Rare Indications of Splenectomy: A Case Series and Literature Review
Nivash Maran, Sugumar Chidambaranathan, Krishna Moorthy

TL;DR
This paper presents six rare cases where splenectomy was performed for unusual reasons like congenital bleeding disorders, pancreatitis complications, and splenic cysts.
Contribution
The study contributes a case series highlighting atypical and life-threatening indications for splenectomy that are rarely discussed in standard clinical guidelines.
Findings
Splenectomy can be life-saving in congenital bleeding disorders with spontaneous splenic hemorrhage.
Chronic pancreatitis can lead to splenic pseudocysts and rupture, requiring combined splenectomy and pancreatectomy.
Primary splenic angiosarcoma is a rare but fatal condition requiring urgent surgical intervention.
Abstract
Splenectomy is a procedure, most commonly performed for trauma, hematological disorders, and certain malignancies. Rare indications such as congenital bleeding disorders, pancreatitis complications, and splenic cysts may also warrant splenic removal, especially in life-threatening conditions or diagnostically unclear scenarios. In this retrospective descriptive case series, we report cases of six patients who underwent splenectomy for rare indications. The first case involves a 13-year-old boy with congenital afibrinogenemia who presented with signs of acute abdomen and class 3 hypovolemic shock. Computed tomography (CT) imaging of the abdomen and pelvis revealed a large perisplenic hematoma and hemoperitoneum suggestive of spontaneous hemorrhage. Despite fibrinogen replacement therapy, the patient remained hemodynamically unstable, and emergency open splenectomy was performed, which…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
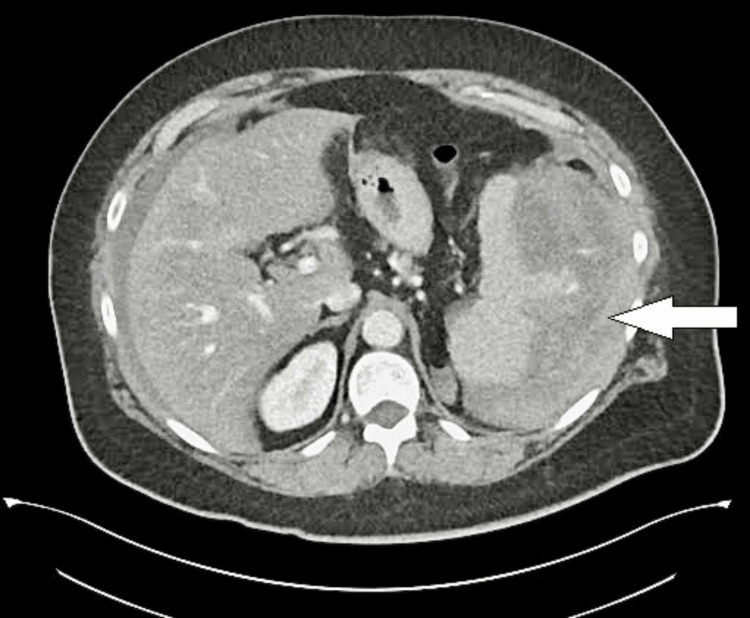 Figure 1
Figure 1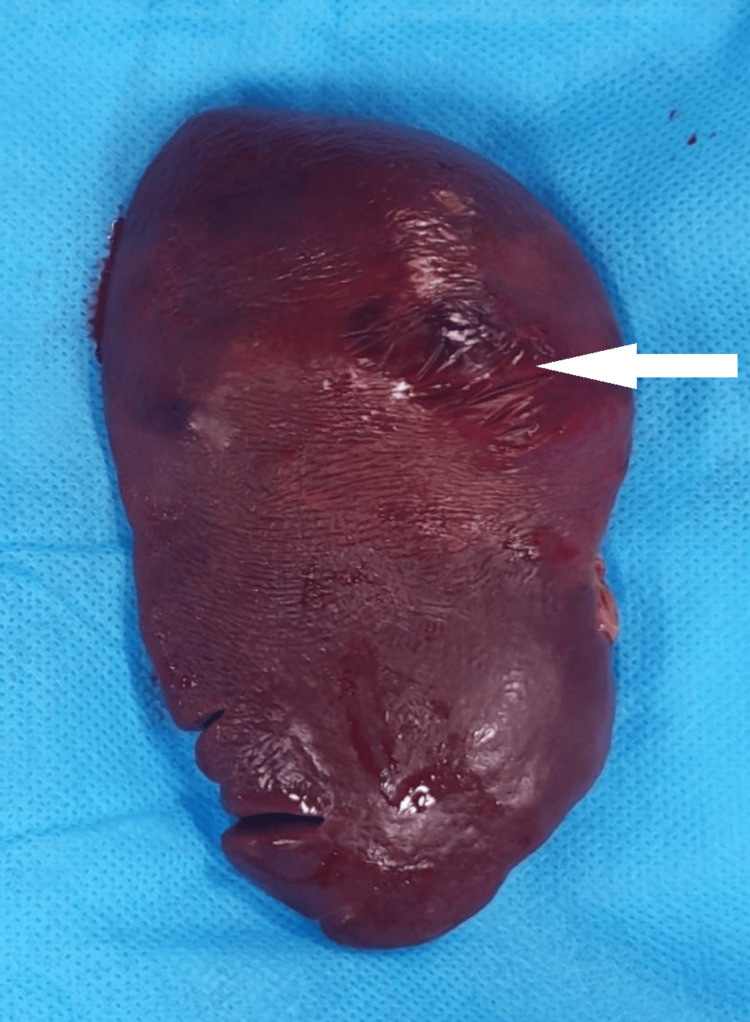 Figure 2
Figure 2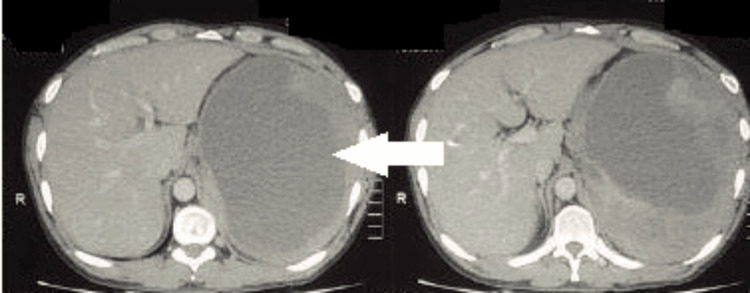 Figure 3
Figure 3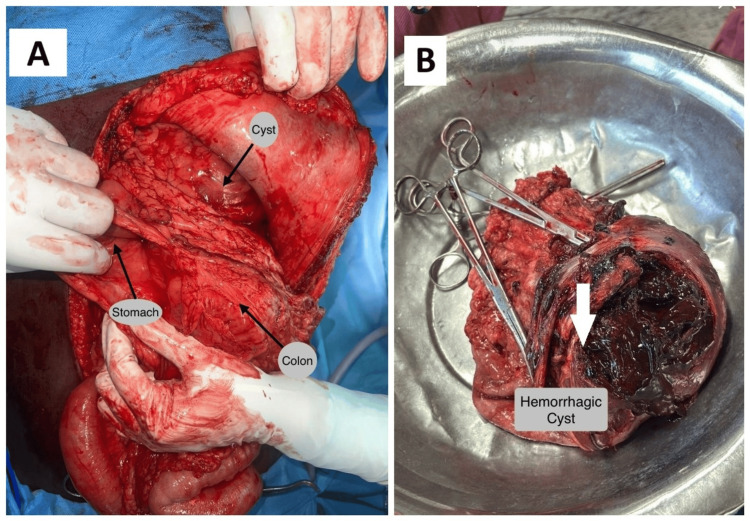 Figure 4
Figure 4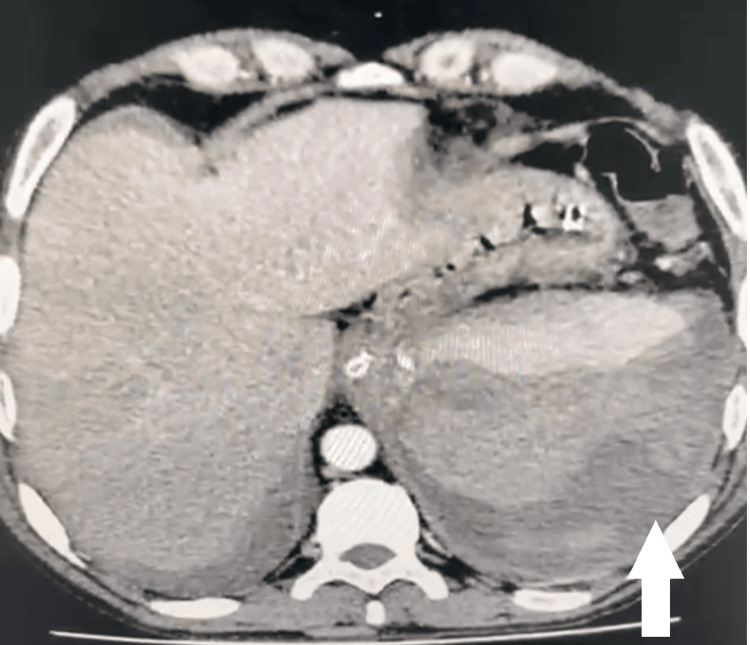 Figure 5
Figure 5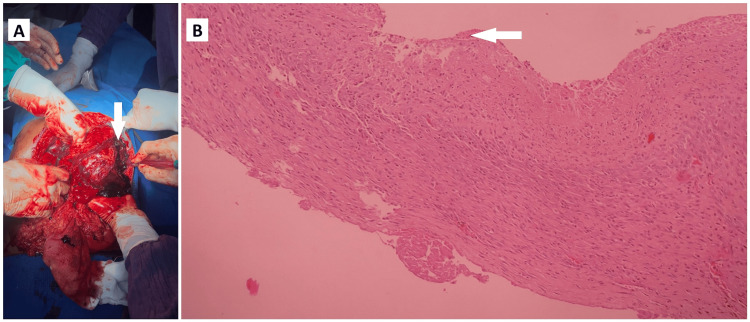 Figure 6
Figure 6 Figure 7
Figure 7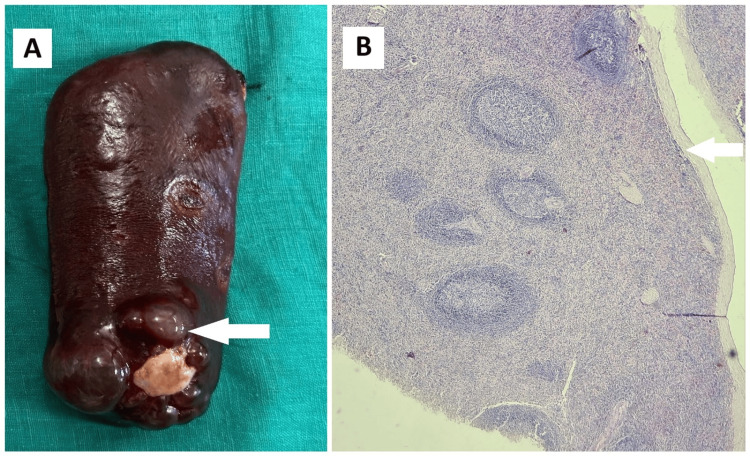 Figure 8
Figure 8 Figure 9
Figure 9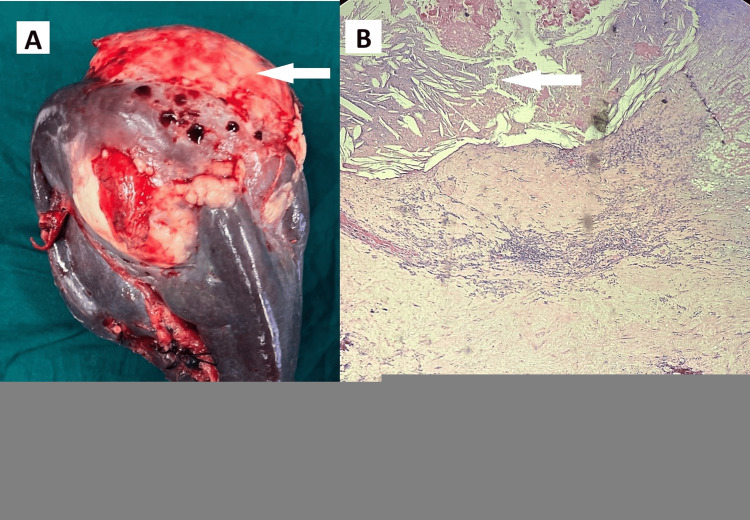 Figure 10
Figure 10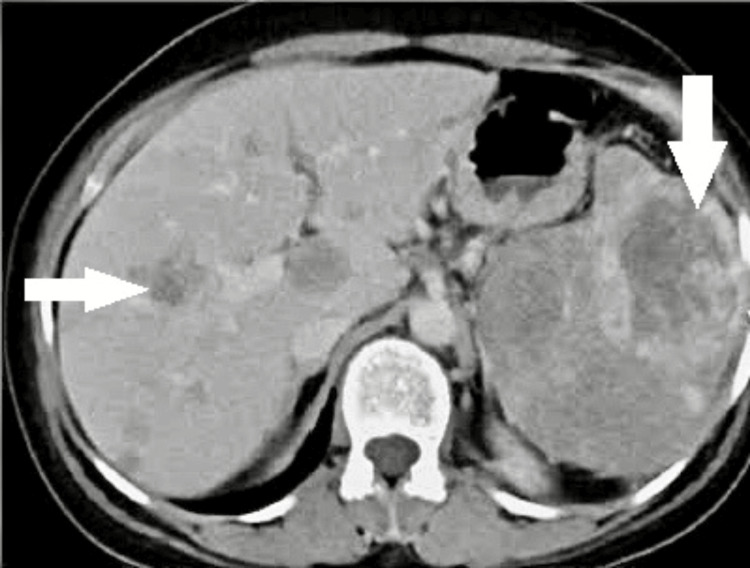 Figure 11
Figure 11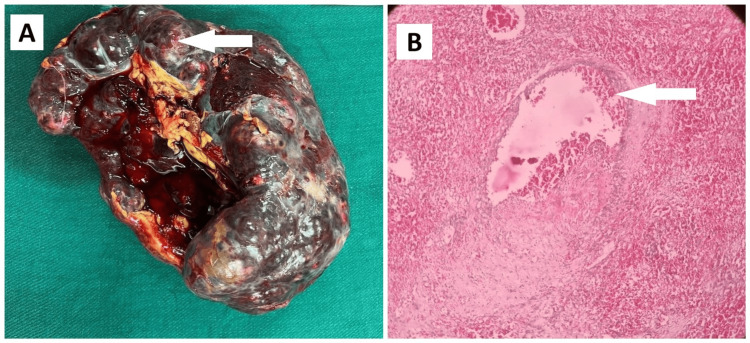 Figure 12
Figure 12| Cases | Age/Sex | Hemoglobin (g/dl) | WBC count (cells/mm3) | Platelets (x109/L) | PT (sec) | APTT (sec) | Fibrinogen (mg/dl) | Amylase (U/L) | Lipase (U/L) |
| Normal values | - | 12 to 16 | 4000-11000 | 150-400 | 11 to 14 | 25-35 | 200-400 | 23-85 | 0-160 |
| Case 1 | 13/M | 7.4 | 9800 | 210 | >60 | >180 | Undetectable | --- | --- |
| Case 2 | 39/M | 8.2 | 12800 | 330 | Normal | Normal | Normal | 420 | 695 |
| Case 3 | 45/M | 7.9 | 14500 | 280 | Normal | Normal | Normal | 385 | 740 |
| Case 4 | 25/F | 11.2 | 8700 | 250 | Normal | Normal | Normal | --- | --- |
| Case 5 | 27/F | 10.4 | 16200 | 290 | Normal | Normal | Normal | --- | --- |
| Case 6 | 44/F | 5.8 | 15600 | 110 | Prolonged | Prolonged | --- | --- | --- |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Pediatric Urology and Nephrology Studies · Hemostasis and retained surgical items
Introduction
Splenectomy is a well-established surgical intervention typically indicated for traumatic injury, hematologic disorders such as immune thrombocytopenic purpura (ITP) and hereditary spherocytosis, and certain malignancies involving the spleen [1,2]. In these contexts, splenectomy offers both therapeutic and, at times, diagnostic benefits. However, less frequently encountered scenarios also warrant splenectomy, often presenting as diagnostic dilemmas or as complications requiring urgent surgical management [3].
Among these, rare indications are congenital coagulopathies such as afibrinogenemia, an autosomal recessive inherited condition characterized by absent or severely reduced fibrinogen levels, where spontaneous hemorrhagic events may involve the spleen and become life-threatening [4-7]. Acute or chronic pancreatitis can also result in perisplenic complications, including intrasplenic pseudocyst formation and eventual rupture due to enzymatic digestion or localized vascular injury [8-11]. Furthermore, primary splenic cysts, although mostly benign and asymptomatic, can enlarge, become symptomatic, get infected, or be misdiagnosed as parasitic or neoplastic lesions, thereby necessitating splenectomy [12-14]. Finally, primary splenic angiosarcoma, an extremely rare and aggressive vascular tumor, may present with spontaneous rupture and widespread metastasis, leading to rapid deterioration and death if not promptly addressed [15,16].
Over the past few decades, the overall incidence of splenectomy has declined due to advances in imaging, interventional radiology, and minimally invasive splenic preservation techniques. In resource-limited or emergent settings, radiological uncertainty and clinical instability often necessitate early surgical exploration and splenic removal. This case series describes six patients who underwent splenectomy for such uncommon conditions, highlighting the diverse presentations and emphasizing the importance of considering splenectomy even in non-traditional clinical scenarios. A brief literature review is included to contextualize these cases and underline the diagnostic and therapeutic value of splenectomy in selected patients.
Case presentation
Case 1: Congenital afibrinogenemia with spontaneous splenic hemorrhage
A 13-year-old boy, with congenital afibrinogenemia diagnosed during childhood, and on irregular treatment and follow-up, presented with sudden-onset left upper quadrant pain, dizziness and abdominal distension for one day. On presentation, he was hypotensive and anemic with elevated prothrombin time and activated partial thromboplastin time (>180 sec) with undetectable serum fibrinogen (Table 1).
CT imaging of the abdomen and pelvis revealed a large hypodense collection sized 7x8x5 cm noted around the spleen with moderate hemoperitoneum (Figure 1).
Congenital afibrinogenemia with spontaneous splenic hemorrhageContrast enhanced CT abdomen and pelvis showing moderate hemoperitoneum with splenic parenchymal rupture. The white arrow indicates the splenic parenchymal rupture.
Even after administration of cryoprecipitate and fibrinogen concentrates, the patient remained hemodynamically unstable. Emergency open splenectomy was performed. Intraoperative findings included two liters of hemoperitoneum and a friable spleen with capsular rupture (Figure 2).
Congenital afibrinogenemia with spontaneous splenic ruptureGross specimen showing splenic parenchymal rupture. The white arrow shows parenchymal laceration.
Postoperative recovery was uneventful, and he was advised long-term hematological follow-up and vaccination as per standard guidelines.
Case 2: Rupture of intrasplenic pseudocyst in chronic pancreatitis
A 39-year-old man diagnosed with chronic alcoholic pancreatitis three years ago, presented with abdominal discomfort and early satiety for five days. CT imaging of abdomen and pelvis showed a well defined hypodense cystic lesion of size 10x13x12 cm seen involving upper pole of spleen with active pooling of contrast into the splenic parenchyma and a small pseudocyst 3x2.5 cm in the tail of pancreas with mild hemoperitoneum, suggesting the possibility of rupture (Figure 3).
Intrasplenic pseudocyst rupture in chronic pancreatitisAxial CT abdomen showing a large hypodense cystic lesion within the upper pole of the spleen with signs of rupture (white arrow).
On presentation he was anemic, resuscitation was done with blood and blood products, and in view of aggravation of symptoms, he underwent emergency open splenectomy with distal pancreatectomy. Intraoperatively, the spleen showed a pseudocyst adjacent to the pancreatic tail, with surrounding fibrosis (Figure 4A).
Ruptured splenic pseudocyst (A) Intraoperative picture showing the splenic pseudocyst; (B) Gross specimen of the spleen showing the ruptured hemorrhagic pseudocyst (marked with white arrow).
Figure 4B shows gross specimen showing hemorrhagic cyst. The patient recovered uneventfully.
Case 3: Intrasplenic pseudocyst rupture
A 45-year-old man, a known case of alcohol induced chronic pancreatitis diagnosed one year ago, presented with complaints of diffuse abdominal pain for one day. He was hypotensive and anemic at the time of admission. Contrast enhanced CT abdomen and pelvis showed a large subcapsular collection 12x11x9 cm in the posterior aspect of the spleen tracking along left paracolic gutter with evidence of contrast extravasation near the hilum (Figure 5).
Intrasplenic pseudocyst rupture in chronic pancreatitisAxial CT showing subcapsular splenic hematoma with rupture (white arrow).
He was planned for emergency laparotomy and intraoperative findings were ruptured splenic hematoma with moderate hemoperitoneum (Figure 6A).
Splenic pseudocyst rupture(A) Intraoperative picture showing splenic parenchymal rupture with hemoperitoneum (white arrow); (B) Histopathology image showing pancreatic parenchyma with pseudocyst without an epithelial lining (white arrow).
He underwent distal pancreatosplenectomy. HIs postoperative period was uneventful. Histopathological examination showed pancreatic parenchyma with pseudocyst (Figure 6B).
Case 4: Large primary splenic cyst
A 25-year-old lady presented with left upper quadrant vague abdomen pain for four months. CT imaging revealed a 6.9x3.9 cm multiloculated cystic lesion in the superior pole of spleen with thin non-enhancing septations with the possibility of a splenic cyst (Figure 7).
Primary splenic cystContrast enhanced CT abdomen image showing a multiloculated cyst in the superior pole of the spleen (white arrow).
Since she was symptomatic and in a diagnostic dilemma, she underwent elective laparoscopic splenectomy. Gross examination showed a multiloculated cystic mass (Figure 8A).
Primary splenic cyst(A) Gross specimen of the spleen with the cyst (white arrow); (B) Histopathological image showing cuboidal to columnar cyst wall lining epithelium with splenic parenchyma (white arrow).
Histopathology confirmed a primary benign epithelial splenic cyst (Figure 8B). The patient recovered uneventfully in the postoperative period.
Case 5: Post-drainage infection of primary splenic cyst
A 27-year-old female patient presented with left hypochondriac pain and intermittent fever for one week. She was already diagnosed as a case of splenic cyst for which percutaneous drainage (PCD) was done one month before this presentation in an outside hospital. CT imaging of abdomen and pelvis showed a well-defined hypodense non-enhancing cystic lesion 7.8x8 cm and calcification in the wall of superior pole of spleen (Figure 9) suggestive of splenic abscess.
Primary splenic cyst with infectionContrast-enhanced CT abdomen showing a cystic lesion in the spleen (white arrow).
She was symptomatic with signs of infection in the form of leukocytosis (Table 1) which might have been introduced from an external source related to previous catheter insertion into the splenic cyst, and hence elective open splenectomy was planned and performed. Intraoperatively, dense adhesions were noted around the spleen. Figure 10A shows gross specimen of the spleen with abscess cavity.
Splenic cyst with an infected complication(A) Gross specimen showing spleen with abscess cavity (white arrow); (B) Histopathological image showing the cyst wall with cholesterol clefts and inflammatory exudates (white arrow).
Histopathology revealed a splenic abscess (Figure 10B).
Case 6: Primary splenic angiosarcoma with spontaneous rupture
A 44-year-old female patient presented to the emergency department with sudden onset abdominal pain, hypotension, and severe anemia. CT imaging of the abdomen and pelvis revealed multiple hetero-dense lesion with internal hemorrhage noted in both lobes of the liver, with the largest measuring 6.3x6.9 cm in segment eight of the liver and also with multiple hetero-dense lesion in the spleen, with the largest measuring 5.2x5 cm, and dense free fluid was also noted (Figure 11).
Primary splenic angiosarcoma with spontaneous ruptureContrast-enhanced CT scan showing multiple heterogeneous lesions in both liver and spleen with hemoperitoneum. The white arrows show the liver metastases and splenic lesion.
Since the patient developed signs of peritonism and hemodynamic instability, an urgent laparotomy was performed. Intraoperatively, hemoperitoneum of around 2.5 liters was noted. The spleen was grossly enlarged and friable with rupture noted near the superior pole. Multiple hyper-vascular lesions were noted in both the spleen and the liver. Figure 11 shows a metastatic lesion in the liver. Splenectomy was performed. Diffuse ooze was noted from the diaphragmatic attachment of the spleen in spite of adequate hemostatic measures. So packing was done in the splenic fossa which was removed in the second look laparotomy after 48 hrs.
Figure 12A shows the gross specimen, demonstrating that the entire spleen was replaced by the hyper vascular mass.
Primary splenic angiosarcoma(A) Gross specimen showing spleen with hyper vascular necrotic tumor (white arrow); (B) Histopathology image showing dilated vascular channels with intervening pleomorphic cells (white arrow).
Histopathology was consistent with angiosarcoma of the spleen with strong positivity of ERG (ETS family of transcription factor expressed in endothelial cells) in tumor cells and Ki67 index of 50% (Figure 12B). She had already presented with distant metastases of the liver and bones at the time of diagnosis. Unfortunately, she succumbed to the disease on postoperative day 10.
Discussion
Splenectomy is most often performed for trauma and hematological disorders such as immune thrombocytopenic purpura (ITP) or hereditary spherocytosis, and certain malignancies [1,2]. However, rare conditions may also necessitate splenic removal, either due to life-threatening complications or diagnostic uncertainty [3]. Our case series highlights a diverse spectrum of such uncommon but significant indications: congenital afibrinogenemia, pancreatitis-related splenic complications, primary splenic cyst, and ruptured angiosarcoma of the spleen.
Congenital afibrinogenemia is a rare bleeding disorder characterized by absent or severely low fibrinogen levels. It is an autosomal recessive disease that results from a mutation of one of the three genes (FGA, FGB, FGG) that code the three polypeptide chains of fibrinogen, disrupting its synthesis and stability, ultimately resulting in life-threatening hemorrhage [4]. While spontaneous hemorrhage is well known, visceral hemorrhage, especially with splenic involvement, is rare and potentially fatal [5,6]. Bleeding episodes in patients with afibrinogenemia are treated with fibrinogen concentrates as the first-line therapy. Cryoprecipitate and fresh frozen plasma are other options when fibrinogen concentrates are unavailable. A growing body of evidence shows that human fibrinogen concentrates are safe and effective; however, they may produce allergic or hypersensitivity reactions. These can range from mild episodes of skin rashes /urticaria to life-threatening anaphylactic reactions. We resuscitated our patient with intravenous fluids, blood and fibrinogen concentrates. But the patient was hemodynamically unstable with signs of peritonitis. In the first case, the failure of conservative measures warranted splenectomy, which proved lifesaving. Recent studies suggest liver transplantation as one of the novel options in treating congenital afibrinogenemia in future [7].
Pancreatitis is a common condition with well-documented complications. Splenic involvement in chronic pancreatitis, particularly in the form of pseudocysts, is uncommon [8]. The pancreas and the spleen are anatomical allies, and for this reason, complications involving the spleen can occur as a result of pancreatitis. The pancreatic tail, splenic hilum, its associated vessels, and the peritoneum of the anterior pancreatic surface are vital in allowing leaked proteolytic pancreatic enzymes. This causes enzymatic degradation of splenic parenchyma and opening up of red pulp with rupture of trabecular vessels, thereby causing subcapsular splenic hematoma leading to spontaneous rupture. There are case reports which have demonstrated that pancreatic pseudocysts can result in splenic penetration associated with hemorrhage and mortality [9]. Although percutaneous or endoscopic drainage may be attempted in selected cases, emergency splenectomy combined with distal pancreatectomy remains the treatment of choice when bleeding, rupture, or infection occurs [10,11].
Primary splenic cysts are uncommon, accounting for <10% of all non-parasitic splenic cysts. They are typically true cysts, meaning they are lined by epithelium and are distinct from secondary (pseudocysts) which usually occur after trauma or inflammation and lack an epithelial lining. Primary splenic cysts can be either congenital (epithelial/epidermoid) or neoplastic (hemangioma/lymphangioma), or parasitic (echinococcal) [12]. They may present with abdominal discomfort or be complicated by infection, hemorrhage, or rupture. Congenital epithelial splenic cysts are often discovered incidentally and if symptomatic usually warrant surgical intervention (splenectomy) [13,14]. In our cases, splenectomy provided both a definitive diagnosis and relief from compressive symptoms. Most epithelial cysts are benign, and elective laparoscopic splenectomy is a safe approach when indicated.
Primary splenic angiosarcoma is an extremely rare and aggressive malignancy with <200 cases reported globally [15]. It most often presents in the sixth decade but may occur earlier. It commonly presents with nonspecific symptoms or as a spontaneous splenic rupture, often leading to delayed diagnosis [16,17]. Metastases to the liver, lungs, or bones are frequently present at diagnosis and the prognosis is usually poor. While splenectomy is essential for bleeding control and histological diagnosis, overall survival remains limited. Diagnosis requires histopathologic evaluation, with immunohistochemical markers such as CD31, CD34, and ERG confirming endothelial origin [18]. Despite surgical resection, prognosis remains poor, with median survival of less than 12 months due to early metastasis and tumor aggression. In the sixth case, the patient underwent emergency surgery but succumbed in the early postoperative period and developed widespread metastases, reflecting the tumor’s aggressive biology.
In our series, splenectomy served several important purposes: hemorrhage control, removal of infected or ruptured cysts, and definitive diagnosis in uncertain or malignant cases. Each case reflects the utility of splenectomy beyond conventional indications and highlights the necessity of early surgical intervention when conservative treatment fails or imaging findings are concerning. Furthermore, histopathology proved essential in confirming the underlying pathology, especially in distinguishing between benign cysts and neoplastic processes.
A high index of suspicion, appropriate imaging, and timely surgical consultation are key in managing these rare splenic conditions. In selected patients, a multidisciplinary team including surgeons, hematologists, gastroenterologists, and radiologists can significantly improve outcomes.
Conclusions
Although splenectomy is most commonly performed for well-established indications such as trauma, hematologic disorders, and malignant involvement of the spleen, this case series highlights the indispensable role of splenectomy in a variety of rare, atypical, and diagnostically challenging conditions. Each case presented demonstrates how splenectomy served either as a life-saving emergency procedure or as a definitive diagnostic and therapeutic intervention when conservative or non-surgical measures failed.
Congenital afibrinogenemia with spontaneous splenic rupture illustrates how inherited bleeding disorders, although rare, can present with life-threatening visceral hemorrhage requiring immediate surgical management. In the context of chronic pancreatitis, splenic pseudocysts represent an uncommon but serious complication that can lead to spontaneous rupture and massive hemorrhage, necessitating prompt surgical intervention, often in combination with distal pancreatectomy. Primary splenic cysts, while typically benign, can become symptomatic, become infected following drainage, or mimic parasitic or neoplastic lesions radiologically, further justifying splenectomy for definitive management. Splenic angiosarcoma represents an extreme example of an aggressive vascular malignancy that frequently presents with spontaneous rupture and advanced metastasis. In such cases, splenectomy may offer temporary hemodynamic stabilization and histologic confirmation, although long-term prognosis remains poor.
This series emphasizes the critical importance of maintaining a broad differential diagnosis when evaluating splenic pathology, particularly in the setting of atypical clinical or radiologic features. Early surgical consultation should be considered when patients present with signs of hemodynamic compromise, abdominal pain of unclear origin, or when imaging suggests cystic, vascular, or hemorrhagic lesions of the spleen. Moreover, the intraoperative and histopathological findings from splenectomy often provide diagnostic clarity in cases where non-invasive methods are inconclusive. Ultimately, timely recognition of these rare but significant conditions and an appropriately tailored surgical approach can result in improved patient outcomes. Multidisciplinary collaboration between surgeons, radiologists, hematologists, and pathologists is essential in managing such complex presentations. While the spleen is often considered expendable in surgical practice, its diseases-especially the rare ones-can challenge even experienced clinicians. Splenectomy, when appropriately indicated, remains a powerful tool in the diagnostic and therapeutic armamentarium of surgeons managing complex abdominal conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Indications for surgery in non-traumatic spleen disease Open Access Maced J Med Sci Coco D Leanza S 29582960720193184446410.3889/oamjms.2019.568PMC 6901870 · doi ↗ · pubmed ↗
- 2Splenectomy for hematologic disorders Arch Surg Schwartz SI Bernard RP Adams JT Bauman AW 3383471011970546546910.1001/archsurg.1970.01340260242036 · doi ↗ · pubmed ↗
- 3Case report of a splenectomy secondary to infectious mononucleosis in a 16-year-old female J Surg Case Rep Wilson GG Rennie K 02025202510.1093/jscr/rjaf 420PMC 1220194440575064 · doi ↗ · pubmed ↗
- 4Bleeding and thrombosis in 55 patients with inherited afibrinogenaemia Br J Haematol Lak M Keihani M Elahi F Peyvandi F Mannucci PM 20420610719991052004210.1046/j.1365-2141.1999.01681.x · doi ↗ · pubmed ↗
- 5Spontaneous splenic rupture in a patient with congenital afibrinogenemia Turk Pediatri Ars Arcagök BC Özdemir N Tekin A 2472494920142607867010.5152/tpa.2014.1070 PMC 4462307 · doi ↗ · pubmed ↗
- 6Rare bleeding disorders in children: identification and primary care management Pediatrics Acharya SS 88289213220132412747510.1542/peds.2012-3662 · doi ↗ · pubmed ↗
- 7Liver transplantation as a novel strategy for resolution of congenital afibrinogenemia in a pediatric patient J Thromb Haemost Corrales-Medina FF Miloh T O'Farrell C Andrews DM Tekin A De Angulo G 323232351820203289045410.1111/jth.15090 PMC 7756576 · doi ↗ · pubmed ↗
- 8Splenic parenchymal complications in pancreatitis JOP Patil PV Khalil A Thaha MA 287291122011 https://pubmed.ncbi.nlm.nih.gov/21546711/21546711 · pubmed ↗