Secondary Neuropathy From Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal Gammopathy, and Skin Changes (POEMS) Syndrome: A Case Report
Peter Young, Maxwell Kroloff

TL;DR
A 62-year-old woman with severe nerve damage was diagnosed with POEMS syndrome and showed significant improvement after treatment.
Contribution
Highlights the importance of considering POEMS syndrome as a secondary cause of polyneuropathy.
Findings
The patient had severe length-dependent neuropathy with demyelination and axonal changes.
Treatment with lenalidomide, dexamethasone, and stem cell transplant led to marked functional improvement.
POEMS syndrome was identified as the underlying cause after ruling out other secondary factors.
Abstract
We report the case of a 62-year-old woman who presented with signs and symptoms of distal sensory polyneuropathy. Her initial electromyography and nerve conduction studies (EMG/NCS) showed a severe length-dependent neuropathy with uniform demyelination and secondary axonal changes. After extensive evaluation for secondary causes, she was ultimately found to have polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS) syndrome. She underwent treatment with lenalidomide and dexamethasone, followed by an autologous stem cell transplant, and is now doing well with marked improvement in her function. This case emphasizes the importance of evaluating for secondary causes of polyneuropathy and provides a brief overview of POEMS syndrome.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
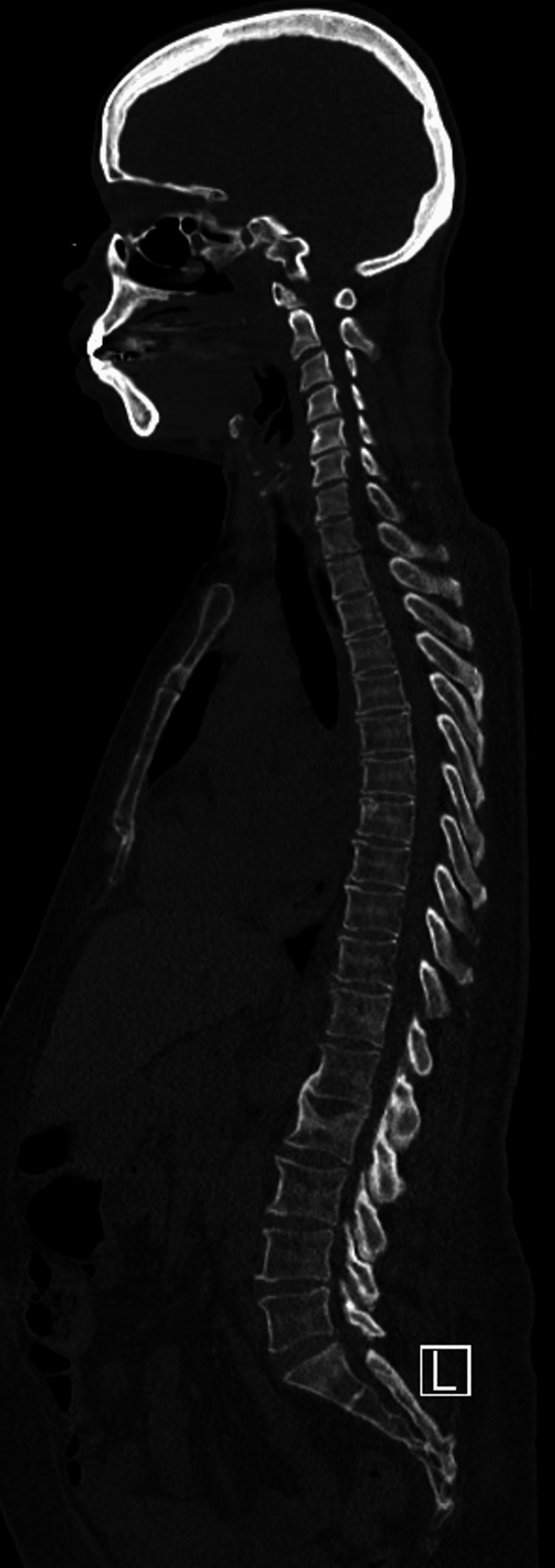 Figure 1
Figure 1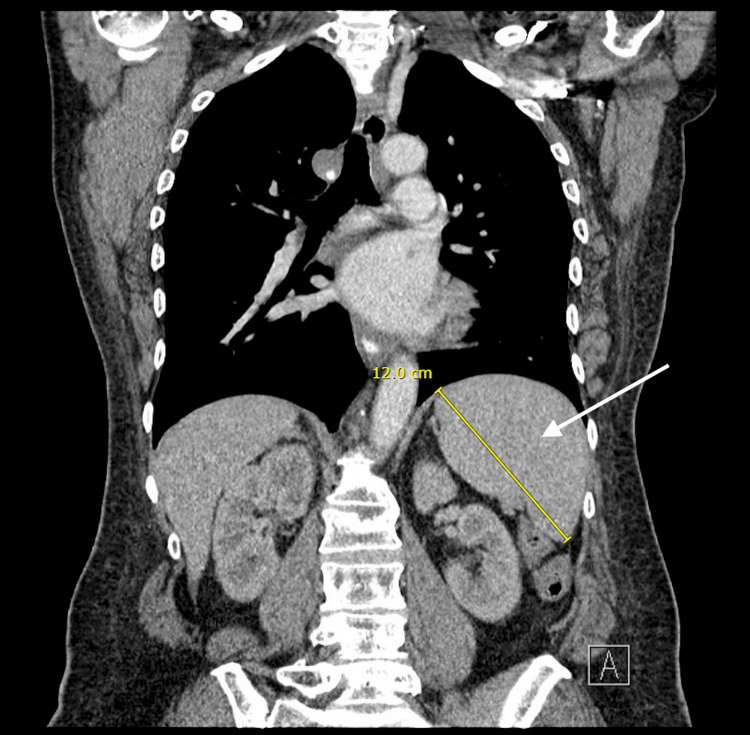 Figure 2
Figure 2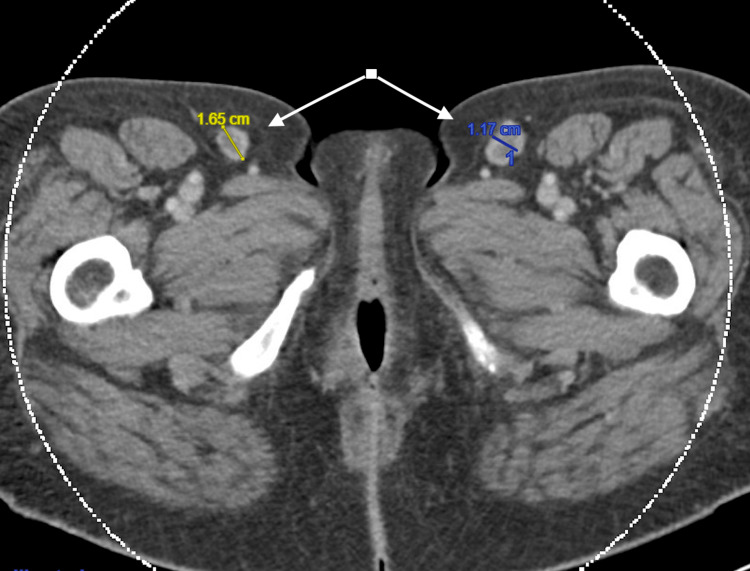 Figure 3
Figure 3| Lab test | Lab value | Reference range |
| HIV antigen/antibody test | Nonreactive | Nonreactive |
| RPR | Nonreactive | Nonreactive |
| TSH | 0.62 mcIU/mL | 0.3-4.7 mcIU/mL |
| Vitamin B1 | 105 nmol/L | 70-180 nmol/L |
| Vitamin B6 | 20.6 nmol/mL | 20-125.0 nmol/mL |
| Vitamin B12 | 380 pg/mL | 254-1,080 pg/mL |
| Hemoglobin A1c | 5.4% | <5.7% |
| SPEP | No monoclonal bands detected | |
| Serum IFE | Monoclonal IgA lambda protein present | |
| Kappa/lambda light chain ratio | 1.18 | 0.26-1.65 |
| C-reactive protein | 0.5 mg/dL | <0.8 mg/dL |
| VEGF | 1,417 pg/mL | 31-86 pg/mL |
| Mandatory criteria | Major criteria (at least one) | Minor criteria (at least one) |
| Polyneuropathy | Sclerotic skeletal lesions | Organomegaly |
| Monoclonal plasma cell disorder | Elevated VEGF levels | Volume overload |
| Castleman disease | Endocrinopathy | |
| Skin changes | ||
| Papilledema | ||
| Thrombocytosis or polycythemia |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Peripheral Nerve Disorders
Introduction
Distal symmetric polyneuropathy (DSP) is the most common subtype of peripheral neuropathy [1]. It can be idiopathic but is often associated with secondary causes [2]. These can include diabetes mellitus, nutritional deficiencies, and toxins such as alcohol or chemotherapy, as well as infections such as human immunodeficiency virus (HIV) or inflammatory conditions [2]. One rare cause of DSP is a paraneoplastic condition characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes, otherwise known as POEMS syndrome [3]. POEMS syndrome is a rare, multi-system disorder driven by a plasma cell clone that can present with a rapidly progressive symmetric ascending polyneuropathy but often involves other debilitating end-organ manifestations as well [4]. Early diagnosis is crucial to prevent progressive functional decline and life-threatening complications [4].
A diagnosis of POEMS requires the presence of peripheral neuropathy and a monoclonal plasma cell disorder, as well as one major criterion and one minor criterion [3]. Major criteria include osteosclerotic or mixed sclerotic/lytic lesions on imaging, Castleman disease, and elevated plasma vascular endothelial growth factor (VEGF) levels [3]. Minor criteria include organomegaly, volume overload, endocrinopathy, skin changes, papilledema, and thrombocytosis or polycythemia [3]. Given its rarity and poorly understood pathogenesis, there is no standardized treatment for POEMS, though most protocols target what is thought to be an underlying clonal plasma cell process.
Case presentation
A 62-year-old woman presented to the clinic with two years of progressive sensitivity and heaviness in her lower extremities. She was experiencing intermittent swelling in her feet that extended up to her calves, as well as numbness, tingling, and burning pain particularly at night and a sensation of tightness in her skin. She reported thinner and more wrinkled skin with acneiform changes on her face. She had become dependent on a cane for ambulation and had suffered multiple falls due to her symptoms. She also endorsed weight loss of at least 40 pounds over 12 months and an enlarged thyroid. She had no fevers, chills, night sweats, lymphadenopathy, back pain, or trauma. She had a history of transient ischemic attack and was on aspirin 81 mg daily and took gabapentin 300 mg three times a day for neuropathic pain. Past medical, family, and social histories were otherwise noncontributory.
At her initial visit, her vitals were unremarkable. Physical exam was notable for 1+ pitting edema to her calves bilaterally. She had significantly diminished pinprick and proprioceptive sensation in her lower extremities, with mildly reduced sensation in her upper extremities. Motor testing revealed 3/5 strength in dorsiflexion and plantarflexion bilaterally, 3+/5 strength in knee flexion and extension, and 4/5 strength in her hips. Upper extremity strength was 4/5 throughout, and she had absent reflexes at the patella, Achilles, biceps, and brachioradialis tendons bilaterally with a downward plantar response. Coordination was intact, but gait was markedly unsteady.
Labs (Table 1) were notable for a monoclonal IgA lambda protein on serum immunofixation (IFE) but normal serum protein electrophoresis (SPEP), urine protein electrophoresis (UPEP), and serum free light chains. Comprehensive metabolic panel, complete blood count, and urinalysis were normal. She had a negative HIV and rapid plasma reagin (RPR) test; normal B12, B6, and B1 levels; and normal thyroid-stimulating hormone (TSH). Magnetic resonance imaging (MRI) of her lumbar and cervical spine was performed, which showed degenerative changes and foraminal narrowing but no cord signal abnormality. Electromyography and nerve conduction studies (EMG/NCS) revealed a very severe length-dependent neuropathy with uniform demyelination and secondary axonal changes, with more dramatic findings in the lower versus upper extremities.
She was seen urgently by neurology and hematology within the next three weeks. A myeloma skeletal survey did not reveal any lytic lesions (Figure 1), and a computed tomography (CT) scan of her chest, abdomen, and pelvis showed mild widespread lymphadenopathy along with borderline splenomegaly (Figures 2, 3). Bone marrow biopsy was normal but showed a small population of 7%-8% lambda-restricted plasma cells, consistent with plasma cell dyscrasia. Based on the presence of a severe peripheral neuropathy as well as a monoclonal plasma cell disorder, there was concern for potential POEMS syndrome. To investigate further, VEGF levels were sent and returned at 1,412 pg/mL (with an upper limit of normal being 86). She was diagnosed with POEMS and started on lenalidomide and dexamethasone. Six months later, she underwent an autologous stem cell transplant. Daratumumab induction had been planned but was denied by insurance despite multiple appeals. With this treatment and aggressive rehabilitation, she has had significant improvement in function, and one year later, she is now ambulatory without any assistive devices. She has remained off chemotherapeutics with close surveillance of her neuropathic symptoms and lab work including SPEP/IFE, kappa/lambda light chains, and VEGF levels.
Normal CT Myeloma SurveySagittal section of the CT myeloma survey, which did not reveal any lytic lesions and was overall unremarkable. Osteosclerotic or mixed sclerotic/lytic lesions are one of the three major criteria for POEMS. In this case, the patient satisfied a major criterion by the presence of elevated plasma VEGF protein.CT: computed tomography; POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes; VEGF: vascular endothelial growth factor
CT Scan Showing Borderline SplenomegalyCT abdomen/pelvis showing borderline splenomegaly of approximately 12 cm, a nonspecific finding but also one of the minor criteria for POEMS syndrome (organomegaly).CT: computed tomography; POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes.
CT Scan Showing Inguinal LymphadenopathyCT abdomen/pelvis revealed mild lymphadenopathy, most notable in the inguinal region. Lymphadenopathy qualifies as organomegaly, which is one of the minor criteria for POEMS syndrome. Other minor criteria include extravascular volume overload, endocrinopathy, skin changes, papilledema, and thrombocytosis or polycythemia.CT: computed tomography; POEMS: polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes.
Discussion
This patient presented with symmetric sensory symptoms along with muscle weakness predominantly affecting her distal extremities, consistent with a DSP. Evaluating for secondary causes of neuropathy is a crucial part of the initial workup. There are numerous etiologies that contribute to DSP, which is the most common subtype of neuropathy. Diabetes mellitus is the most common cause (18%-49% of cases), followed by alcohol use, toxins and chemotherapeutic drugs, nutritional deficiencies, immune-mediated causes, and hereditary conditions (most commonly Charcot-Marie-Tooth disease) [1]. Chronic idiopathic axonal polyneuropathy (CIAP) is a diagnosis of exclusion, which is responsible for between 12% and 49% of cases [2].
This patient was ultimately found to have POEMS syndrome, a rare paraneoplastic syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes [3]. The pathogenesis is not fully understood but thought to be related to increased VEGF among other proinflammatory cytokines driven by a clonal plasma cell process [5]. As in the above patient, a rapidly worsening, symmetric ascending peripheral polyneuropathy is often the initial presenting feature, emphasizing the importance of early diagnosis and intervention [4]. Yet, distinguishing POEMS from alternative etiologies of peripheral neuropathy such as amyloid light chain (AL) amyloidosis or chronic inflammatory demyelinating polyneuropathy (CIDP) can be challenging.
To avoid lasting end-organ manifestations, clinicians must maintain a high index of suspicion for POEMS, especially in the setting of a symmetric length-dependent peripheral neuropathy and a monoclonal gammopathy. NCS can show demyelination similar to CIDP but has distinguishing characteristics including more severe axonal loss [6]. Aside from the neuropathy, the prevalence of other manifestations varies greatly. In addition to a complete history and physical exam, complete blood count, and comprehensive metabolic panel, the diagnostic workup should include a serum and 24-hour urine collection with electrophoresis and IFE, as well as quantitative immunoglobulins and a serum free light chain assay. A serum VEGF level is also indicated, in addition to hormonal studies, to screen for endocrinopathy. In terms of imaging, a CT survey or PET-CT is necessary to evaluate for osteosclerotic lesions, as a skeletal survey is likely to miss occult lesions. An echocardiogram should be performed to assess right-sided pressures, and finally, a bone marrow aspirate and biopsy with fluorescence in situ hybridization (FISH) panel for myeloma should be completed. Interestingly, the bone marrow plasma cell clone is often a relatively small size (~5% in 50% of patients) with POEMS [5]. Mandatory criteria for the diagnosis of POEMS syndrome require a polyneuropathy (typically demyelinating) and a monoclonal plasma cell proliferative disorder (typically lambda light chain). One additional major criterion is required, including the presence of Castleman disease, sclerotic bone lesions, or an elevated VEGF. Finally, at least one minor criterion is required, including organomegaly, extravascular volume overload, endocrinopathy, skin changes, or thrombocytosis/polycythemia (Table 2) [3].
Due to its rarity, there is no standard therapeutic strategy for POEMS. In fact, treatment regimens are largely based on prior retrospective studies, as well as extrapolated from treatment strategies in patients with multiple myeloma or AL amyloidosis. Fortunately, compared with multiple myeloma, the prognosis of POEMS is superior, with a median overall survival of 13.8 years, and this estimate is prior to the incorporation of many of the novel therapies employed today [4]. Generally, treatment is aimed at targeting the plasma cell clone along with upfront autologous stem cell transplant with high-dose melphalan conditioning for transplant-eligible patients. Autologous stem cell transplant leads to a durable response with five-year progression-free survival on the order of 74% and overall survival of 89% [7].
The immunomodulatory drug, lenalidomide, in combination with corticosteroids is the most studied initial induction regimen with a clinical and biochemical response rate of approximately 75% to 95% [8]. The proteasome inhibitor, bortezomib, is another option, yet treatment-related neuropathy remains a major concern given the often debilitating baseline neuropathy in many patients with POEMS. In comparison, incorporation of daratumumab, an anti-CD38 monoclonal antibody, represents a more promising therapeutic approach in combination with lenalidomide and dexamethasone, given its balance of tolerability and efficacy in both patients with multiple myeloma and POEMS. Multiple case reports have highlighted the encouraging upfront clinical and hematologic response rates when daratumumab is incorporated with lenalidomide and dexamethasone [9]. However, the lack of standardized clinical trials and drug cost have limited its use, as in our patient.
Conclusions
POEMS is a systemic disease thought to be driven by a plasma cell clone that can result in multiple debilitating end-organ manifestations. Clinicians must maintain a high index of suspicion as early diagnosis and treatment are paramount. This highlights the importance of evaluating for secondary causes of peripheral neuropathy. Given the systemic nature of POEMS, treatment is aimed at targeting the plasma cell clone, though its rarity continues to make POEMS a diagnostic and therapeutic challenge.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peripheral neuropathies Handb Clin Neurol Hanewinckel R Ikram MA Van Doorn PA 26328213820162763796310.1016/B 978-0-12-802973-2.00015-X · doi ↗ · pubmed ↗
- 2The epidemiology and risk factors of chronic polyneuropathy Eur J Epidemiol Hanewinckel R van Oijen M Ikram MA van Doorn PA 5203120162670049910.1007/s 10654-015-0094-6PMC 4756033 · doi ↗ · pubmed ↗
- 3POEMS syndrome: update on diagnosis, risk-stratification, and management Am J Hematol Dispenzieri A 193419509820233773282210.1002/ajh.27081 · doi ↗ · pubmed ↗
- 4An update on the diagnosis and management of the polyneuropathy of POEMS syndrome J Neurol Cerri F Falzone YM Riva N Quattrini A 25826726620193026417610.1007/s 00415-018-9068-4PMC 6343023 · doi ↗ · pubmed ↗
- 5Recent advances in the treatment and supportive care of POEMS syndrome J Clin Med Bou Zerdan M George TI Bunting ST Chaulagain CP 70111120223649858810.3390/jcm 11237011 PMC 9741379 · doi ↗ · pubmed ↗
- 6Uniform demyelination and more severe axonal loss distinguish POEMS syndrome from CIDPJ Neurol Neurosurg Psychiatry Mauermann ML Sorenson EJ Dispenzieri A Mandrekar J Suarez GA Dyck PJ Dyck PJ 4804868320122239644110.1136/jnnp-2011-301472 · doi ↗ · pubmed ↗
- 7High-dose therapy and autologous stem cell transplantation in patients with POEMS syndrome: a retrospective study of the Plasma Cell Disorder sub-committee of the Chronic Malignancy Working Party of the European Society for Blood & Marrow Transplantation Haematologica Cook G Iacobelli S van Biezen A 16016710220172763420110.3324/haematol.2016.148460 PMC 5210246 · doi ↗ · pubmed ↗
- 8Efficacy and safety of regimens used for the treatment of POEMS syndrome-a systematic review Clin Lymphoma Myeloma Leuk Faizan U Sana MK Farooqi MS Hashmi H 03322202210.1016/j.clml.2021.07.03334507924 · doi ↗ · pubmed ↗