Totally endoscopic systemic atrioventricular valve re-replacement for congenitally corrected transposition of the great arteries: case report
Riku Kato, Toshiaki Ito

TL;DR
This paper reports a successful minimally invasive surgery to replace a heart valve in a patient with a rare heart condition.
Contribution
The paper presents a novel endoscopic approach for re-replacement of the systemic atrioventricular valve in adults.
Findings
Endoscopic SAVV re-replacement is feasible in adults with ccTGA.
The approach overcomes unique technical challenges and provides good outcomes.
A 47-year-old patient showed improvement after the procedure.
Abstract
Congenitally corrected transposition of the great arteries (ccTGA) is often associated with systemic atrioventricular valve (SAVV) regurgitation and the dysfunction of the systemic ventricle. We describe a case of a 47-year-old female who underwent SAVV replacement with bioprosthetic valve at 39-year-old through left thoracotomy approach. She developed dyspnoea on exertion and was recommended for surgery. We performed a totally three-dimensional endoscopic minimally invasive re-replacement of SAVV. Endoscopic replacement of SAVV for an adult is possible with an excellent view. We describe our approach which has overcome unique technical hurdles and has yielded favourable outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
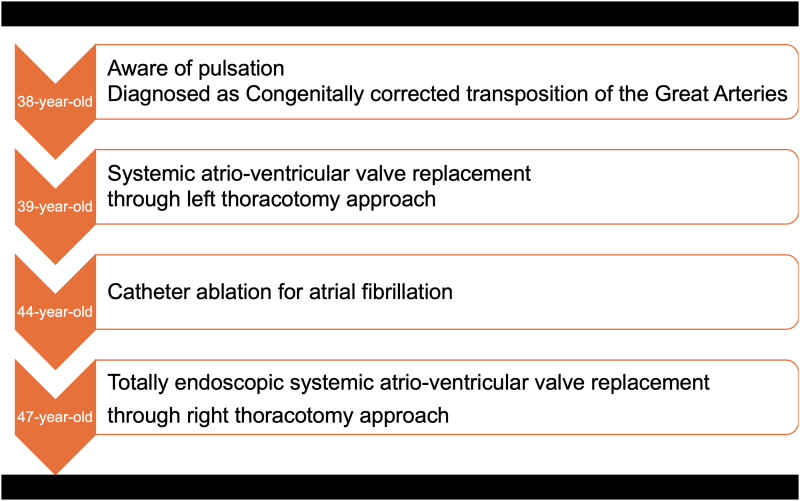 Figure 1
Figure 1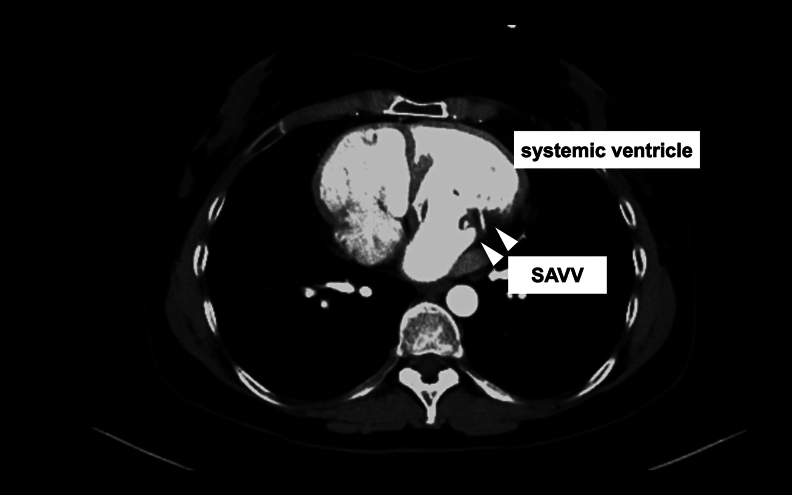 Figure 1
Figure 1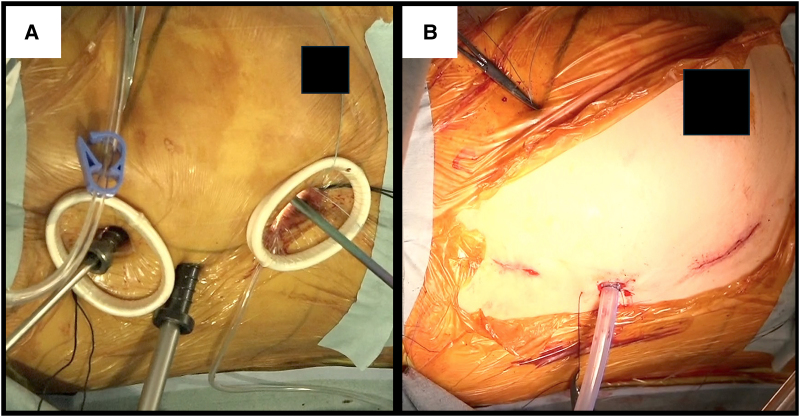 Figure 2
Figure 2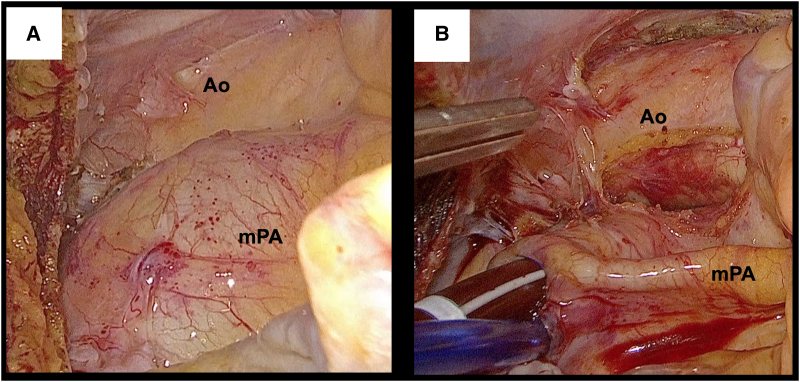 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac Structural Anomalies and Repair · Mechanical Circulatory Support Devices
Introduction
Congenitally corrected transposition of the great arteries (ccTGA) is a rare cardiac malformation characterized by double discordance. Nearly 90% of ccTGA patients have complications with other congenital heart diseases, such as ventricular septal defects and pulmonary stenosis, often requiring anatomical repairs during the infancy.^1^ However, ccTGA patients without additional cardiac complications and symptoms may not require surgery in childhood. Many of these patients must undergo systemic atrioventricular valve (SAVV) replacement in adulthood due to SAVV regurgitation. The unique anatomy of ccTGA makes securing the visualization of SAVV challenging. Herein, we report a case where a totally 3D endoscopic approach via right thoracotomy provided a good visualization of the SAVV.
Summary figure
**
Case report
A 47-year-old female with ccTGA, who undergone SAVV replacement with a bio-prosthesis (Epic 27 mm; Abbott Laboratories, IL, USA) as a 39-year-old and catheter ablation for atrial fibrillation as a 44-year-old, presented with dyspnoea on exertion. Her transthoracic echocardiography showed that biventricular function remained normal (functional left ventricular ejection fraction: 65%, functional right ventricular ejection fraction: 55%) and the end-diastolic and end-systolic diameters of the functional left ventricle were 58 and 37 mm, respectively. The mean trans-prosthetic pressure gradient was 14 mmHg, and the degree of SAVV regurgitation was moderate (Video 1). Given her symptoms, she was referred to our institution for surgical re-replacement. The index surgery was performed via left thoracotomy and left atriotomy thorough the left atrial appendage at the prior institution to address the anatomical challenge of ccTGA. During that procedure, the right jugular vein was injured when inserting a venous drainage tube, resulting in a right haemothorax. A bioprosthetic valve had been selected due to her desire for future pregnancy. Her contrast-enhanced computed tomography scan illustrated that the SAVV was vertically oriented (Figure 1, Video 2), indicating that visualization through the conventional median sternotomy approach would be challenging. Moreover, she also strongly hoped to avoid median sternotomy. Based on our experience, we anticipated that the totally endoscopic approach through the right chest with a three-dimensional (3D) endoscope could provide a better surgical view of the SAVV.
Contrast-enhanced computed tomography showed that systemic atrioventricular valve was vertically oriented (white arrow).
Under general anaesthesia, she was placed in a thirty-degree left lateral decubitus position with the right arm fixed over the head. Cardiopulmonary bypass (CPB) was established through the right groin. Distal perfusion of the right leg was performed using 6 Fr sheath because the right femoral artery was so small. A 10 mm trocar for a 3D endoscope (Karl Storz, Tuttlingen, Germany) was inserted through the fourth intercostal space. The main 4 cm incision was made at the fifth intercostal space without rib-spreading. A 2 cm incision for a left-hand instrument was placed at the third intercostal space (Figure 2A and B). The intrathoracic and intrapericardial adhesion were not severe, despite the previous haemothorax. Upon opening the pericardium, the dilated main trunk of the pulmonary artery (mPA) which was positioned to the right side of the ascending aorta prevented exposure of it (Figure 3A). Inserting a vent tube into mPA through the cranial-side window brought mPA collapsed, improving the visualization of the ascending aorta (Figure 3C). The ascending aorta was cross clamped using a flexible clamp, and cardiac arrest was achieved through antegrade cardioplegia. The vent tube, a cardioplegia needle, and the aortic clamp were inserted through the cranial-side window. Through a right-side left atriotomy, the sclerotic bioprosthetic valve was exposed with a similar view with usual endoscopic mitral valve surgeries. Although the valve was removed with scissors and cut-set-cautery, it was so tightly embedded into pannus. Therefore, it had to be divided into several segments for complete removal. Subsequently, a new mechanical valve (St. Jude Medical valve 27 mm; Abbott Laboratories, IL, USA) was placed in supra-annular position. The left atrium was closed, and the patient was weaned off CPB (Video 3). Transoesophageal echocardiogram demonstrated no paravalvular leakage.
(A) Setup of intraoperative port setting, (B) postoperative surgical wound.
3D-endoscopic view before inserting vent tube into the main trunk of the pulmonary artery (A), and after inserting vent tube (B). Ao, aorta.
Aortic cross-clamp, cardiopulmonary bypass, and operation times were 152, 232, and 295 min, respectively. She was extubated 19 h after the operation. She had an uneventful recovery and went home on a postoperative Day 8, being asymptomatic under optimal medical therapy 1 year after surgery. Her echocardiogram showed normal functions of the SAVV and the systemic ventricle.
Comment
In this patient, anatomical repair (double switch surgery) was not usually indicated for her age. When ccTGA is first diagnosed in adulthood, timely intervention to SAVV is important before deterioration of anatomical right ventricular function.^2^ Once its function has deteriorated due to SAVV regurgitation, it is difficult to return to its baseline even if surgery is performed at that time.^3^ Whereas good long-term outcomes of SAVV replacement in ccTGA patients were reported,^4^ emphasizing the importance of timely valve replacement to achieve the best outcomes.
Exposure of SAVV through median sternotomy is not necessarily easy in ccTGA because the ventricular apex is deviated to the midline, and the valve is directed towards ventral side. Left thoracotomy, as this patient underwent in index surgery, could be an option. Our experience indicated endoscopic approach through the right chest, as usual endoscopic mitral valve surgery, could be another good option to access SAVV in ccTGA with SLL (situs solitus, L-loop, L-malposition) anatomy. Venting of the main pulmonary artery, which lies on the right side of the aorta, played an important role in exposing the ascending aorta. In recent years, trans-catheter approach is also a possible option,^5^ but we report that endoscopic surgery through the right chest could be a versatile option for intervention of SAVV in ccTGA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller G-P, et al 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J 2021;42:563–645.32860028 10.1093/eurheartj/ehaa 554 · doi ↗ · pubmed ↗
- 2Acar P, Sidi D, Bonnet D, Aggoun Y, Bonhoeffer P, Kachaner J. Maintaining tricuspid valve competence in double discordance: a challenge for the paediatric cardiologist. Heart 1998;80:479–483.9930048 10.1136/hrt.80.5.479PMC 1728855 · doi ↗ · pubmed ↗
- 3Mongeon F-P, Connolly HM, Dearani JA, Li Z, Warnes CA. Congenitally corrected transposition of the great arteries ventricular function at the time of systemic atrioventricular valve replacement predicts long-term ventricular function. J Am Coll Cardiol 2011;57:2008–2017.21565637 10.1016/j.jacc.2010.11.021 · doi ↗ · pubmed ↗
- 4Deng L, Xu J, Tang Y, Sun H, Liu S, Song Y. Long-term outcomes of tricuspid valve surgery in patients with congenitally corrected transposition of the great arteries. J Am Heart Assoc 2018;7:e 008127.29874165 10.1161/JAHA.117.008127 PMC 5907565 · doi ↗ · pubmed ↗
- 5de Carvalho MM, Machado AP, Rodrigues RA, Silva JC, Cruz C, Macedo F. Transcatheter systemic atrioventricular valve-in-valve implantation in a congenitally corrected transposition of the great arteries patient. Cardiol Young 2023;33:1715–1717.36896671 10.1017/S 104795112300029 X · doi ↗ · pubmed ↗