Pharmacoequity in Anticoagulation Among Medicare Patients With Venous Thromboembolism
Amina A. Alkhalaf, Sungho Bea, Geetha S. Iyer, Julie C. Lauffenburger, Katsiaryna Bykov

TL;DR
The study examines how race and ethnicity affect whether Medicare patients with blood clots receive recommended anticoagulant treatments.
Contribution
The study provides new evidence on racial and ethnic disparities in anticoagulant prescribing among Medicare patients with venous thromboembolism.
Findings
Race and ethnicity are associated with the likelihood of receiving guideline-recommended direct oral anticoagulants.
Disparities persist even after adjusting for clinical and socioeconomic factors.
Abstract
This cohort study investigates the association of race and ethnicity with initiation of guideline-recommended direct oral anticoagulants in Medicare beneficiaries with venous thromboembolism.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Patients, No. (%) (N = 204 679) | Absolute standardized difference vs White | |||
|---|---|---|---|---|---|
| Black or African American (n = 22 139) | Hispanic (n = 2942) | White (n = 179 598) | Black or African American | Hispanic | |
| Demographics | |||||
| Age, mean (SD), y | 77.1 (8.0) | 79.4 (8.6) | 77.3 (7.7) | 0.02 | 0.27 |
| Gender | |||||
| Female | 14 835 (67.0) | 1985 (67.5) | 107 472 (59.8) | 0.15 | 0.16 |
| Male | 7304 (33.0) | 957 (32.5) | 72 126 (40.2) | ||
| Medicare dual status | |||||
| Partial dual | 2716 (12.3) | 323 (11.0) | 7680 (4.3) | 0.29 | 0.26 |
| Full dual | 7727 (34.9) | 2111 (71.8) | 19 652 (10.9) | 0.6 | 1.57 |
| Index event | |||||
| Deep vein thrombosis | 8485 (38.3) | 1470 (50.0) | 58 519 (32.6) | 0.12 | 0.36 |
| Pulmonary embolism | 13 654 (61.7) | 1472 (50.0) | 121 079 (67.4) | 0.12 | 0.34 |
| Bleeding history and bleeding risk | |||||
| Any prior visit for bleeding | 6736 (30.4) | 919 (31.2) | 53 873 (30.0) | 0.01 | 0.03 |
| HAS-BLED score, mean (SD) | 2.6 (0.7) | 2.5 (0.7) | 2.4 (0.7) | 0.38 | 0.26 |
| Comorbidities | |||||
| Atrial fibrillation | 3146 (14.2) | 427 (14.5) | 34 221 (19.1) | 0.13 | 0.12 |
| Congestive heart failure | 8378 (37.8) | 1030 (35.0) | 51 556 (28.7) | 0.2 | 0.14 |
| Chronic kidney disease | 7692 (34.7) | 807 (27.4) | 43 537 (24.2) | 0.23 | 0.07 |
| Diabetes | 11 330 (51.2) | 1634 (55.5) | 58 731 (32.7) | 0.38 | 0.47 |
| Cancer | 4856 (21.9) | 515 (17.5) | 39 895 (22.2) | 0.01 | 0.12 |
| Combined comorbidity score, mean (SD) | 5 (3.4) | 4.7 (3.4) | 4.3 (3.2) | 0.22 | 0.13 |
| Frailty score, mean (SD) | 0.2 (0.1) | 0.3 (0.1) | 0.2 (0.1) | 0.25 | 0.37 |
| Baseline medications | |||||
| Antiplatelets | 2853 (12.9) | 399 (13.6) | 19 350 (10.8) | 0.07 | 0.09 |
| H2 antagonists | 2840 (12.8) | 465 (15.8) | 16 430 (9.1) | 0.12 | 0.2 |
| Proton pump inhibitors | 8562 (38.7) | 1487 (50.5) | 69 918 (38.9) | 0.01 | 0.24 |
| Nonsteroidal anti-inflammatory drugs | 5577 (25.2) | 969 (32.9) | 38 791 (21.6) | 0.09 | 0.26 |
| Health care use: No. physician visits, mean (SD) | 41.6 (35.8) | 42.3 (34.0) | 39 (31.1) | 0.08 | 0.1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Atrial Fibrillation Management and Outcomes · Acute Myocardial Infarction Research
Introduction
Every year, more than 1 million US individuals experience venous thromboembolism (VTE),^1^ with higher VTE and mortality rates in Black patients suggesting disparities in care.^2^ While differences in uptake of direct oral anticoagulants (DOACs), which have replaced warfarin as the preferred treatment,^3^ have been observed in atrial fibrillation,^4,5^ little is known about patterns of DOAC adoption across racial and ethnic populations in VTE. We examined pharmacoequity, defined as equitable access to guideline-recommended medications regardless of race, ethnicity, gender, socioeconomic status, or geography, in DOAC use among Medicare beneficiaries with VTE.
Methods
This cohort study was approved by the Mass General Brigham institutional review board and deemed exempt from consent because data were deidentified. This report follows the STROBE reporting guideline. We used Medicare fee-for-service claims (January 1, 2013, to December 31, 2022) to identify individuals aged 65 years or older who initiated an oral anticoagulant (warfarin, dabigatran, rivaroxaban, apixaban, or edoxaban) within 30 days of a VTE hospitalization and after at least 1 year of continuous Medicare Part A, B, and D coverage (eTable 1 in Supplement 1).
Exposure was Medicare-reported race and ethnicity obtained from the Social Security Administration. We analyzed Black, Hispanic, and White patients; individuals in other race categories (American Indian or Alaska Native and Asian or Pacific Islander) were excluded due to small numbers. The outcome was initiation of a DOAC vs warfarin. Multivariable logistic regression estimated odds ratios (ORs) for DOAC initiation in Black and Hispanic patients compared with White patients adjusting for 78 baseline covariates selected a priori for their association with anticoagulant prescribing and health care use (eTable 2 in Supplement 1). Demographics (age, sex, state of residence, and dual eligibility status) were captured at the index date. Analyses were conducted for the overall period and stratified into 2013 to 2015, 2016 to 2018, and 2019 to 2022. Cohorts were created using Aetion Evidence Platform version 4.53; analyses were conducted in June 2025 using SAS version 9.4 (SAS Institute).
Results
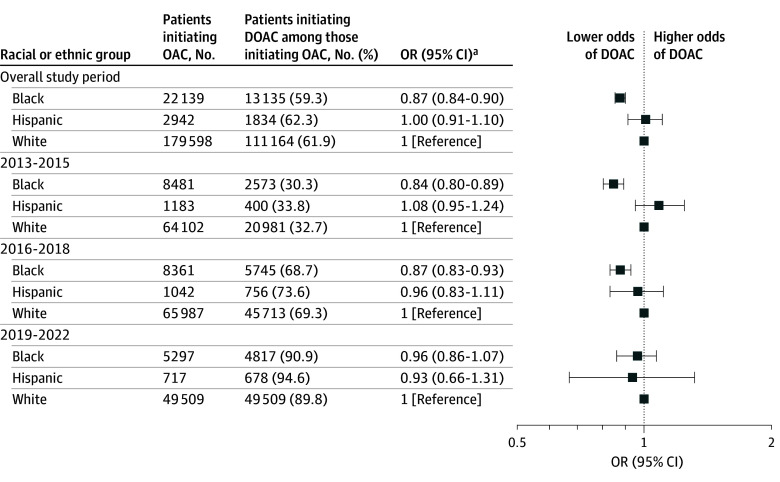
Among 204 679 study-eligible individuals (22 139 Black [10.8%], 2942 Hispanic [1.4%], and 179 598 White [87.7%]; mean [SD] age, 77.3 [7.7] years; 124 292 female [60.7%]) (Table), 61.9% of White, 59.3% of Black, and 62.3% of Hispanic patients initiating anticoagulation were started on DOACs. Adjusted odds of DOAC initiation were lower in Black vs White patients overall (OR, 0.87; 95% CI, 0.84-0.90), in 2013 to 2015 (OR, 0.84; 95% CI, 0.80-0.89), and 2016 to 2018 (OR, 0.87; 95% CI, 0.83-0.93) but not in 2019 to 2022 or for Hispanic vs White patients throughout the study period (Figure).
Odds of Direct Oral Anticoagulant (DOAC) Treatment by Race and EthnicityTreatment with DOACs is shown across racial and ethnic groups in Medicare beneficiaries initiating oral anticoagulants after venous thromboembolism. OAC indicates oral anticoagulant; OR, odds ratio.aAdjusted for all baseline covariates, including calendar year.
Discussion
This cohort study found that Black patients had lower odds of being initiated on DOACs than White patients, especially during the early period of DOAC uptake. There was no difference in DOAC initiation odds between Hispanic and White patients. Our findings for Black patients are consistent with studies in atrial fibrillation^4,5^; however, DOAC adoption was similar in Hispanic and White patients in our study. Although absolute differences were small, even modest inequities can carry public health consequences given the high VTE incidence.
Our findings align with those of Nathan et al^6^ but expand generalizability by analyzing an older Medicare population in more recent years. In addition, we adjusted for a wide range of characteristics, ensuring comprehensive control for baseline differences.
Study limitations include the lack of information on patient or physician treatment preferences, prescriber-level factors, and other social factors influencing OAC choice, such as health literacy and cost. Medicare data combine race and ethnicity, and claims reflect dispensing rather than prescribing or use, which may result in misclassification. In addition, we did not assess disparities in anticoagulation initiation, including noninitiation due to nonadherence or a clinical decision not to treat. Moreover, findings may not be generalizable to other populations. Early adoption gaps found in this study suggest potential racial and ethnic disparities in access to newer pharmacotherapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Virani SS, Alonso A, Aparicio HJ, ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e 254-e 743. doi:10.1161/CIR.000000000000095033501848 PMC 13036842 · doi ↗ · pubmed ↗
- 2Giorgio K, Walker RF, Mac Lehose RF, . Venous thromboembolism mortality and trends in older US adults, 2011-2019. Am J Hematol. 2023;98(9):1364-1373. doi:10.1002/ajh.2699637366276 PMC 10529371 · doi ↗ · pubmed ↗
- 3Iyer GS, Tesfaye H, Khan NF, Zakoul H, Bykov K. Trends in the use of oral anticoagulants for adults with venous thromboembolism in the US, 2010-2020. JAMA Netw Open. 2023;6(3):e 234059. doi:10.1001/jamanetworkopen.2023.405936947039 PMC 10034573 · doi ↗ · pubmed ↗
- 4Reynolds KR, Khosrow-Khavar F, Dave CV. Racial and ethnic disparities in initiation of direct oral anticoagulants among Medicare beneficiaries. JAMA Netw Open. 2024;7(5):e 249465. doi:10.1001/jamanetworkopen.2024.946538709533 PMC 11074810 · doi ↗ · pubmed ↗
- 5Essien UR, Kim N, Hausmann LRM, . Disparities in anticoagulant therapy initiation for incident atrial fibrillation by race/ethnicity among patients in the Veterans Health Administration System. JAMA Netw Open. 2021;4(7):e 2114234. doi:10.1001/jamanetworkopen.2021.1423434319358 PMC 8319757 · doi ↗ · pubmed ↗
- 6Nathan AS, Geng Z, Dayoub EJ, . Racial, ethnic, and socioeconomic inequities in the prescription of direct oral anticoagulants in patients with venous thromboembolism in the United States. Circ Cardiovasc Qual Outcomes. 2019;12(4):e 005600. doi:10.1161/CIRCOUTCOMES.119.00560030950652 PMC 9119738 · doi ↗ · pubmed ↗