Genetic SHBG Deficiency Unmasks the Discrepancy Between Biochemical and Clinical Hypogonadism
Xue D Manz, Michel J Vos, Ron S Booij, Rieneke Sanson, Leo H J Jacobs

TL;DR
A man with very low SHBG levels showed normal symptoms but abnormal hormone tests, revealing how genetic SHBG issues can confuse hypogonadism diagnoses.
Contribution
This case highlights the diagnostic challenges of genetic SHBG deficiency and its impact on testosterone measurements.
Findings
Low SHBG levels can mask true testosterone status, leading to misleading biochemical results.
Genetic variants in SHBG can impair hormone binding and secretion, causing abnormal lab findings without clinical symptoms.
Direct measurement of free testosterone is more accurate than calculated values in cases of SHBG deficiency.
Abstract
Near–absent serum SHBG influences calculated free testosterone, complicating the evaluation of suspected hypogonadism. We report a 50–year–old man with longstanding low total testosterone (147.1 ng/dL [SI: 5.1 nmol/L], reference range: 289-866 ng/dL [SI: 10.0-30.0 nmol/L]). Further laboratory testing revealed a suppressed SHBG of 2 nmol/L (reference range: 14–72 nmol/L) and remarkably normal calculated free testosterone (between 5.0 and 6.0 ng/dL [SI: 0.174-0.210 nmol/L], reference range: 4.9-15.7 ng/dL [SI: 0.160-0.700 nmol/L]). Direct equilibrium–dialysis measurement, however, revealed low free testosterone (2.9 ng/dL [SI: 0.099 nmol/L], reference range: 4.9-15.8 ng/dL [SI: 0.170-0.546 nmol/L]), establishing the diagnosis of biochemical hypogonadism. Genetic analysis demonstrated compound heterozygosity for the SHBG variants c.554C > T (p.Pro185Leu), which impairs steroid binding and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
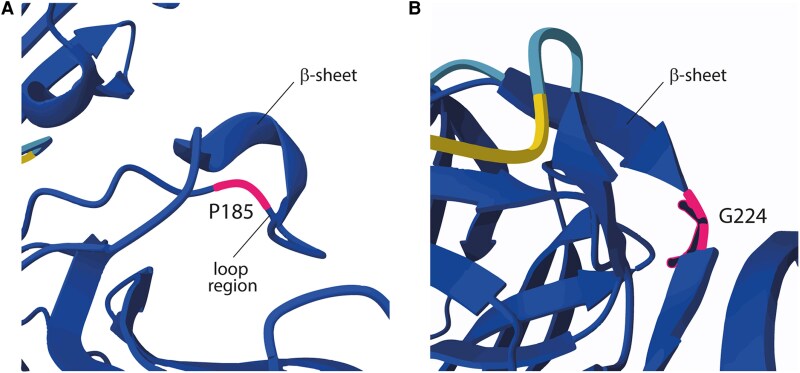 Figure 1
Figure 1| Laboratory test | Results at presentation (on clomiphene) | 6 weeks past presentation | 12 weeks past presentation | Reference range |
|---|---|---|---|---|
| TSH | 0.64 mIU/L | 0.35-5.00 mIU/L | ||
| FT4 | 0.86 ng/dL | 0.7-1.5 ng/dL | ||
| Cortisol 10:00 AM | 14.1 µg/dL | 3.6-19.6 µg/dL | ||
| LH | 7 IU/L | 2 IU/L | 4 IU/L | 1-12 IU/L |
| Testosterone | 115 ng/dL | 141 ng/dL | 104 ng/dL | 230-864 ng/dL |
| Testosterone (LC-MS/MS) | 85 ng/dL | 302-1066 ng/dL | ||
| Calculated free Testosterone | 5.0 ng/dL | 6.0 ng/dL | 8.5 ng/dL | 4.6-20.2 ng/dL |
| Free Testosterone (dialysis, LC-MS/MS) | 2.9 ng/dL | 4.9-15.8 ng/dL | ||
| SHBG | 2 nmol/L | 2 nmol/L | 1 nmol/L | 14-72 nmol/L |
| IGF-1 (SDS) | 48 ng/mL (−2.5 SDS) | 153 ng/mL (−0.06 SDS) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHypothalamic control of reproductive hormones · Adrenal Hormones and Disorders · Hormonal and reproductive studies
Introduction
SHBG is a glycoprotein primarily produced in the liver and is critical for the transport of sex steroids. SHBG has a high affinity for androgens and a lower affinity for estrogens [1]. SHBG regulates the free, biologically active fractions and influences both their metabolic clearance and tissue accessibility [2]. Modulating the proportion of unbound sex steroids orchestrates sexual characteristics and reproductive function in both men and women. Reduced SHBG levels may have significant clinical consequences and are commonly associated with obesity, insulin resistance, metabolic syndrome, and polycystic ovary syndrome. SHBG levels are regulated by multiple factors, including hormonal, nutritional, genetic, and metabolic influences. Circulating SHBG concentrations are shaped by hormonal, nutritional, metabolic, and genetic factors. Twin and family studies indicate that common genetic variants explain approximately 30% to 80% of the interindividual variation in serum SHBG levels [3]. By contrast, true monogenic SHBG deficiency due to loss-of-function mutations is exceedingly rare. Although numerous SHBG polymorphisms have been identified, inconsistencies among published studies continue to obscure their precise biological significance. In this report, we present an adult man with near-absent SHBG levels, caused by a compound heterozygous variation in the coding region of human SHBG, illustrating diagnostic pitfalls and sex-specific phenotypic effects.
Case Presentation
A 50-year-old man was referred to the internal medicine department for reevaluation of a longstanding low testosterone level. His condition was first discovered 10 years earlier during a fertility assessment, when semen analysis revealed oligoasthenoteratozoospermia. At that time, laboratory evaluation showed a total testosterone of 147.1 ng/dL (SI: 5.1 nmol/L) (reference range: 289-866 ng/dL [SI: 10.0-30.0 nmol/L]), reduced inhibin B of 86 pg/mL (SI: 86 ng/L) (reference range: 150-400 pg/mL [SI: 150-400 ng/L]), and discordant gonadotropins: an inappropriately low LH of 1.8 IU/L (reference range: 1.5-8 IU/L) alongside an elevated FSH of 13.6 IU/L (reference range: 2-7 IU/L).
Therapeutic intervention included clomiphene citrate therapy and left-sided varicocelectomy, which improved spermatogenesis. His partner initially conceived spontaneously but experienced several miscarriages. Eventually, the couple had 2 children while he continued clomiphene therapy for several years. Notably, no further investigation into the underlying cause of his hypogonadism was performed at the fertility center.
Upon presentation to our hospital, the patient appeared generally healthy with normal libido, energy levels, and muscle strength, which was incongruent with his biochemical profile. Physical examination revealed a well-virilized male with normal male-pattern hair distribution, low-normal testicular volumes (12 mL, reference range: 12-25 mL), normal semen volume (3.3 mL, reference range: 1.5-5 mL), and no gynecomastia.
Diagnostic Assessment
Initial laboratory evaluation during clomiphene therapy revealed some striking findings (Table 1). A low total testosterone of 115 ng/dL (SI: 4.0 nmol/L) (reference range: 230-864 ng/dL [SI:10.0-30.0 nmol/L]) with a LH of 7 IU/mL (reference range: 1-12 IU/mL) and suppressed SHBG of 2 nmol/L (reference range: 14-72 nmol/L). IGF-1 was also reduced at 48 ng/mL (−2.5 SD score). Furthermore, thyroid function (TSH and free T4) and adrenal function (morning cortisol) were normal (Table 1). Brain magnetic resonance imaging showed no pituitary abnormalities.
Although his free testosterone of 5.0 ng/dL (SI: 0.174 nmol/L) (reference range: 4.9-15.7 ng/dL [SI: 0.160-0.700 nmol/L]) was normal, it was calculated based on SHBG levels [2]. Therefore, direct free testosterone was assessed by equilibrium dialysis through our reference laboratory, which revealed free testosterone of 2.9 ng/dL (SI: 0.099 nmol/L) (reference range: 4.9-15.8 ng/dL [SI: 0.170-0.546 nmol/L]), together with a reduced total testosterone of 85 ng/dL (SI: 2.95 nmol/L) (reference range: 302-1065 ng/dL [SI: 10.5-37 nmol/L]), determined by liquid chromatography-tandem mass spectrometry. Although direct measurement revealed low free testosterone, the absence of clinical symptoms suggested preserved androgen action at the tissue level. This discrepancy prompted further investigation.
Given the persistently near-absent SHBG level without clinical manifestation, genetic evaluation of SHBG was performed. Informed consent was obtained from the patient for genetic analysis and publication. Genomic DNA was isolated from peripheral blood leukocytes. The genomic sequence for human SHBG was retrieved from the National Center for Biotechnology Information database (Gene ID 6462). The SHBG gene was amplified from genomic DNA in 3 overlapping fragments, using DreamTaq DNA polymerase (Thermo Fisher Scientific, Groningen, The Netherlands). Sequencing was performed by Sanger sequencing (BaseClear, Leiden, The Netherlands) and analyzed using BioEdit 7.7.1 [4]. Sequencing identified 2 heterozygous single nucleotide polymorphisms (SNPs) in the coding region of SHBG. For verification of the 2 SNPs, restriction enzyme analysis was carried out on the PCR products using the restriction enzymes SmaI and Cfr10 I (New England Biolabs, Ipswich, USA and NIPPON Genetics, Düren, Germany), respectively. The presence of the SNPs resulted in disruption of the enzyme recognition sites.
Treatment
Clomiphene stimulates pituitary gonadotropins by modulating the estrogen receptor. This binding results in LH and FSH release and negatively regulates GH production by activating SOCS3, which inhibits Jak/Stat signaling. Subsequently, this reduces IGF-1 levels by 40% to 80% in healthy adult men with intact pituitary function [5]. Therefore, the patient's clomiphene therapy was discontinued to evaluate his normal hormonal regulation. Furthermore, no testosterone supplementation was initiated because the patient did not experience any clinical symptoms.
Outcome and Follow-up
Six weeks after clomiphene had been discontinued, the patient's IGF-1 concentration had normalized to 153 ng/mL (−0.06 SD score), whereas SHBG remained markedly suppressed (<5 nmol/L). Consequently, after respectively 6 and 12 weeks, total testosterone continued to fluctuate between 104 and 141 ng/dL (SI: 3.6-4.9 nmol/L), yet the calculated free testosterone stayed within the reference range at 6.95 ng/dL (SI: 0.241 nmol/L). Despite the persistently low total testosterone, the patient remained clinically asymptomatic.
The 2 SNPs correspond to the National Center for Biotechnology Information reference SNP cluster IDs rs6258 and rs1182086432, resulting in a proline to leucine (exon 4, c.554C > T, p.P185L) amino acid substitution and a glycine to arginine (exon 5, c.670G > A, p.G224R) amino acid substitution, respectively. 3D structural modeling using AlphaFold [6] predicted that Pro185 is located in a loop region, where it likely confers rigidity (Fig. 1A). Its substitution with Leu185 introduces greater flexibility, potentially impacting protein folding or function. AlphaFold modeling of Gly224 showed that this amino acid is positioned between 2 β-sheets, where it likely facilitates flexibility and structural integrity. Substitution to Arg224 introduces a positively charged, bulkier side chain, which is predicted to cause reduced flexibility, steric hindrance, and most likely structural disruption (Fig. 1B).
AlphaFold-predicted structure of SHBG illustrating the location and predicted effects of the identified variants. (A) P185 is situated within a loop region adjacent to a β-sheet. Proline's rigid cyclic structure restricts flexibility. The p.P185L substitution replaces proline with leucine, a more flexible residue, which may alter loop dynamics and protein stability. (B) G224 is positioned between 2 β-sheets, a crucial structural feature required for local flexibility and β-sheet alignment. The p.G224R substitution introduces a bulkier, positively charged arginine, which could disrupt local folding through steric clashes and altered electrostatic interactions.Abbreviations: G224, glycine 224; P185, proline 185.
Discussion
This case highlights the complex interplay between biochemical evaluation and clinical presentation in endocrinology. SHBG plays an important role in testosterone homeostasis, and severely low levels can result in misleading calculated free testosterone values. Free testosterone is estimated by mathematically modeling its equilibrium with SHBG and albumin, using measured total testosterone, SHBG, and albumin levels, according to the Vermeulen calculation [7]. When SHBG is profoundly low, calculated free testosterone may not reflect dialyzed free testosterone, and in such discordant situations, equilibrium dialysis provides a more definitive assessment [8].
The patient’s markedly reduced SHBG levels were explained by a compound heterozygous missense variant in the SHBG gene: c.554C > T (p.Pro185Leu; rs6258) in exon 4 and c.670G > A (p.Gly224Arg; rs182086432) in exon 5. These SHBG variants have been previously characterized. The p.Pro185Leu variant is suggested to have a prevalence of 2% and reduces SHBG levels by 25% to 50% in heterozygous subjects [9]. The substitution of proline by leucine at position 185 may lead to a more flexible structure, affecting glycosylation and calcium binding, ultimately reducing testosterone binding affinity and increasing SHBG clearance (Fig. 1A). This altered binding affinity is supported by a recent study by Walravens et al [10]. Interestingly, this study also showed that the rs6258 variant did not affect calculated free testosterone values. This is probably explained by the fact that less than 20% of circulating SHBG has reduced testosterone affinity, while the remaining 80% retains normal function. However, the participants were healthy men carrying a heterozygous SNP. A case report with a homozygous mutation showed a SHBG serum level below 5 nmol/L and described gonadotropin-independent precocious puberty, likely due to increased free sex hormone levels [11]. Furthermore, the patient we describe is compound heterozygous for 2 SNPs, in which the rs182086432, p.Gly224Arg variant has been identified in a Dutch family and is associated with intracellular retention and a complete block in SHBG secretion [12]. Substitution to Arg224 is likely to impair SHBG folding, which causes accumulation of SHBG in the endoplasmic reticulum, preventing secretion [12]. As a result, homozygous variants have no detectable circulating SHBG. Interestingly, the homozygous presence in a male showed normal volume and sperm concentration in his semen analysis. The female exhibited a prolonged but regular menstrual cycle without signs of hirsutism or hyperandrogenism. This suggests that a complete absence of circulating SHBG does not interfere with gonadal function [2].
Total to nearly absent SHBG levels did not interfere with male gonadal differentiation or pubertal development and reproductive function of the gonads. In contrast, in women, low SHBG increases bioavailable androgens, potentially causing hirsutism, menstrual irregularities, and features of polycystic ovary syndrome. This sex-specific difference may be explained by various mechanisms. First, SHBG is also produced in other tissues than the liver, including the placenta, testis, brain, and endometrium. The testis produces an alternative SHBG transcript [3], also known as androgen binding protein. This transcript lacks exon 7, which may result in different protein folding to provide local regulatory functions [13]. The mutations found in this patient are located in exon 4 and 5, which are identical for hepatic and testicular SHBG. Therefore, we expect that testicular SHBG (androgen binding protein) is also affected, although this hypothesis is an area for future study. Second, intratesticular testosterone concentrations are approximately 100-fold higher than serum levels, which exceeds testicular SHBG binding capacity, probably explaining the preservation of spermatogenesis in this patient [14, 15]. The coexisting andrological abnormalities (eg, low inhibin B/high FSH, oligoasthenoteratozoospermia, varicocele, small testicular volume) can explain gonadotropin and semen findings but do not account for the near-absence of SHBG caused by SHBG variants in this patient as circulating SHBG is from hepatic origin [3, 13].
In summary, the compound heterozygosity of SHBG variants identified in our patients describes preserved androgen-dependent functions and normal LH that argue against clinical hypogonadism. This highlights the limitations of biochemical criteria and underscores the need to contextualize laboratory values with clinical presentation, particularly in the setting of genetic SHBG deficiencies. In such rare cases, the concept of “biochemical hypogonadism” may not indicate true androgen insufficiency but rather reflect limitations in current diagnostic paradigms. Long-term follow-up will be important to determine whether such patients face any late complications from their lifelong absence of circulating SHBG.
Learning Points
Free testosterone must be measured directly by equilibrium dialysis when SHBG levels are extremely low, since calculated values are invalid.Compound heterozygosity for p.Pro185Leu (affecting protein stability/binding) and p.Gly224Arg (causing retention) can reduce circulating SHBG.Male gonadal function and fertility can remain largely intact despite absent circulating androgen carrier protein; most likely, intratesticular testosterone concentrations are independent of plasma binding proteins.
Contributors
All authors contributed to the diagnosis and clinical interpretation of the patient's case. X.D.M. conceptualized and prepared the manuscript. L.H.J. supervised the project. M.J.V. and R.S.B. performed and interpreted the DNA sequencing analysis. R.S. was responsible for patient care. All authors reviewed and approved the final version.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hammond GL . Plasma steroid-binding proteins: primary gatekeepers of steroid hormone action. J Endocrinol. 2016;230(1):R 13‐R 25.27113851 10.1530/JOE-16-0070 PMC 5064763 · doi ↗ · pubmed ↗
- 2Hogeveen KN, Cousin P, Pugeat M, Dewailly D, Soudan B, Hammond GL. Human sex hormone–binding globulin variants associated with hyperandrogenism and ovarian dysfunction. J Clin Invest. 2002;109(7):973‐981.11927624 10.1172/JCI 14060 PMC 150924 · doi ↗ · pubmed ↗
- 3Xita N, Tsatsoulis A. Genetic variants of sex hormone-binding globulin and their biological consequences. Mol Cell Endocrinol. 2010;316(1):60‐65.19733622 10.1016/j.mce.2009.08.025 · doi ↗ · pubmed ↗
- 4Hall TA . Bio Edit: a user-friendly biological sequence alignment editor and analysis program for Windows 95/98/NT. Nucleic Acids Symp Ser. 1999;41(41):95‐98.
- 5Mogar N, Zhang D, Heaney AP. Reduced IGF-1 levels following clomiphene treatment for male hypogonadism. J Endocr Soc. 2025;9(7):bvaf 078.40421427 10.1210/jendso/bvaf 078PMC 12105911 · doi ↗ · pubmed ↗
- 6Jumper J, Evans R, Pritzel A, et al Highly accurate protein structure prediction with Alpha Fold. Nature. 2021;596(7873):583‐589.34265844 10.1038/s 41586-021-03819-2PMC 8371605 · doi ↗ · pubmed ↗
- 7Vermeulen A . Physiology of the testosterone-binding globulin in man. Ann N Y Acad Sci. 1988;538(1):103‐111.3056178 10.1111/j.1749-6632.1988.tb 48855.x · doi ↗ · pubmed ↗
- 8Fiers T, Wu F, Moghetti P, Vanderschueren D, Lapauw B, Kaufman J-M. Reassessing free-testosterone calculation by liquid chromatography–tandem mass spectrometry direct equilibrium dialysis. J Clin Endocrinol Metab. 2018;103(6):2167‐2174.29618085 10.1210/jc.2017-02360 · doi ↗ · pubmed ↗