis for age or age group.
Comparison of CBT With and Without a Narrative Assessment in a Single Meta-Analysis
Together, CBT interventions with and without a narrative assessment were associated with a lower risk of suicide attempt (RR, 0.74; 95% CI, 0.58-0.93; P = .02). When subgroup analysis was conducted to compare CBT with and without a narrative assessment, a significant difference was found in favor of CBT with a narrative assessment (Q_1_ = 7.27, P = .007; I^2^ = 86%).
Discussion
The findings of this systematic review and meta-analysis indicate that CBT interventions incorporating a narrative assessment were associated with reduced risk of suicide attempts, with a medium effect size, suggesting that they are more impactful than CBT interventions without this component, which did not show a statistically significant result. These findings were robust across multiple sensitivity analyses.
The association between CBT with a narrative assessment and risk of suicide attempt became insignificant only when studies with an above average treatment length were excluded. However, this sensitivity analysis was based on just 4 studies, most of which had small sample sizes, and the findings should therefore be interpreted cautiously. Treatment length did not differ significantly between studies with and without a narrative component, suggesting that treatment duration alone cannot explain the difference in results. At the same time, the narrative component serves to identify rather than address treatment targets, and its impact is likely contingent on the intervention that follows. It may therefore be more impactful when sufficient treatment length is available to work through these identified targets.
To provide a more definitive answer to the question whether a narrative assessment can indeed improve the effectiveness of interventions, head-to-head comparisons are needed in which the impacts of identical interventions with and without a narrative assessment on suicide or suicide attempts (not suicidal ideation) are directly compared in randomized clinical trials. It may also be valuable to examine factors that influence the effectiveness of a narrative assessment. While a window of 4 weeks or less since a suicide attempt appears both workable and clinically meaningful,^39^ it remains uncertain whether a longer interval would still yield useful insights. This may differ between suicidal ideation and suicidal behavior: an instance of behavior may be easier to recall and reconstruct than an instance of thoughts or feelings. A related question is whether a narrative assessment based on an index episode of relatively mild ideation can adequately capture the processes that may eventually culminate in a suicide attempt, or whether such dynamics become visible only during episodes of more severe suicidal thoughts and behaviors. Finally, it seems plausible that a narrative assessment is more impactful when followed by a personalized treatment that can be tailored to the personal dynamics revealed through the interview, such as BCBT, rather than when embedded in a standardized, one-size-fits-all approach.
Limitations
This study has limitations. It is important to realize that none of the studies in this meta-analysis were designed to isolate the effects of a narrative assessment. Although the included studies were all randomized clinical trials, any associations found in this meta-analysis are therefore associational, not necessarily causal, and can be influenced by several confounders.
Three such confounders were identified, one of which was a difference in the age of participants in studies with and without a narrative assessment: almost all studies on CBT with a narrative assessment were conducted among adults, while most studies on CBT without a narrative assessment focused on adolescents and young adults. This represents a major limitation of the literature, as studies involving younger populations often report smaller and more inconsistent effects,^15^ perhaps because most psychotherapies are directed at the individual, whereas the difficulties of young people are more often contextually and relationally driven.^38^ Consequently, the difference in participant age may have contributed to the larger uncertainty surrounding the outcomes associated with CBT without a narrative assessment and potentially led to an underestimation of the effect size of CBT without a narrative assessment. This may in turn be due to studies involving young people employing more stringent control conditions or safety protocols. However, the level of detail in the majority of studies does not permit this hypothesis to be adequately examined.
Apart from the difference in age, the event rate was significantly lower in studies without a narrative assessment, probably due to differences in the recruitment sites used. This limits the power to detect intervention effects in these trials. The overall risk of bias in studies without a narrative assessment was slightly higher but still fell within the same category of some concerns as the studies with a narrative assessment, suggesting that this difference is likely negligible.
Conclusions
In this systematic review and meta-analysis of CBT interventions, CBT with a narrative assessment was associated with a reduced risk of suicide attempt, whereas CBT without this component was not. In light of this uncertainty, clinicians may do well to use CBT protocols that include a narrative assessment, such as the BCBT protocol from Bryan and Rudd.^40^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jobes DA. Managing Suicidal Risk: A Collaborative Approach. 3rd ed. The Guilford Press;2006.
- 2Swift JK, Trusty WT, Penix EA. The effectiveness of the Collaborative Assessment and Management of Suicidality (CAMS) compared to alternative treatment conditions: a meta-analysis. Suicide Life Threat Behav. 2021;51(5):882-896. doi:10.1111/sltb.1276533998028 · doi ↗ · pubmed ↗
- 3Klonsky ED, Dixon-Luinenburg T, May AM. The critical distinction between suicidal ideation and suicide attempts. World Psychiatry. 2021;20(3):439-441. doi:10.1002/wps.2090934505359 PMC 8429339 · doi ↗ · pubmed ↗
- 4De Cou CR, Comtois KA, Landes SJ. Dialectical behavior therapy is effective for the treatment of suicidal behavior: a meta-analysis. Behav Ther. 2019;50(1):60-72. doi:10.1016/j.beth.2018.03.00930661567 · doi ↗ · pubmed ↗
- 5Nuij C, van Ballegooijen W, de Beurs D, . Safety planning-type interventions for suicide prevention: meta-analysis. Br J Psychiatry. 2021;219(2):419-426. doi:10.1192/bjp.2021.5035048835 · doi ↗ · pubmed ↗
- 6Rudd MD, Bryan CJ, Wertenberger EG, . Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: results of a randomized clinical trial with 2-year follow-up. Am J Psychiatry. 2015;172(5):441-449. doi:10.1176/appi.ajp.2014.1407084325677353 · doi ↗ · pubmed ↗
- 7Borges LM, Nazem S, Matarazzo BB, Barnes SM, Wortzel HS. Therapeutic risk management: chain analysis of suicidal ideation and behavior. J Psychiatr Pract. 2019;25(1):46-53. doi:10.1097/PRA.000000000000035830633732 · doi ↗ · pubmed ↗
- 8Lohani M, Bryan CJ, Elsey JS, . Collaboration matters: A randomized controlled trial of patient-clinician collaboration in suicide risk assessment and intervention. J Affect Disord. 2024;360:387-393. doi:10.1016/j.jad.2024.06.00438838788 · doi ↗ · pubmed ↗