PPP2R1A Mutation: A Critical Amplifier for Immune Checkpoint Blockade Therapy Efficacy
Yuanzhuo Gu, Zhengkui Zhang, Fangfang Zhou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
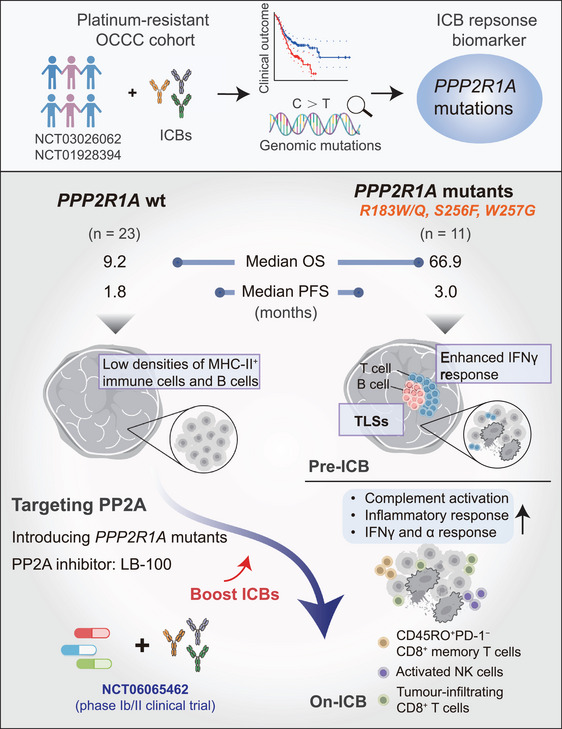 FIGURE 1
FIGURE 1- —National Natural Science Funds of China
- —The Natural Science Foundation of Zhejiang Province, China
- —Suzhou Innovation and Entrepreneurship Leading Talent Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Ovarian cancer diagnosis and treatment · Ferroptosis and cancer prognosis
1
In a recent paper published in Nature [1], Dai et al. revealed that PPP2R1A mutations in ovarian clear cell carcinoma (OCCC) are linked to superior survival following immune checkpoint blockade (ICB), driven by enhanced interferon (IFNγ) signaling and pre‐existing tertiary lymphoid structures (TLSs) that foster robust T‐cell immunity. This work nominates PPP2R1A as a promising therapeutic target to potentiate ICB efficacy across cancer types.
Despite the clinical impact of ICBs on various cancers, their efficacy in ovarian cancer remains limited, with even the most responsive OCCC subtype showing only a 15% response rate. This is underscored by the recent finding that durvalumab (anti‐PD‐L1) failed to improve progression‐free survival (PFS) or overall survival (OS) compared to chemotherapy in the MOCCA trial, despite some symptomatic improvement. Furthermore, traditional biomarkers, including PD‐L1 expression, tumor mutation burden (TMB), and BRCA1/2 status, have proven inadequate in predicting ICB responses of OCCC, highlighting the pressing need to discover novel molecular determinants of response. The observed superiority of combination therapies over ICB monotherapy suggests a promising path forward. For instance, the combination of sintilimab (anti‐PD‐1) with bevacizumab (anti‐VEGF) significantly extended median PFS to 13.8 months versus 2.0 months with monotherapy [2], with a similar benefit observed for the nivolumab and ipilimumab combination in trial NCT04969887 of OCCC. This paradigm shift toward combinations underscores the need to identify which patients are most likely to benefit. In this context, the role of specific genetic alterations is gaining prominence. Beyond the established link between pathogenic POLE/POLD1 mutations and high TMBs or SETD2_Y1666 mutation, which modulate the tumor‐immune microenvironment [3], emerging evidence points to mutation‐specific responses. These collective findings illuminate two critical facets of OCCC immunotherapy: the necessity of rational combination strategies and the heterogeneity of treatment responses driven by distinct molecular features.
This study also initiated from the genomic fidelity of clinical cohort, according to 34 patients with platinum‐resistant OCCC receiving ICB therapy (NCT03026062 and NCT01928394), 11 cases (32.4%) were found to carry PPP2R1A gene mutations responded better in ICB treatment, predominantly at the R183 hotspot (81.8%). The mutations, encoding a scaffold subunit of protein phosphatase 2A (PP2A), were associated with a remarkable survival benefit and achieved a median OS of 66.9 months with ICB, seven times longer than that of the wild type group (9.2 months) (log‐rank p = 0.031). This effect was independent of cancer type (validated in pan‐cancer cohort) and co‐occurring mutations such as ARID1A, establishing PPP2R1A mutations as a highly specific and potent predictive biomarker for ICB, a finding that addresses a critical gap in OCCC precision immunotherapy (Figure 1).
Cancer patients with PPP2R1A mutations benefit more from ICB treatment. Cancer patients with PPP2R1A mutations are associated with markedly prolonged OS and PFS following ICB treatment. The upper panel reveals how PPP2R1A mutation was identified, through two clinical trials (NCT03026062 and NCT01928394) of 34 patients with platinum‐resistant OCCC receiving ICB therapy. Clinical outcomes and genomic mutations were analyzed to identify the key biomarkers for ICB responses. The lower panel illustrates that the mechanisms of PPP2R1A mutations responded better in pre‐ and post‐ICB treatment. PPP2R1A mutant tumors exhibited enhanced IFNγ response, pre‐existing TLSs before ICB treatment, more immune infiltration, including CD8+ T cells and activated NK cells, and an expansion of CD45RO+CD8+ memory T cells post‐ICB. In contrast, PPP2R1A wild‐type tumors exhibited low densities of MHC‐II+ immune cells and B cells pre‐ICB treatment. Preclinical studies in vitro and in vivo suggest that targeting PP2A (a multimeric phosphatase with PPP2R1A‐ecoded scaffold) can boost ICB efficiency in tumors with wild‐type PPP2R1A, mainly through (1) knocking down or CRISPR‐editing wild‐type PPP2R1A, (2) introducing the mutant form, or (3) applying the PP2A inhibitor LB‐100. Currently, a Phase Ib/II clinical trial (NCT06065462) of ICB and LB‐100 combined therapy is conducting in OCCC patients without somatic PPP2R1A mutations.
Transcriptome (*n *= 29) and CO‐Detection by indEXing (CODEX) imaging (n = 28) demonstrated that PPP2R1A‐mutant tumors possess a pre‐existing, immunologically favorable microenvironment. Prior to ICB, these tumors exhibited IFNγ pathway enrichment, activated adaptive immune responses, higher densities of major histocompatibility complex (MHC)‐II^+^ immune cells and proliferative B cells (CD20^+^ Ki‐67^+^), and the presence of TLSs supporting B‐ and T‐cell activity. TLSs have been reported to be associated with good ICB response [4]. Post‐ICB, these patients showed further activation of key immune pathways (inflammatory response, complement pathway, and IFN‐α response), expansion of CD45RO^+^ CD8^+^ memory T cells and activated NK cells, along with heightened T cell receptor (TCR)/ B cell receptor (BCR) richness, indicating successful engagement and diversification of the immune response. In contrast, the wild‐type group lacked these features and failed to sustain responses.
The feasibility of targeting PPP2R1A to enhance immunotherapy was confirmed in preclinical models. Genetic perturbation of PPP2R1A (knockdown, mutation introduction, and CRISPR editing), or its pharmacological inhibition with LB‐100 [5], significantly sensitized tumor cells to immune attack. In vitro models revealed that the knockdown or mutation of PPP2R1A in tumor cells enhanced their sensitivity to killing by B7H3 chimeric antigen receptor T (CAR‐T) cells (with a 50% increase in apoptosis rate). In a humanized patient‐derived xenograft (PDX) model, mutant PPP2R1A tumors responded significantly to anti‐PD‐L1 therapy, with a 50% reduction in tumor weight (p < 0.0001). The PP2A inhibitor LB‐100 effectively mimicked the PPP2R1A mutation phenotype and synergized with ICB, supporting the launch of Phase Ib/II clinical trials (NCT06065462) to evaluate ICB combined with PP2A inhibition.
The study is limited by its sample size, which constrained the statistical power of subgroup analyses (e.g., only 4 AKT‐mutant cases), and the small number of PPP2R1A‐mutant cases in external validation cohorts (only four in the melanoma subgroup). These limitations hinder robust independent analyses and affect conclusion reliability. While PPP2R1A mutations are linked to an improved immune microenvironment (e.g., stronger IFNγ signaling and more T‐cell infiltration), the precise mechanisms by which PP2A function loss regulates immune pathways remain unclear. Additionally, the synergistic or independent interactions between PPP2R1A mutations and other known markers remain unknown, which is worth further exploration.
In summary, this paper reveals that the transformation of PPP2R1A from a mutational marker to a therapeutic target represents a paradigm shift in predicting and enhancing ICB efficacy, especially in OCCC. Key future directions include: (1) Elucidating the direct molecular mechanisms by which PP2A inhibition rewires tumor‐immune cell crosstalk, particularly its impact on T‐cell function and exhaustion; (2) Determining whether PPP2R1A mutation status can synergize with or act independently of existing biomarkers like TMB and PD‐L1 to refine patient stratification; (3) Validating its predictive power in large, prospective clinical trials across multiple cancer types. The ongoing clinical translation of PP2A inhibitors as “immune sensitizers” is promising, especially for wild‐type PPP2R1A patients in Phase Ib/II trials. This research trajectory holds significant potential to guide treatment for a broader population of cancer patients receiving immunotherapy, hoping it will bring therapeutic guidance to more cancer patients receiving or about to receive ICB treatment.
Author Contributions
Y.G. conceived and drafted the manuscript. Y.G. and Z.Z. drew the figure. Z.Z. and F.Z. discussed and revised the manuscript. All authors have read and approved the article.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Y. Dai , A. Knisely , M. Yano , et al., “PPP 2R 1A Mutations Portend Improved Survival After Cancer Immunotherapy,” Nature 644 (2025): 537–546.40604275 10.1038/s 41586-025-09203-8PMC 12350166 · doi ↗ · pubmed ↗
- 2Z. Peng , H. Li , Y. Gao , et al., “Sintilimab Combined With Bevacizumab in Relapsed or Persistent Ovarian Clear Cell Carcinoma (INOVA): A Multicentre, Single‐Arm, Phase 2 Trial,” Lancet Oncology 25 (2024): 1288–1297.39276785 10.1016/S 1470-2045(24)00437-6 · doi ↗ · pubmed ↗
- 3X. Ma , N. Riaz , R. M. Samstein , et al., “Functional Landscapes of POLE and POLD 1 Mutations in Checkpoint Blockade‐Dependent Antitumor Immunity,” Nature Genetics 54 (2022): 996–1012.35817971 10.1038/s 41588-022-01108-w PMC 10181095 · doi ↗ · pubmed ↗
- 4B. A. Helmink , S. M. Reddy , J. Gao , et al., “B Cells and Tertiary Lymphoid Structures Promote Immunotherapy Response,” Nature 577 (2020): 549–555.31942075 10.1038/s 41586-019-1922-8PMC 8762581 · doi ↗ · pubmed ↗
- 5W. S. Ho , H. Wang , D. Maggio , et al., “Pharmacologic Inhibition of Protein Phosphatase‐2A Achieves Durable Immune‐Mediated Antitumor Activity When Combined With PD‐1 Blockade,” Nature Communications 9 (2018): 2126.10.1038/s 41467-018-04425-z PMC 597435029844427 · doi ↗ · pubmed ↗