Atraumatic Spleen Rupture: A Rare Fatal Complication of Dengue Hemorrhagic Fever
Harsha Vardhini, Magesh Murali

TL;DR
This paper reports two rare cases of spleen rupture without trauma in patients with severe dengue, highlighting the challenges in managing such life-threatening complications.
Contribution
The paper presents two rare clinical cases of atraumatic splenic rupture in dengue hemorrhagic fever, emphasizing management strategies and outcomes.
Findings
Atraumatic splenic rupture can occur in dengue hemorrhagic fever without external injury.
Non-operative management was successful in one patient but failed in another despite aggressive interventions.
Clinical response during resuscitation influenced the decision for conservative versus interventional management.
Abstract
Dengue is a common tropical infection in Southeast Asian countries, with clinical severity ranging from a self-limited acute febrile illness lasting 3-5 days to severe disease with a wide spectrum of complications. These complications can include extensive shock, coagulopathy, hemorrhage, multi-organ dysfunction, and death. In this case report, we describe two cases of atraumatic splenic rupture occurring in the context of dengue hemorrhagic fever. In these two patients, non-traumatic rupture of the spleen occurred in the absence of any external injury, with positive dengue signs and serology. The major clinical challenges in managing these patients were hypovolemic shock, thrombocytopenia, and coagulopathy. Both cases were managed non-operatively, with an emphasis on organ preservation. The first patient responded well to aggressive resuscitative efforts, was closely monitored for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
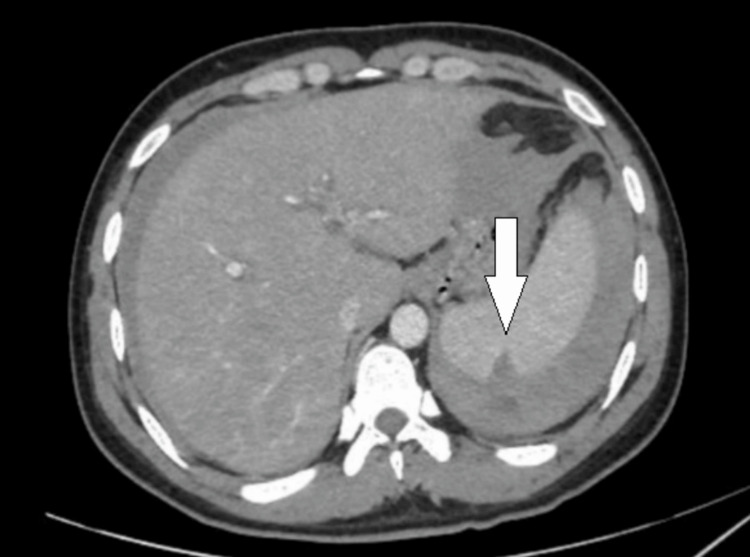 Figure 1
Figure 1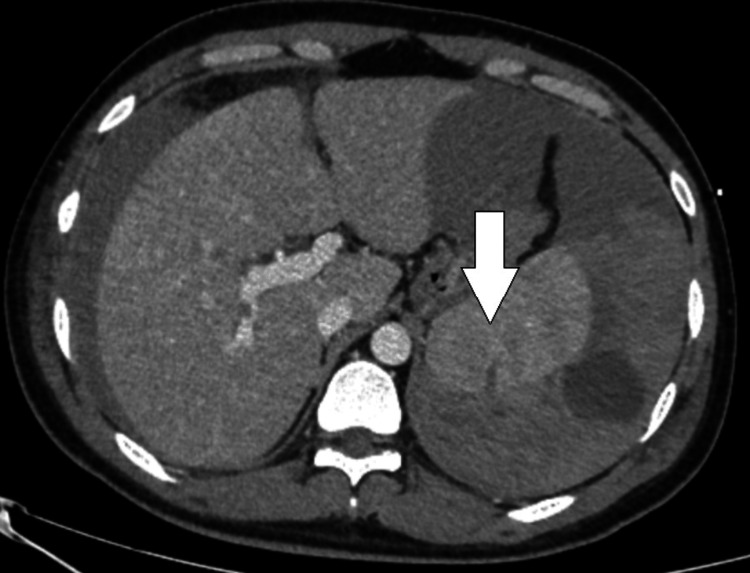 Figure 2
Figure 2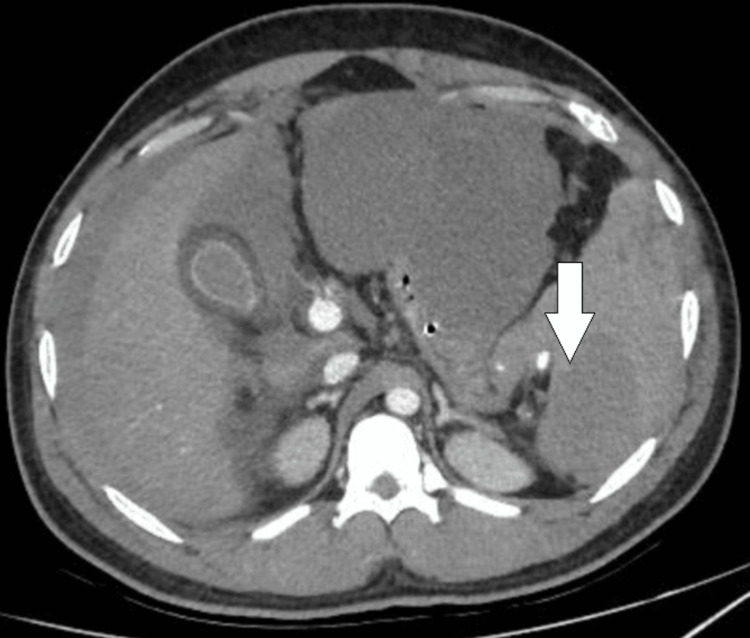 Figure 3
Figure 3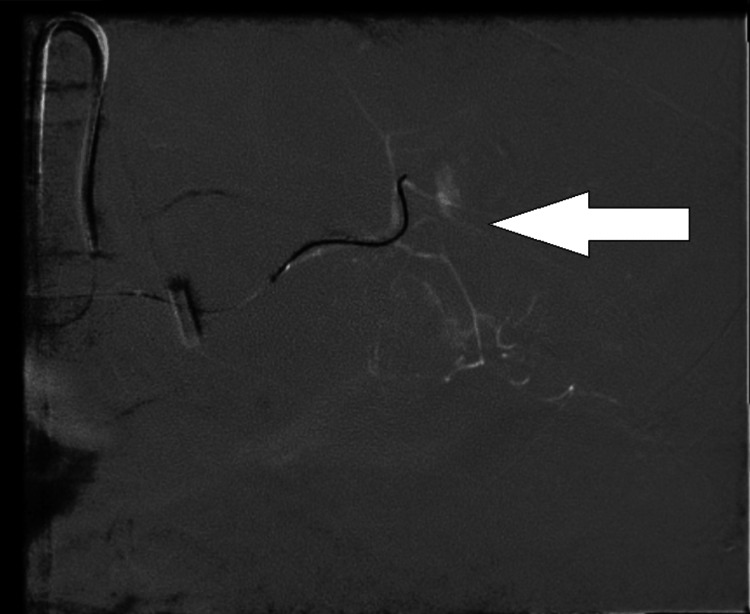 Figure 4
Figure 4| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day of Discharge | Reference Range | |
| Hemoglobin (g/dL) | 13.7 | 10.5 | 9.2 | 8.1 | 7.7 | 8.4 | 10.3 | 13.2 - 16.6 |
| Total count (10^3/microliter) | 4.96 | 9.31 | 4.97 | - | - | - | - | 4 - 11 |
| Platelet (10^3/microliter) | 42 | 44 | 96 | 104 | 110 | 137 | 161 | 150 - 450 |
| Packed cell volume | 40.6% | - | - | - | - | - | 31.6 | 40% - 54% |
| Prothrombin time (seconds) | 12.4 | - | - | 11.5 | - | - | - | 11 - 13.5 |
| INR | 1.03 | - | - | 0.96 | - | - | - | 0.8 - 1.1 |
| APTT (seconds) | 37.9 | - | - | 32.9 | - | - | - | 25 - 35 |
| Total bilirubin (mg/dL) | 0.31 | - | - | - | - | - | - | 0.1 - 1.2 |
| AST (U/L) | 835 | - | - | - | - | 194 | - | 5 - 40 |
| ALT (U/L) | 432 | - | - | - | - | 241 | - | 7 - 56 |
| Fibrinogen (mg/dL) | 223 | - | - | - | - | - | - | 200 - 400 |
| Serum ferritin (ng/mL) | 11368.9 | - | - | - | - | - | - | 30 - 400 |
| Serum triglycerides (mg/dL) | 187 | - | - | - | - | - | - | < 150 |
| Day 1 | Day 2 | Day 3 | Reference Range | |
| Hemoglobin (g/dL) | 7.8 | 4.3 | 6.8 | 13.2 - 16.6 |
| Total count (10^3/microliter) | 20.84 | - | 18.35 | 4 - 11 |
| Platelet (10^3/microliter) | 104 | 29 | 55 | 150 - 450 |
| Packed cell volume | 26.7% | 14.4 | - | 40% - 54% |
| Prothrombin time (seconds) | 17.9 | - | 25.6 | 11 - 13.5 |
| INR | 1.51 | - | 2.18 | 0.8 - 1.1 |
| APTT (seconds) | 109.6 | - | 60.8 | 25 - 35 |
| Total bilirubin (mg/dL) | 0.31 | - | - | 0.1 - 1.2 |
| AST (U/L) | 4002 | - | 14818 | 5 - 40 |
| ALT (U/L) | 3749 | - | 4523 | 7 - 56 |
| Fibrinogen (mg/dL) | 123 | - | 153 | 200 - 400 |
| Serum ferritin (ng/mL) | 40001 | - | - | 30 - 400 |
| Serum triglycerides (mg/dL) | 187 | - | - | < 150 |
| Serum Urea (mg/dL) | 53 | 41 | - | 7 - 20 |
| Serum creatinine (mg/dL) | 2.76 | 2.79 | - | 0.6 - 1.3 |
| WSES Class | Injury Description | Hemodynamic Status |
| Class I (Mild) | Minor splenic injuries without major vascular involvement | Hemodynamically stable |
| Class II (Moderate) | Moderate splenic injuries with limited vascular involvement | Hemodynamically stable |
| Class III (Moderate) | More extensive splenic injuries, possibly with segmental vascular injury | Hemodynamically stable with potential signs of instability |
| Class IV (Severe) | Severe splenic injuries with major vascular involvement or a shattered spleen | Hemodynamically unstable |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Case Reports on Hematomas · Trauma Management and Diagnosis
Introduction
Dengue fever is a common arthropod-borne viral infection caused by the Flavivirus genus. It is a single-stranded RNA virus with four distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4 [1]. Dengue remains a significant public health concern, with nearly 5.9 million cases reported globally in 2019, predominantly affecting populations in Southeast Asian countries [2]. The disease is transmitted to humans through the bite of the female Aedes mosquito, which breeds in man-made water reservoirs typically found at the household level. After an extrinsic incubation period of 8 to 10 days within the mosquito, the virus becomes transmissible, and the intrinsic incubation period in humans ranges from 4 to 7 days.
The pathogenesis of dengue involves direct viral injury and immune-mediated cellular damage, leading to endothelial dysfunction, macrophage activation, and platelet destruction. These processes result in vasculopathy, coagulopathy, cytopathy, and organ dysfunction, collectively defining severe dengue [3].
Dengue hemorrhagic fever with shock is one of the severe manifestations of the disease. Common bleeding manifestations in dengue include epistaxis, hematemesis, melena, hematuria, and menorrhagia, with intracranial and retroperitoneal hemorrhages being rare [4].
Splenic involvement with subcapsular hematoma is an uncommon complication, reported in approximately 1.5% of all dengue cases [5,6]. Due to the rarity of the complication, it is difficult to diagnose unless clinicians have a very high index of suspicion. Only a few case reports describe this rare presentation and hence, there is no clear consensus or guidelines to approach this complication.
In this report, we present two cases of spontaneous splenic rupture secondary to dengue-associated coagulopathy. Both patients presented to the emergency department with clinical features consistent with severe dengue. While dengue fever complicated by coagulopathy and hemorrhagic shock is not uncommon, splenic rupture in the setting of severe dengue is a rare clinical presentation [5-7]. We highlight the challenges encountered and the management strategies implemented following complex clinical decision-making. Management differed based on clinical progression: one case was managed conservatively with close monitoring, while the other required definitive intervention with splenic artery embolization.
Case presentation
Case 1
A 33-year-old man with no known comorbidities presented to the Emergency Department with a five-day history of fever associated with chills, headache, myalgia, and abdominal pain localized to the left upper quadrant for one day. He was previously evaluated at an outside facility and found to be dengue NS1 positive. The patient was triaged to the red zone of the Emergency department as his National Early Warning Score 2 (NEWS2) score was 13 [8]. On examination in the Emergency Department, the patient was tachycardic (110 beats per minute), hypotensive (89/60 mmHg), and had an elevated lactate level of 4.1 mmol/L. Abdominal examination revealed severe tenderness in the left hypochondrium with diffuse guarding and rigidity. Point-of-care ultrasound showed free fluid in the splenorenal space and a perisplenic collection.
A contrast-enhanced computed tomography (CECT) scan of the abdomen revealed splenomegaly with a 1.7 cm splenic laceration, a subcapsular hematoma measuring 8.3 × 2.6 × 2.9 cm, and hemoperitoneum. Additionally, hepatomegaly and pleural effusion were noted (Figure 1). The patient was stabilized in the Emergency Department. Due to the need for intensive monitoring and anticipation of deterioration, he was admitted to the intensive care unit (ICU) for further management.
CECT abdomen on day 1 CECT: Contrast-enhanced computed tomography
In the ICU, he was supported with non-invasive positive pressure ventilation, bilevel positive airway pressure (BiPAP), due to respiratory distress. Early pulmonary edema secondary to fluid resuscitation and blood transfusion versus acute respiratory distress syndrome (ARDS) were considered as differentials for the respiratory distress. The patient presented with B-lines and a minimal pleural effusion on a point-of-care ultrasound (POCUS) examination in the ICU. Fluid administration, blood transfusion, and vasopressor support were optimized carefully after regular hemodynamic assessments of the patient. Initial laboratory investigations revealed thrombocytopenia, elevated liver enzymes, and increased ferritin levels (Table 1). Following the discussion of the multidisciplinary team consisting of an intensivist, a surgeon, and an interventional radiologist, conservative management of the splenic rupture was chosen, as there was no active contrast extravasation on the CECT scan. Hourly vitals were checked, and sixth hourly monitoring of hemoglobin, hematocrit, platelets, and blood gas was done. He was transfused blood products accordingly to maintain his hemoglobin and platelet counts. The massive transfusion protocol was not followed for this patient.
The platelet counts gradually improved from 42,000 per microlitre on day 1 to 104,000 per microlitre on day 4. A repeat abdominal scan was performed on day 4, showing a decrease in the size of the hematoma (Figure 2). By day six, the patient was weaned off ICU care and transferred to the general ward, remaining clinically and hemodynamically stable with recovery from dengue shock syndrome.
CECT abdomen on day 4, showing a decrease in the size of the hematomaCECT: Contrast-enhanced computed tomography
Case 2
A 23-year-old man with no significant past medical history presented with a four-day history of fever and headache, vomiting for two days, and breathlessness for one day. He tested weakly positive for dengue IgM and had thrombocytopenia (platelet count: 68 × 10³/μL) at an outside hospital. The patient was brought to our hospital unresponsive. He was directly triaged to the red zone of the Emergency department. Cardiopulmonary resuscitation (CPR) was initiated per ACLS protocol. In the first two rhythm checks, asystole was noted, and the subsequent 4 rhythm checks showed pulseless electrical activity. IV adrenaline was administered every 3-5 minutes. Return of spontaneous circulation (ROSC) was achieved after six cycles. Post-ROSC, the patient was intubated and resuscitated with IV fluids as he was dehydrated. He was started on vasopressors due to worsening shock.
A nasogastric (Ryle’s) tube aspirate showed coffee ground material, and the patient exhibited progressive metabolic acidosis and severe shock. Severe dengue hemorrhagic shock was suspected, and the management was started in line with dengue hemorrhagic shock. Due to hemodynamic instability, need for respiratory support, and intensive monitoring, the patient was admitted to the critical care unit for further management.
In the ICU, lung-protective ventilation was continued along with fluid resuscitation, massive transfusion of blood products, vasopressor therapy, and continuous renal replacement therapy. POCUS revealed free fluid in the abdomen. Definitive radiological investigation was deferred on day one as the patient was too critical to be shifted for investigation. On day two of ICU stay, a CECT scan of the abdomen demonstrated active, progressive arterial contrast extravasation in the gastrosplenic region with moderate hemoperitoneum, likely arising from splenic arterial branches, along with a non-enhancing loculated fluid collection along the greater curvature of the stomach (Figure 3). Splenic artery angioembolization was performed to control ongoing hemorrhage (Figure 4).
CECT abdomen on day 2CECT: Contrast-enhanced computed tomography
Angio-embolization of the splenic artery
The patient's laboratory investigations revealed a worsening AST/ALT level suggestive of shock liver/ dengue hepatitis (Table 2). Though the patient's lab values did not categorize into overt disseminated intravascular coagulation, the corresponding parameters were worsening. These findings were considered to be a part of the multi-organ dysfunction of the patient's illness.
Despite aggressive supportive measures, the patient’s shock worsened, and he ultimately succumbed to his illness on day 3 of hospitalization.
Discussion
Dengue is a dynamic illness characterized by three phases: the acute febrile phase (1-3 days), the critical phase (4-6 days), and the recovery phase (beyond five days) [4]. Approximately 5-10% of patients may progress to the critical phase after the third to fourth day of illness, which is marked by vasculopathy, coagulopathy, and shock. Hemorrhagic manifestations can occur during both the febrile and afebrile phases, commonly involving the skin, mucosal surfaces, gastrointestinal tract, and genitourinary tract [3].
Atraumatic pathological rupture of the spleen, although rare, carries a significant risk of morbidity and mortality. The overall incidence of atraumatic splenic rupture ranges between 0.1% and 0.3%, with variation depending on the specific etiological factor. Common pathological causes include neoplastic diseases, infections, inflammatory conditions, drug-induced effects, and mechanical disorders, which together account for 93% of atraumatic splenic rupture cases, compared to 7% in an idiopathic normal spleen. The overall mortality rate is approximately 12.2%, with splenomegaly, age over 40 years, and neoplastic disorders identified as high-risk factors [9].
The World Society of Emergency Surgery (WSES) classifies splenic injury according to anatomical and hemodynamic status into mild (WSES Class I), moderate (Class II and III), and severe (Class IV) categories (Table 3) [10]. This classification aids in guiding management strategies.
Management of splenic subcapsular hematoma remains controversial. While early splenectomy has traditionally been advocated to prevent rupture and complications, recent evidence suggests that many cases may regress with conservative management or splenic artery embolization [9,11,12].
In hemodynamically stable patients, non-operative, organ-preserving approaches can be successful, provided there is careful patient selection and access to appropriate monitoring and interventional radiology or surgical support.
In our first case, the patient was hemodynamically stable corresponding to Class II of WSES classification of splenic injury. He was managed successfully with close monitoring and multidisciplinary team involvement. Conversely, angioembolization serves as a salvage therapy in moderate to severe cases where hemodynamic instability and severe coagulopathy preclude surgical intervention. Our second patient presented with severe shock, coagulopathy, and multi-organ dysfunction and underwent splenic artery embolization as a source control measure, as he was considered too unstable for surgery corresponding to Class IV in the WSES classification of splenic injury [9,10].
In both these cases, the splenic rupture was diagnosed during the critical phase of the illness (days 4-6) [4].
The primary objective in managing bleeding in coagulopathic patients is prompt control of the bleeding source to achieve hemodynamic stability. In atraumatic splenic rupture, it is critical to address the underlying pathology precipitating the event. In both our cases, dengue-associated coagulopathy was the key etiologic factor. Although both patients presented during the critical phase of dengue illness, their clinical courses diverged-one toward recovery and the other toward deterioration. Our decisions regarding conservative versus interventional management were therefore guided not only by baseline patient characteristics but also by their dynamic clinical progression in the ICU setting.
This case report is based on a single-center experience of managing two cases, and hence, generalizability is limited.
Conclusions
Management of splenic subcapsular hematoma in thrombocytopenic and coagulopathic patients warrants a high index of suspicion and early evaluation. A careful, individualized approach is essential. The decision regarding the urgency and type of intervention should be guided primarily by the patient’s clinical condition, hemodynamic stability, and coagulation status rather than imaging findings alone. Premature or aggressive intervention in a bleeding, thrombocytopenic patient may lead to adverse outcomes. This type of situation needs a multidisciplinary approach with the readiness to switch to an interventional or surgical approach from a conservative approach or vice versa, depending on disease progression. Therefore, a balanced strategy that thoughtfully integrates both conservative and interventional options is essential to optimize patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dengue virus Clin Lab Med Ross TM 1491603020102051354510.1016/j.cll.2009.10.007PMC 7115719 · doi ↗ · pubmed ↗
- 2Dengue 2 2025 2025 https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue
- 3National Guidelines for Clinical Management of Dengue Fever Ministry of Health and Family Welfare, Government of India 2023 https://ncvbdc.mohfw.gov.in/Doc/National%20Guidelines%20for%20Clinical%20Management%20of%20Dengue%20Fever%202023.pdf
- 4ISCCM position statement: management of severe dengue in intensive care unit Indian J Crit Care Med Bhalla A Singh H Suri V 058282024 https://pubmed.ncbi.nlm.nih.gov/39234231/10.5005/jp-journals-10071-24748 PMC 1136992239234231 · doi ↗ · pubmed ↗
- 5Splenic artery embolization in subcapsular splenic hematoma secondary to dengue hemorrhagic fever J Glob Infect Dis Dronamraju SS Gaidhane SA Mahalaqqa KN Gaidhane AM Andhale AG Quazi ZS 1451471320213470315610.4103/jgid.jgid_140_20PMC 8491811 · doi ↗ · pubmed ↗
- 6Systematic review of spontaneous splenic rupture in dengue-infected patients Rev Med Virol Radwan I Magdy Khattab M Mahmoud AR 029201910.1002/rmv.202930609179 · doi ↗ · pubmed ↗
- 7A stitch in time dengue with spontaneous splenic rupture Radio Infect Dis Padyana M Gopaldas JA Karanth S 14514872020
- 8National Early Warning Score (NEWS) 2 10 2025 2017 https://www.rcp.ac.uk/improving-care/resources/national-early-warning-score-news-2/