Early experience with pulsed field ablation for atrial fibrillation in Central Asia: A case series
Ayan Abdrakhmanov, Zhansaya Yerkhanova, Serge Boveda, Zhanar Abdrakhmanova, Assel Chinybayeva, Bibigul Adilbekova, Zhanasyl Suleymen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
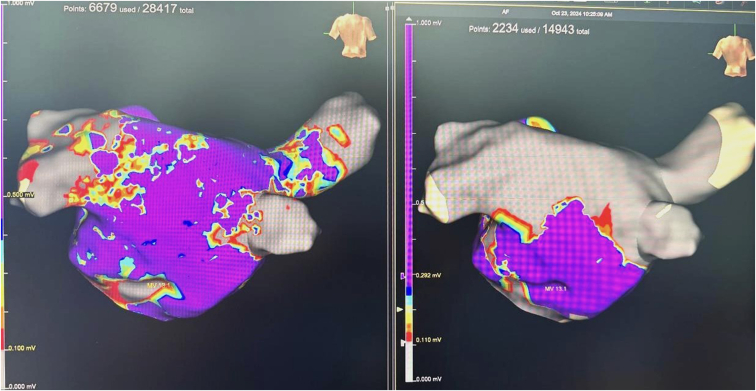 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Cardiac electrophysiology and arrhythmias
Key Findings
- ▪To our knowledge, this is the first reported case series of pulsed field ablation (PFA) for atrial fibrillation in Central Asia.
- ▪All patients remained in sinus rhythm at 3- and 6-month follow-up.
- ▪In patients with heart failure with mildly reduced ejection fraction, PFA led to improved left ventricular function and reduced left atrial volume index.
- ▪No atrial fibrillation recurrence or significant arrhythmias occurred during follow-up.
Pulsed field ablation (PFA) is a novel, nonthermal ablation modality increasingly used for the treatment of atrial fibrillation (AF)1, with a favorable safety profile and promising efficacy demonstrated in large multicenter studies.2, 3, 4 However, data from resource-constrained regions, particularly Central Asia, remain scarce.
We report preliminary outcomes from 14 consecutive patients who underwent PFA for symptomatic, drug-refractory paroxysmal or persistent AF at our institution between January 2024 and January 2025. The FARAPULSE PFA system (Boston Scientific, Marlborough, MA) was used in all procedures. Pulmonary vein isolation was successfully achieved in 100% of cases without major procedural complications, including stroke, esophageal injury, phrenic nerve palsy, or vascular events.
Additionally, for patients with persistent and long-standing persistent AF, supplemental linear ablation using the FARAWAVE catheter was performed in the roof and posterior wall of the left atrium (Figure 1).Figure 1. Preablation and postablation 3-dimensional electroanatomic mapping posterior wall ablation after multiple PVIs using PFA in persistent AF. AF = atrial fibrillation; PFA = pulsed field ablation; PVI = pulmonary vein isolation.
At 3- and 6-month follow-up, all patients remained in sinus rhythm as confirmed by Holter monitoring and clinical assessment. In a subgroup of patients with heart failure with mildly reduced ejection fraction (n = 4), transthoracic echocardiography demonstrated a mean improvement in left ventricular ejection fraction from 44.8% to 52.8%. In addition, the mean left atrial volume index decreased from 45.8 mL/m^2^ to 42.2 mL/m^2^ after PFA (Table 1). No patients experienced AF recurrence or significant arrhythmias during the follow-up period.Table 1. Echocardiographic outcomes in patients with HFmrEF after PFAPatientLA volume index before PFA (mL/m^2^)LA volume index after PFA (mL/m^2^)EF before PFA (%)EF after PFA (%)134.434.24862263.060.04548345.745.04248440.129.44453EF = ejection fraction; HFmrEF = heart failure with mildly reduced ejection fraction; LA = left atrial; PFA = pulsed field ablation.
Our experience aligns with the safety and efficacy outcomes reported in recent large studies, such as the MANIFEST-17K registry2 and the ADVENT trial3, which demonstrated high procedural success rates and low complication rates with PFA. Importantly, our findings suggest that PFA can be safely and effectively implemented in health-resource-constrained environments, providing a valuable alternative for patients with complex arrhythmia profiles, including those with structural heart disease and previous ablation failures.
In conclusion, PFA seems to be a feasible, safe, and effective ablation strategy for AF in Central Asia, including in patients with comorbid heart failure and ablation history.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pierucci N.Mariani M.V.Laviole D.Pulsed field energy in atrial fibrillation ablation: from physical principles to clinical applications J Clin Med 1310202429803879252010.3390/jcm 13102980 PMC 11121906 · doi ↗ · pubmed ↗
- 2Ekanem E.Neuzil P.Safety of pulsed field ablation in over 17,000 patients: The MANIFEST-17K study Nat Med 3072024202020293897791310.1038/s 41591-024-03114-3PMC 11271404 · doi ↗ · pubmed ↗
- 3Reddy V.Y.Gerstenfeld E.P.Natale A.Pulsed field or conventional thermal ablation for paroxysmal AF—the ADVENT trial N Engl J Med 389182023166016713763414810.1056/NEJ Moa 2307291 · doi ↗ · pubmed ↗
- 4Reichlin T.Kueffer T.Badertscher P.Pulsed field ablation for persistent AF—The CHAMPION-AF Trial N Engl J Med 2024