Metastatic Pleomorphic Adenoma: A Systematic Review
Alberto Jose Peraza-Labrador, Doreen Palsgrove, Marcelo Villacis, Victoria Woo, Nestor R. Gonzalez, Andreas Ciscato, Justin Bishop

TL;DR
Metastatic pleomorphic adenoma is a rare benign tumor that behaves like a malignancy by spreading to other body parts, requiring careful diagnosis and long-term monitoring.
Contribution
This systematic review compiles and analyzes 95 cases of metastatic pleomorphic adenoma to better understand its clinical features and outcomes.
Findings
The parotid gland is the most commonly affected site, with 75.8% of cases.
Bone and cervical lymph nodes are the most frequent metastatic sites, with rates of 21.88% and 20.31%, respectively.
Approximately 52.7% of patients were alive at the time of follow-up, while 8.4% died from the disease.
Abstract
Metastatic pleomorphic adenoma (MPA) is a benign-appearing pleomorphic adenoma that spreads to regional and distant sites, such as lymph nodes, lungs, or bones, despite lacking malignant features histologically. A systematic review of documented case reports and case series of metastatic pleomorphic adenoma is presented. Searches were conducted across various databases to identify articles published from 1953 to December 2024. The variables included were gender, age, symptoms, type of gland, histological features, molecular studies, type of treatment, and follow-up. Of the 95 cases reported, 58.8% affected females, and 41.1% were males. The average age for MPA was 49.9 years, and the mean size was 2.4 cm. The parotid gland was the most commonly affected, accounting for 75.8% of cases, followed by the submandibular gland with 13.6%. The treatment for the (benign) pleomorphic adenoma…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
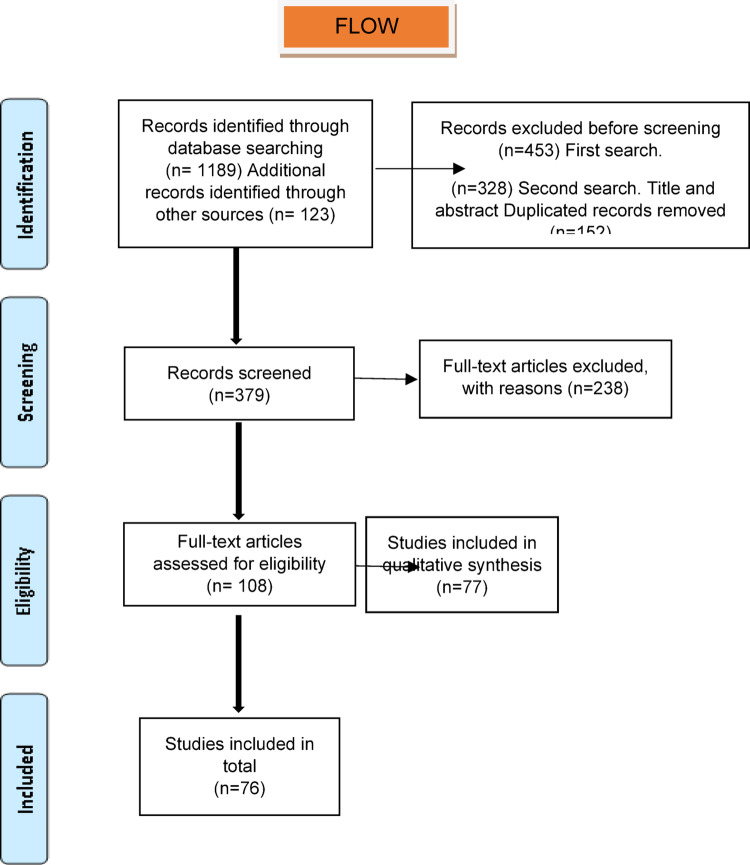 Figure 1
Figure 1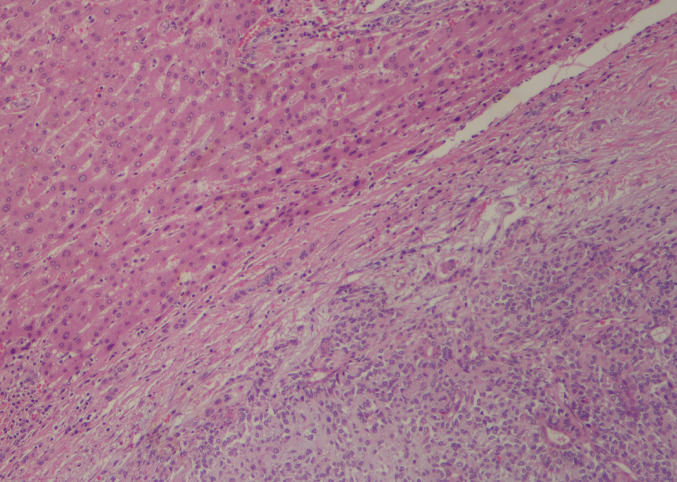 Figure 2
Figure 2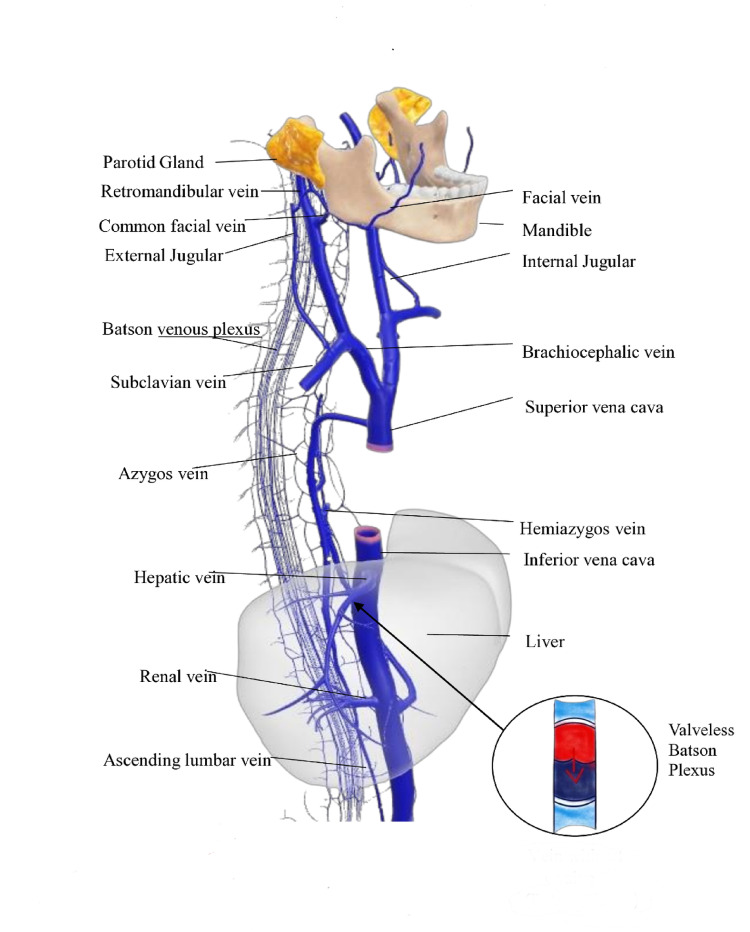 Figure 3
Figure 3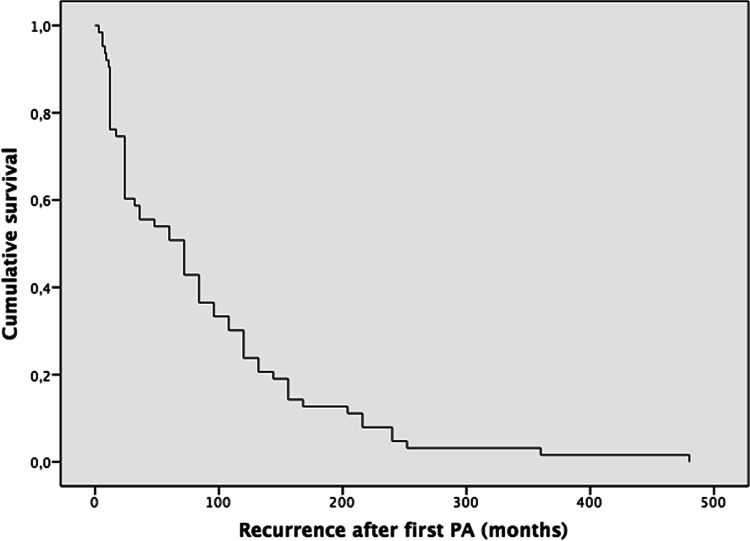 Figure 4
Figure 4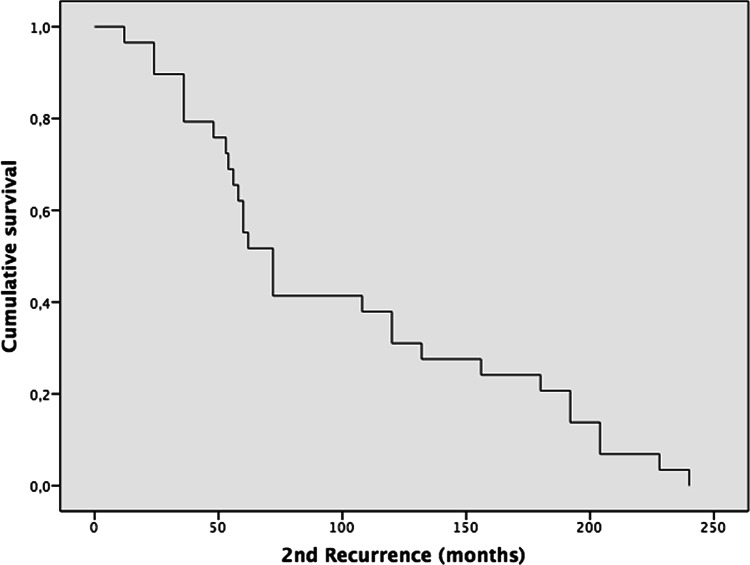 Figure 5
Figure 5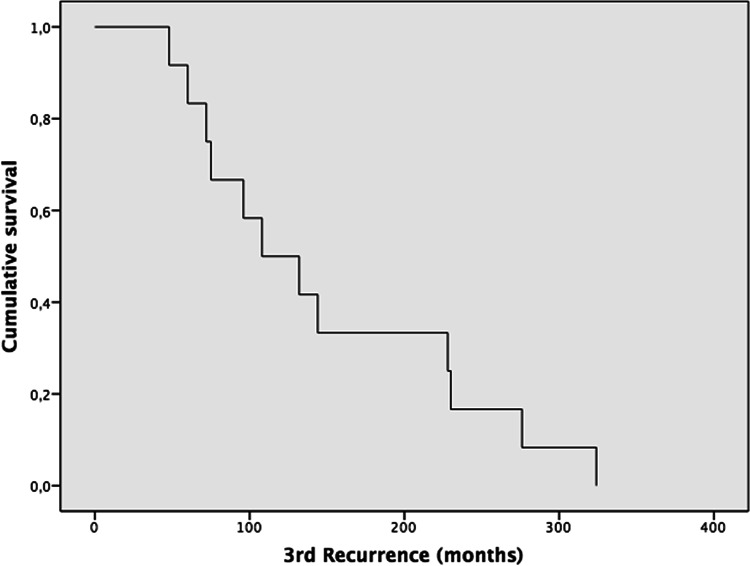 Figure 6
Figure 6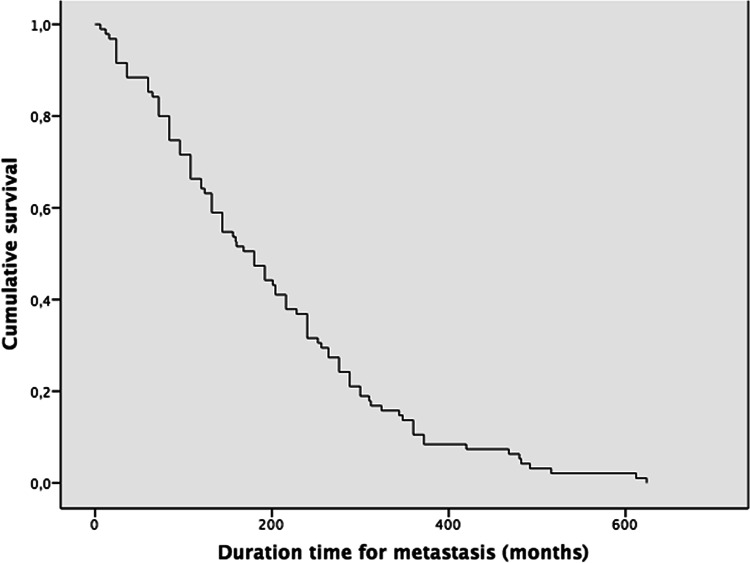 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Ear and Head Tumors · Cancer and Skin Lesions
Introduction
Pleomorphic adenomas (PAs) are the most common salivary gland neoplasm, accounting for approximately 60–80% of all salivary gland tumors [1, 2]. The parotid gland is the most frequently affected site, with approximately 85% of cases, followed by the minor salivary glands (10% of cases) and the submandibular glands (5% of cases) [3].
PAs of the parotid gland predominantly arise in the superficial lobe (about 80%), with 15–20% originating in the deep lobe and potentially extending into the parapharyngeal space, typically without symptoms or facial nerve involvement [4–6]. Standard management involves superficial or total parotidectomy with facial nerve preservation [7]. Recurrence rates are influenced by the surgical approach, with enucleation (88.9%) and simple excision (46.9%) carrying significantly higher risks compared to superficial (approximately 4%) and total parotidectomy (approximately 1%) [8, 9]. Recurrent PAs may present as multinodular lesions at or near the original site, with a 7% risk of further recurrence following reintervention [10]. Malignant transformation, though rare, occurs in 3% and may be signaled by rapid tumor growth or new-onset facial nerve dysfunction [11].
Foote and Frazell first described metastatic PA (MPA) in 1953 [12]. The WHO 5th edition classification recognizes Metastasizing Pleomorphic Adenoma (MPA), similar to the previous edition, as a rare salivary gland tumor, typically associated with multiple prior recurrences. Common metastatic sites include bone, lung, and cervical lymph nodes [13]. Despite its metastatic potential, no definitive histological or molecular markers currently predict such behavior [13, 14].
A highly speculative theory is that MPA may arise as a consequence of prior surgical interventions, potentially facilitating tumor cell entry into lymphatic or vascular channels and leading to regional or distant metastases, often years after the initial procedure [15, 16]. Hematogenous dissemination is the prevailing hypothesis, supported by the frequent occurrence of metastases in the lungs and bones. Alternative mechanisms, such as aspiration of shed tumor cells and lymphatic spread along the cervical nodal chain, have also been proposed, though less substantiated [17, 18].
MPA occurs between 1.5 and 55 years following initial surgical intervention of a PA [20]. The treatment of choice is surgical and has been shown to improve survival compared to nonoperative management [21]. According to WHO data, approximately 40% of patients succumb to the disease, with a five-year mortality rate approaching 50%. In contrast, 47% of patients achieve disease-free survival, while 13% continue to live with active disease [20].
This systematic review aims to provide a comprehensive update on the epidemiology, clinical, and molecular characteristics of MPA, with a focus on gender- and age-related differences in metastatic patterns and survival rates.
Materials and Methods
A systematic review of the published literature on cases of MPA was performed. According to the guidelines, this study met the criteria for nonhuman subject research. As a result, institutional review board approval was not required.
Search Strategy
The research followed the PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-analyses) [22]. An electronic search was conducted from 1953 until December 2024 (Fig. 1) from PUBMED, EMBASE, SCOPUS, and SCIENCE-DIRECT. The MeSH terms were “Metastatic pleomorphic adenoma” OR “Metastatic salivary benign mixed tumor” OR “Metastasizing pleomorphic adenoma” AND “Salivary gland metastasis.” A manual search was also made from referenced papers. A protocol was enrolled and recorded with the International Prospective Register of Systematic Reviews PROSPERO (CRD420251001423). The research question was based on the “PVO” framework for systematic reviews (P = patient/population, V = variable, O = outcome). This research aimed to answer the following question: What are the demographics, clinical features, and factors associated with metastasis of PA?Fig. 1. Flow chart of the selected papers
The certainty of the evidence from the primary studies will be assessed using pre-established strategies, such as evaluating methodological quality with the Oxford Centre for Evidence-based Medicine classification system and excluding studies deemed irrelevant by the reviewers. The findings will be presented in tables containing the most pertinent information.
Selection Criteria and Risk of Bias
Studies with individual data for the diagnosis of primary pleomorphic adenoma and demographics of patients with MPA were included without age, gender, or anatomic location limitations. Exclusion criteria included non-English-language, animal, and cadaveric specimens, non-obtainable full-text studies, review studies, systematic reviews, and studies with insufficient or incomplete data. Two investigators (A.P.L. and A.C) independently reviewed the search to determine that all appropriate articles were included in the analysis. Any disagreements were resolved through discussion with a third author (JB). The type of studies included were case reports [14,17,18,26–30,34,35,39–42,44–48,50–59,63–68,70–72,80–84,86–95,97–99,102–109–113] and case series [12, 38, 43, 48, 69]. For conceptual purposes of this review, the types of surgery were defined as excision (as the surgical removal of only the tumor from the salivary gland, preserving as much of the surrounding parotid gland tissue as possible) [10]. Superficial parotidectomy (defined as the surgical removal of a portion of the gland, including the tumor that also involves the removal of some surrounding tissue to clear margins) [11], and total parotidectomy (which consisted of the complete surgical removal of the parotid gland, including both the superficial and deep lobes) [10, 11].
The strength of evidence for each of the included articles was assessed by the Oxford University Centre for Evidence-based Medicine (http:// www. cebm. net/ index. aspx?o = 1025). (Table 1) These guidelines rank the studies from level 1 (highest) to 5 (lowest): level 1 (randomized controlled trials), level 2 (prospective cohort clinical studies), level 3 (3A well-conducted case–control study with low risk of bias and a high probability of a causal relationship, and 3B a case–control or case report study with significant bias or confounding factors. Level 4 (case series studies) and level 5 (case-based reasoning and bench studies). To address missing data, this study employs the pairwise deletion method, analyzing only the available data points between each pair of variables [23]. For the selected cases, the published histologic data were reviewed by a Head and Neck Pathologist at the University of Texas Southwestern Medical Center in Dallas, Texas (AC), with evaluation of the primary pleomorphic adenoma, recurrences, and metastatic pleomorphic adenoma (MPA) when available. The qualitative analysis was supplemented with descriptive statistics derived from the raw data, maintaining the original measurement units. Data normality was evaluated using the Kolmogorov–Smirnov test. For variables following a normal distribution, results were presented as mean ± standard deviation; for non-normally distributed variables, the median and interquartile range (IQR) were reported. Precision was assessed using 95% Wald confidence intervals for normally distributed quantitative variables, and the Agresti–Coull method for proportions. Time-to-event outcomes, including recurrence and metastasis, were analyzed using Kaplan–Meier (KM) estimates for endpoints with consistently reported follow-up durations (i.e., time to first, second, and third recurrence and time to metastasis). All statistical analyses were conducted using Microsoft Excel 2018 (Microsoft Corp., Redmond, WA, USA) and the Statistical Package for the Social Sciences (SPSS) software, version 20.0 Copyright IBM (SPSS Inc., Chicago, IL, USA).Table 1. Oxford classification. disease-related death (r)Author/yearStudyGenderPrimary glandAge for PAAge for MPAOrgan with metastasisFollow-up/monthsPatient statusEvidence levelFoote F /1953Case seriesfemaleright Parotid2639Lungnot mentionednot mentioned4Fine G / 1961Case reportmaleright parotid4852Vertebrae, humerus, ribs12died3bClapp WA / 1966Case reportmaleright parotid4049Thigh and muscle, shoulder, abdomen7died3bYoungs YR/1973Case reportfemaleright Parotid1627Liver12alive4Giltman L / 1977Case reportmaleright Parotid2358scalp1alive3bChen KT / 1978Case reportfemaleright Parotid3951sacrum24alive3bMa, Wajed / 1978Case reportfemaleright submandibular3856vertebraenot mentionednot mentioned4Morrison PD / 1984Case reportmaleright Parotid1869temporal bone1not mentioned4Drinkard DW / 1986Case reportmaleleft parotid1633mandible12alive3bWermuth DJ / 1988Case reportmaleright soft palate2737Lung1alive3bel-Naggar A / 1988Case reportfemaleleft parotid5463Abdomen12not mentioned3bCollina G / 1989Case reportfemaleright submandibular2635Cervical lymph nodes12alive3bmaleright Parotid814Cervical lymph nodes36aliveCresson DH / 1990Case reportfemaleright Parotid7784Retroperitoneum60alive3aSim DW / 1990Case reportmaleright Parotid1655Lung2alive3bFreeman SB / 1990Case reportfemaleleft nasal septum1532Cervical lymph nodes12alive3bLandolt U / 1990Case reportmaleright soft palate7375Lungnot mentionednot mentioned4Girson M / 1991Case reportmaleleft parotid1733Calvarianot mentionednot mentioned4Pitman MB / 1991Case reportfemaleright Parotid7072Lung, sacrum,not mentionednot mentioned4maleright Parotid2363Lung, vertebraenot mentionednot mentionedWenig BM /1992Case seriesfemaleright Parotid5177Kidney, skin0died3bmaleleft submandibular4161Sacrum, thorax, humerus36died (r)femaleleft parotid1253Skin, femur, central nervous system24died (r)femaleleft parotid7283Retroperitoneum60alivefemaleright Parotid2433Lung60alivemaleright parotid1530Cervical lymph nodes0alivefemaleleft nasal septum1331Cervical lymph nodes36alivemaleleft submandibular1420Cervical lymph nodes192alivemaleleft parotid5276Lung0diedmaleleft parotid1733Calvaria24alivefemaleright Parotid3465Kidney0aliveQureshi AA / 1994Case reportmaleleft parotid1634Supraspinatus muscle, shoulder12alive3bOlsha O / 1995Case reportmaleleft parotid2646Liver48alive3bSchreibstein JM / 1995Case reportfemaleright parotid5075Sacrum1alive4Klijanienko J / 1997Case reportfemalehard palate5663Lung, cervical lymph nodes16died (r)3bmaleparotid5355vertebrae, skull base12died (r)Hoorweg JJ / 1998Case seriesfemaleleft parotid4573Lung36alive3amaleleft parotid3041Scalp108alivefemaleright submandibular3546Sacrum, mandible18aliveSampson BA / 1998Case reportmaleright parotid7274Lung, sacrum, sphenoid6died (r)3bGoodisson DW / 1999Case reportfemaleleft hard palate1320Maxillary bone24alive3bCzader M / 2000Case reportfemaleright parotid5356Lung, kidney, skull base6alive3bChen IH / 2000Case reportfemaleleft parotid2251Cervical lymph nodes10alive3bHay MA / 2001Case reportfemaleleft parotid3651Cervical lymph nodes,26alive3bRaja V / 2002Case reportmaleleft parotid6772Lungnot mentionednot mentioned4Marioni G / 2003Case reportmaleright parotid2032Sinonasal6alive3bKhademi / 2003Case reportfemaletongue left area1919Cervical lymph nodes24alive3bYoshizaki T / 2004Case reportfemaleleft parotid1033Lung21alive3bMuthusami J.C. / 2006Case reportmaleright Parotid2331Scalp24alive3bSteele NP / 2007Case reportfemaleright Parotid1543Lung1not mentioned4Sabesan T/ 2007Case reportmaleleft parotid3360Supraclavicular fossa24alive3bHyun Yee H / 2007Case reportfemaleleft submandibular2868Lung, skin, brain11not mentioned4Van der Schroeff MP / 2007Case reportfemaleright parotid1962Ribs6died3bSit KY / 2008Case reportmaleleft submandibular3846Lung6alive3bRodriguez FJ / 2008Case reportfemaleleft parotid5457Lung60died (r)3bGhosh A / 2008Case reportfemaleleft parotid2935Shoulder,not mentionednot mentioned4Xiao L / 2008Case reportfemaleleft parotid4672Sacrum, kidney34died (r)3bEbbing J / 2009Case reportfemaleleft parotid2049Kidneynot mentionednot mentioned4Zhang Y / 2009Case reportfemaleleft parotid4564Lung1alive3bLarbcharoensub / 2009Case seriesfemaleright submandibular3645Cervical lymph nodes6alive3afemaleleft parotid3242Cervical lymph nodes30alivefemaleright parotid2740Cervical lymph nodes1aliveBhutta MF / 2010Case reportfemaleleft parotid6275Kidney9alive3bBae CH / 2010Case reportmalesoft palate4849Sphenoid sinusnot mentionednot mentioned4Singhal A / 2010case reportmaleleft parotid1646livernot mentionednot mentioned4Chen CP / 2011Case reportmaleright buccal mucosa7375Lung, cervical lymph nodes44not mentioned4Reiland MD / 2012Case reportmaleleft parotid1531Scalp, maxillary bone, infratemporal fossa, sinus132alive3aVivian MA / 2012Case reportfemaleright Parotid2440Kidneynot mentionednot mentioned4Santaliz R /2012Case reportfemaleleft submandibular2353Cervical lymph nodes10alive3bRF Chinoy / 2013case reportmaleparotid5050Cervical lymph nodesnot mentionednot mentioned4Akiba J / 2013case reportfemaleleft hard palate4262Maxillary bonenot mentionednot mentioned4Miladi S / 2014Case reportfemaleleft submandibular1838Cervical lymph nodes8alive3bTarsitano A / 2014Case reportfemaleleft parotid911Sinonasal6alive3bAbou-Foul AK / 2014Case reportmaleleft parotid5057Lung, liver16alive3bMcGarry JG / 2015Case reportfemaleright Parotid4065Shoulder,3died (r)3bM Moonim / 2015Case reportfemaleright Parotid1668Liver, thyroid6alive3bMariano FV / 2015Case reportfemaleleft parotid6568Scalpnot mentionednot mentioned4Young VS / 2015Case reportfemaleparotid4565Liver3not mentioned4Knight J / 2017Case reportmaleright submandibular6268Vertebrae7not mentioned4Nakai A /2017Case reportfemaleright Parotid2838Lung3not mentioned4Koyama M/ 2018Case reportfemaleleft parotid4061Lung, kidney, skull base60alive3bKoyama M / 2018Case reportfemaleleft parotid4063Lung, liver, kidney, sinonasal, brain60alive3bWasserman JK / 2019Case seriesfemaleparotid3557Thigh and musclenot mentionednot mentioned4maleparotid3657Cervical lymph nodesnot mentionednot mentionedmaleparotid4348vertebraenot mentionednot mentionedmaleparotid3459Cervical lymph nodesnot mentionednot mentionedWong DKC / 2019case reportfemaleright Parotid3161Cervical lymph nodes, infratemporal fossa6alive3bShoukair FL / 2020case reportfemaleright submandibular1337cervical lymph nodes, lips24alive3bFonseca D / 2022Case reportfemaleright parotid1429Cervical lymph nodes1not mentioned4Lu H / 2023Case reportmaleleft submandibular2834Cervical lymph node6alive3bLobo J / 2023Case reportfemaleparotid1243Kidney24alive4Catarsi L /2023Case reportfemaleleft parotid2331Cervical lymph nodesnot mentionednot mentioned4AlNahwe RW / 2023Case reportmaleright Parotid2539Scalp24not mentioned4Tsai /2024case reportfemaleleft parotid6161Cervical lymph nodes126not mentioned4Jacob S / 2024case reportmaleleft parotid1219cervical lymph nodenot mentionednot mentioned4
Results
Some of the highlights are presented here. The complete results and data of the 95 cases are summarized in Tables 2, 3 (Demographics), and Tables 4, 5, 6, 7 (Kaplan–Meier).Table 2. Demographics of metastatic pleomorphic adenoma. *[IC 95%] two-sided confidence intervals calculated using the Agresti–Coull method; total n = 95 cases. Mean ± standard deviation is reported for normally distributed variables (Kolmogorov–Smirnov test p > 0.05)Total100% (N = 95) Total casesAge (years)Age at PA DiagnosisAge at the time ofMetastasisMean ± SD (Min/Max)[CI95%]33.7 ± 17.9 (8/77)49.9 ± 17.1 (11/84)[30.1–37.3][46.5–53.3]Size of MPA lesion (cm)11.8 ± 17.9 (1/145)[8.2–15.4]100% (n = 5)[CI95%]SexFemale58.8% (n = 56)[50.0–69.6]Male41.1% (n = 39)[30.4–50.0]Type of gland primaryParotid75.8% (n = 72)[66.4–83.2] *Submandibular13.6% (n = 13)[8.2–22.2] *Bucogingival1.0% (n = 1)[0.2–5.6] *Soft palate3.2% (n = 3)[1.1–8.7] *Nasal septum2.2% (n = 2)[0.6–5.6] *Hard palate3.2% (n = 3)[1.1–8.7] Tongue1.0% (n = 1)[0.2–5.6] Anatomic locationRight43.2% (n = 41)[33.4–53.2]Left46.4% (n = 44)[36.5–56.3]Not mentioned10.6% (n = 10)–Type of surgeryExcision42.1% (n = 40)[33.4–53.2]Superficial parotidectomy28.4% (n = 27)[19.6–29.2]Total parotidectomy (resection)17.9% (n = 17)[13.2–23.1]Enucleation8.4% (n = 8)[2.8–13.7]Fragmented excision1.0% (n = 1)[0.0–6.2] Not mentioned2.1% (n = 2)–Mean ± SD (n)**[CI95%]Recurrence—First (months)87.1 ± 92.1 (n = 62)[64.4–109.8]Recurrence—second (months)100.3 ± 69.5(n = 29)[75.0–125.6]Recurrence—third (months)149.4 ± 92.3(n = 12)[97.2–201.6]Recurrence—fourth (months)105.6 ± 31.04(n = 6)[80.8–130.4]Recurrence—fifth (months)142.5 ± 12.3(n = 4)[130.4–154.5]Duration time for metastasis (months)198.3 ± 138.3(n = 95)[170.5–226.1]Follow-up (months)26.9 ± 33.7(n = 69)[19.0–34.9]100% (n = 95)[CI95%]Patient statusAlive52.7% `(n = 50)[41.6–61.5]Dead from the disease8.4% (n = 8)[6.6–20.2]Dead from another condition5.3% (n = 5)[1.9–12.03]Not mentioned34% (n = 32)–Table 3. Organs affected by metastatic pleomorphic adenoma. [IC 95%] two-sided confidence intervals calculated using the Agresti–Coull method; total (n = 128) lesions from 95 cases128 = 100% (N = 95)[CI95%]Bone (All sites)21.88% (n = 28)[15.5–29.8]Sacrum/ iliac bone5.47% (n = 7)[2.5–11.1]Vertebrae4.69% (n = 6)[2.0–10.1]Maxillary bone (and palate)2.34% (n = 3)[0.5–7.0]Infratemporal fossa or temporal bone2.34% (n = 3)[0.5–7.0]Skull base1.56% (n = 2)[0.1–5.9]Mandible1.56% (n = 2)[0.1–5.9]Humerus1.56% (n = 2)[0.1–5.9]Ribs1.56% (n = 2)[0.1–5.9]Femur0.78% (n = 1)[0.0–4.7]Cervical lymph nodes20.31% (n = 26)[14.2–28.2]Lung17.97% (n = 23)[12.2–25.6]Kidney7.81% (n = 10)[4.1–13.9]Liver5.47% (n = 7)[2.5–11.1]Scalp4.69% (n = 6)[2.0–10.1]Sinonasal3.12% (n = 4)[1.0–8.0]Supraspinatus muscle, scapula, or shoulder3.12% (n = 4)[1.0–8.0]Skin2.34% (n = 3)[0.5–7.0]Brain1.56% (n = 2)[0.1–5.9]Sphenoid sinus1.56% (n = 2)[0.1–5.9]Upper and lower lip0.78% (n = 1)[0.0–4.7]Thyroid0.78% (n = 1)[0.0–4.7]Supraclavicular fossa0.78% (n = 1)[0.0–4.7]Abdomen1.56% (n = 2)[0.1–5.9]Retroperitoneum1.56% (n = 2)[0.1–5.9]Thigh and muscle1.56% (n = 2)[0.1–5.9]Central nervous system0.78% (n = 1)[0.0–4.7]Table 4A Kaplan–Meier (KM) curve was constructed to assess time to first recurrence following initial PA, with follow-up extending to nearly 500 monthsRecurrence-First (months) Median recurrence 72 Mean 87.1 ± SD 92.1 (n=62) IC95% [64.4–109.8]Table 5. The second recurrence–free survival function was estimated with KM, with a maximum follow-up period of approximately 240 to 250 monthsRecurrence–2nd (months) Median recurrence 72 Mean 100.3±69.5 (n=29) IC95% [75.0–125.6]Table 6. Third recurrence-free survival. The KM curve demonstrates a stepwise decline without a plateau, with a concentration of events occurring between 50 and 140 monthsRecurrence–3rd (months) Median recurrence 108 Mean 149.4±92.3 (n=12) IC95% [97.2–201.6]Table 7KM curve for time to metastasis reveals a sustained decline in metastasis-free survival (MFS), without reaching a plateau throughout the follow-up periodMetastasis–time to event (months) Median recurrence 180 Mean 198.3 ± 138.3 (n=95) IC95% [170.5–226.1]
Age of PA diagnosis: The patients’ ages ranged from 9 to 77 years. The average age of diagnosis for both genders was 33.7 ± 17.9. For females, the average age was 32.98 years, with the youngest female patient diagnosed at 9 years [34]. For males, the average was 33.79 years, with the youngest diagnosed at 8 years [35].
Type of surgery and recurrence: The most common treatment for PAs was excision in 42.1% (n = 40) cases. The next most common treatment was superficial parotidectomy with 28.4% (n = 28) cases. Seventeen (n = 17), 17.9% of patients received a total parotidectomy/resection. Recurrences: Several patients experienced recurrence of their PA (up to five recurrences) before developing metastasis. The mean time to the first recurrence was 87.1 ± 92.1 months (n = 62), while the second recurrence occurred after an average of 100.3 ± 69.5 months (n = 29). Subsequent recurrences were observed in only a small number of cases.
Age of MPA diagnosis: The average age of diagnosis for both genders was 49.9 ± 17.1; the youngest female patient was diagnosed at 11 years [34]. The youngest male patient was 20 years old [43].
Time to metastasis: The average time for MPA was 198.3 ± 138.3 months (n = 93), ranging from 0 to 624 months. In two cases, the MPA was diagnosed synchronously as the pleomorphic adenoma.
Patient status: From the follow-up data analyzed, 52.7% (n = 50) were alive with the disease, 8.4%(n = 8) had died from the MPA, and 5.3% (n = 5) had died for other reasons. Follow-up information was not available in 34% (n = 32) of cases.
Organ/site involved in MPA: To ensure a more accurate representation of metastatic distribution, the analysis included all affected organs rather than calculating metastasis rates solely on a per-patient basis. This method accounted for cases with multiple simultaneous metastatic sites and helped prevent inflation of metastasis percentages. Among the 95 cases reviewed, a total of 128 metastatic sites were documented. The most frequently affected organs were the bone and lymph nodes, at 21.88% (n = 28) cases and 20.31% (n = 26) of cases, respectively. Within the bone category, the sacrum (5.47%) and vertebrae (4.69%) were the most commonly involved sites, followed by the lungs, in 17.97% (n = 23) of cases. Interestingly, the kidney was involved in 7.81% (n = 10) of cases. The complete results and data of the organ/site affected by metastasizing pleomorphic adenoma of the salivary gland are summarized in Table 3.
Discussion
Our systematic review included 76 studies, encompassing a total of 95 cases with a diagnosis of metastatic pleomorphic adenoma (MPA). Malignant transformation is a recognized negative outcome of pleomorphic adenomas (PAs), occurring in approximately 1.5% of cases within the first five years and rising to 9.5% after 15 years or more [24]. Among the resulting malignancies, salivary duct carcinoma is the most frequently reported subtype, accounting for 41% of cases [25]. In contrast, metastatic pleomorphic adenoma (MPA) represents an even rarer phenomenon of malignant transformation, with a capacity for regional or distant spread. Notably, MPA retains the histological features of a benign tumor, lacking cytological signs of malignancy such as cellular atypia, elevated mitotic activity, or necrosis. Diagnosis of MPA is therefore based solely on the presence of metastasis, despite the absence of malignant histopathological characteristics [13, 20].
Tumor Recurrence
In our review, local recurrence for PAs occurred in 65% of cases, and multiple recurrences (from 1 to 5 recurrences) in 35% before the development of the MPA. The average time to the first recurrence was 87.1 months, and the average time to the second recurrence was 100.3 months (Table 2). Something unexpected was the recurrence after total parotidectomy, with 12.3%, where the average is 3% for primary PA [114]. The local and multiple recurrence rates in our study were similar to the review by Knight et al., who reported local recurrence in 72.8% and multiple recurrence in 37% of their cases [19]. The literature also documents a latency period between primary PA to MPA of 6 months [26] to over 52 years [27]. Our review showed that the mean age for PA was 33.7 years, with a range from 8 [35] to 77 [39]. For MPA, the mean age was 49.9 years, with a range from 11 [34] to 84 years [39]. Of note, there were 2 cases where the metastatic PA was diagnosed at the same time as the primary PA that had no previous surgical intervention [28, 29] (Table 4, 5, 6).
Molecular Data
Although limited, several studies have reported significant findings related to the potential molecular mechanisms involved in metastasis. Notably, a study by Mariano et al. identified deletions in chromosomes 3p in PA and 9p in cases of MPA [30]. Chromosome 3p deletions have been implicated in various malignant epithelial neoplasms, including clear cell renal cell carcinoma, where deletions of 3p and 9p were observed in 25% and 47% of metastatic cases, respectively [31]. Furthermore, deletions in 9p have demonstrated a statistically significant association with both lymph node involvement and distant metastasis (P = 0.03) [32].
Yu et al. identified the CD105 molecule in recurrent and metastasizing pleomorphic adenomas [36]. This molecule, also known as endoglin, is a transmembrane glycoprotein primarily expressed on endothelial cells, and it plays a significant role in metastasis. Elevated levels of CD105 have been detected in various cancers and are positively correlated with tumor progression and metastasis [37]. Two studies reported PLAG1 mutations in cases of MPA [38, 95]. In a study by Agaimy et al., six tumors were classified as conventional PAs, while four exhibited canalicular-trabecular morphology. Among these, three MPAs demonstrated HMGA2 gene fusions, four showed PLAG1 alterations, and one case harbored an NFIB mutation [96]. Akiba et al. found an MPA with PLAG1 expression with no gene rearrangements by (RT)-PCR. RT-PCR did not demonstrate any fusion genes, including PLAG1-CTNNB1, PLAG1-CHCHD7, PLAG1-LHIT, and PLAG1-TCEA1, although the internal control, Porphobilinogen Deaminase (PBGD), was identified in both primary and metastatic lesions [90].
Wasserman et al. identified a novel HMGA2::-TMTC2 fusion in an MPA, representing a unique genetic alteration. This fusion was confirmed through RNA sequencing and fluorescence in situ hybridization (FISH) [38]. TMTC2 (Transmembrane O-Mannosyltransferase Targeting Cadherins 2) is located on chromosome 12q21.31. It is a protein that modifies cadherins, which are cell adhesion molecules [33]. These data support growing evidence that specific genetic alterations may contribute to the metastatic potential of PAs. The molecular events that underpin MPA merit additional investigation, as a greater understanding may have impacts on diagnosis and treatment.
Mechanism of Spread
The route by which pleomorphic adenoma metastasizes remains poorly understood. A strong consideration (still hypothetical and speculative) has been given to hematogenous dissemination during the incisional biopsy or surgical manipulation (seeding) [16, 17]. Including fine needle aspiration [60]. The tumor may then form tumor embolisms in capsular blood vessels before hematogenous spread to different anatomical sites [61] (Fig. 2). Knight et al. reported that the most frequently affected sites in MPA were bone (36.6%), followed by the lungs (33.8%) and cervical lymph nodes. However, taking bone as an example, we found that most MPAs affect the axial skeleton, including the skull, vertebrae, ribs, sternum, sacrum, and mandible. MPA can be localized, affecting a specific bone [19, 56, 81, 86, 89–91, 93, 94], or multifocal, affecting multiple discrete bones [43, 47, 57, 80–84, 92]. In our study, MPA metastasized to bone in 21.88% of cases, being the sacrum 5.47% [38, 43, 57, 86–88] and the vertebrae in 4.69% [19, 38, 47, 56, 82, 89], the most common, followed by 11.72% in other bones. In the context of bone metastasis, pleomorphic adenoma-derived myoepithelial cells have been shown to secrete key bone-modulating factors, including Receptor Activator of Nuclear Factor Kappa-Β Ligand (RANKL) [76], Parathyroid Hormone-related Protein (PTHrP) [78], and Matrix Metalloproteinases (MMPs), particularly MMP-2 and MMP-9 [77]. RANKL and PTHrP play critical roles in bone metabolism and are frequently associated with underlying tumor-induced bone metastases. In pleomorphic adenomas, PTHrP expression has been observed in the inner lining of tubuloductal and cyst-like structures, single-layered ducts, isolated tumor cells, and clusters demonstrating squamous metaplasia [79].Fig. 2H&E 10x. Metastatic pleomorphic adenoma to the liver (courtesy of Columbia University Department of Pathology). Clear separation of hepatocytes and myoepithelial cells with chondroid and myxoid background
For lymphatic spread, the second most common after bone, our study found 20.31% of cases [17, 26, 28, 29, 35, 38, 41, 43, 47, 52, 63–72]. A possible theory is that tumor cells may enter the lymphatic system during surgical procedures and subsequently reach distant sites such as the lungs. However, careful diagnostic evaluation is essential to avoid misclassifying a recurrent pleomorphic adenoma (PA) as an MPA, as some PAs may be mistakenly interpreted as lymph node metastases. True lymphatic metastasis is typically supported by cases occurring several years after the initial or repeated surgical interventions. Drainage to the deep cervical lymph nodes eventually enters the thoracic duct (main lymphatic channel). The thoracic duct empties into the left subclavian vein. Cells then follow the same systemic circulation [74].
The lungs were the third most common organ affected by MPA, in 17.97% of cases. This is interesting as the lung represents the first capillary bed encountered by venous blood draining from the head and neck, particularly via the facial and jugular veins. They also serve as a primary site for filtration and entrapment of circulating tumor cells within the pulmonary vasculature [62]. A key process for different metastasis is the Batson’s Venous Plexus (Vertebral Venous Plexus), which is a valveless venous network connecting pelvic, thoracic, and cranial veins to the vertebral column, including the sacrum. As the plexus is valveless, blood flow (and tumor cells) can reverse in direction during straining, coughing, or increased intra-abdominal pressure [75] (Fig. 3). On the other hand, Wermuth et al. have suggested that the oral cavity may serve as a potential source of pulmonary metastasis through the aspiration of tumor cells [40]. Even though 23 lung metastases were documented [12, 40–46, 48–59], four of 5 intraorally PA cases metastasized to the lung [40, 41, 47, 55], which may support this hypothesis.Fig. 3. Routes of possible metastasis of MPA. The MPA could invade veins from the parotid region, which drain into the external and internal jugular veins, to the subclavian vein and the superior vena cava (SVC). Blood subsequently travels to the right side of the heart, specifically the right atrium and ventricle, where the tumor cells may survive in the lung’s capillary bed and enter the left side of the heart. through the lungs [74]. From there, it’s pumped into the aorta and distributed throughout the body via arteries. and out to the rest of the body. The Batson plexus plays a fundamental role. For example, the liver has a dual supply, with 25% of the blood from the hepatic artery (a branch of the aorta via the celiac trunk). Thus, the tumor cells can reach the liver through the hepatic artery and lodge in the liver’s capillary beds (sinusoids) [73]
While it is not possible at this time to predict which PA will metastasize, factors that may play a role in metastasis include multiple recurrences of PA, incomplete surgical excision (e.g., enucleation versus excision or parotidectomy), Long-standing tumors, and a history of capsular rupture during surgery.
Prognosis
Although the overall mortality was 13.4% (n = cases), MPA-related deaths were 8 cases; some of the deaths occurred at 3 months [80] and 8 years after diagnosis of MPA [47]. Among those with comprehensive information, MPAs presenting with multiple metastases involving bone were associated with an 85% increased risk of death, with an average survival time of 13.3 months [43, 47, 57, 80–84]. This survival duration is comparable to the average of 9.8 months observed in head and neck metastases originating from other primary sites [85] (Table 7).
Of note, adjuvant radiotherapy was employed in several recurrent PAs and MPAs in our review [12, 18, 38, 44, 46–48, 50, 52, 53, 56–58, 63, 65, 69, 80, 81, 86, 98, 99, 101, 105, 108, 111]. However, it is challenging to determine whether radiation therapy improved survival or prognosis, as noted in a previous study [19].
Pleomorphic adenomas exhibit unpredictable latency and potential for regional or distant spread, necessitating long-term patient monitoring—especially in cases of incomplete excision or recurrence. Complete surgical removal with clear margins remains critical to reducing metastatic risk. Emerging perspectives suggest that PAs may possess low-grade malignant potential in specific contexts. To better understand MPA, future research should focus on molecular characterization through genomic and transcriptomic analyses. Establishing centralized registries or multi-institutional databases for rare salivary gland tumors could enhance data collection, supporting improved diagnostic and therapeutic strategies.
Study Limitations
The primary limitation of this review lies in the variability of the available literature, as the majority of included cases were isolated reports or small case series, many of which lack standardized diagnostic criteria or uniform follow-up (Table 8). Furthermore, the infrequency of MPA likely contributes to underrecognition and diagnostic misclassification, potentially skewing incidence and clinical outcomes estimates. Nevertheless, by compiling findings across diverse sources, this review offers a broader perspective on the clinical presentation and pathological features of MPAs.Table 8. Evaluation of the histologic features of different analyzed studies to evaluate the supporting images of the diagnosis and the included information for confirmationAuthorYearPA DiagnosisDiagnosis of recurrenceDiagnosis of MPA with PA histologyCommentsFoote, F. W1953correctHistology of recurrencePA not showing the background organblack and white imageMarshall G1961Histology of primary parotidHistology of local recurrenceMost likely recurrenceBlack and white pictureChen KT1978Primary compatible with PANo histologyPA without the background of the organEl naggar1988Histology of primary parotidHistology of local recurrencePA not showing the background organBlack and white pictureWermuth DJ1988Histology of primaryNo histologyPA not showing the background organGuido Collina1989Histology of submandibular PANo histologyMost likely met within the lymph nodeBlack and whiteDavid Sim1990Histology of primary parotidHistology of recurrencePA in the lungBlack and white pictureCresson1990Histology of primary parotidNo histologyMPA does not show the background organBlack and white pictureWenig BM1992Primary Hx, concerning for malignancyNo histologyConcerning for an EX PA-carcinomaBlack and white pictures, 5 cases shownJerzy Klijanienko1997Histology of primary parotidHistology of recurrencePA without background of the met- questionable met VS recurrencepictures not optimalJJ Hoorweg1997Histology of primary parotidHistology of local recurrenceThe picture is difficult to seeblack and white pictureGoodison1999maxillary PAHistology of recurrenceMost compatible with recurrence- not metBlack and white pictureChen Ih2000ParotidNo good picture, difficult to evaluateOne black and white picture- not convincingMarioni G2003Histology of primary parotidMultiple cases includedPA not showing the background organCD105 positiveYoshizaki T2004Histology of primary parotidHistology of local recurrencePA not showing the background organBlack and white pictureMuthusami J.C2006Histology of primary parotidHistology of local recurrenceSubcutaneous scalp PASteele NP2007Histology of primary parotidHistology of local recurrenceMPA is not showing the background organT Sabesan2007Histology of primary parotidNo histology of recurrenceMPA in a supraclavicular lymph nodeVan der Schroeff2007Histology of primary parotidHistology of local recurrenceMPA not showing the background organBlack and white pictureHyun Yee H2007Histology of submandibular PAHistology of chondromyxoid syringomaMPa in boneXiao L2008No informationHypercellular area of the PA concerningno primarySit KY2008Histology of PANo imageno imageRodríguez-Fernández J2008Histology of primary parotidPA without the background of the metblack and white pictureEbbing J2009Histology of primary parotidNo histologyMPA in the kidneyZhang Y2009Histology of primary parotidHistology of recurrent multipleOnly cytology pictures—no backgroundonly cytology picturesBhutta MF2010Histology of primary parotidHistology of local recurrencePicture not optimalBae Ch2010PA soft palateHistology of local recurrenceMost likely PA recurrenceReiland MD2012Histology of the upper gingiva PAHistology of tonsillar PA?MPA in the skinSantaliz-Ruiz LE2012No primary hxNo HistologyMore suggestive of recurrent PAVivian MA2012Histology of primary parotidHistology of local recurrenceDifficult to appreciate the PA- ONLY CytologyAkiba J2013Primary palate lesion with vascular invasionNo histologyMet to the maxillary bone- No bone background in the picturePLAG1 IHC + RF Chinoy2013No primary histologyNo histology of recurrenceSuspicious of Epithelial myoepithelial carcinomaTarsitano A2014Histology of primary parotidHistology of local recurrenceThe picture shows a lesion underneath the skin, but the image is smallAbou-Foul AK2014Histology of primary parotidNo histologyMPA in the lungMariano FV2015Histology of primary parotidNo histologyMPA- good subcutaneous imageYoung VS2015Histology of adenocarcinoma of the colonNo histologyPA not showing the background organMcGarry JG2015Histology of primary parotidHistology of local recurrenceSuggestive of recurrenceM Moonim2015Histology of primary parotidHistology of local recurrenceMPA in thyroidKnight J2016No histology includedNo histologyMPA does not show the background organNakai A2017Primary with a capsular irregularityNo recurrence HistologyHistology of MPA in the lungKoyama M2018Histology of primary parotidHistology of recurrent multipleMPA not showing the background organWasserman JK2019Histology of primary parotidHistology of local recurrenceMPA histology4 cases total- one with HMGA2-TMCT2 mutationWong DKC2019Histology of primary parotidNo histologyDifficult to see the imageInfratemporalShoukair FL2020Histology of the upper lip PANo histologyMost likely local recurrenceFonseca D2022Histology of primary parotidHistology of recurrent multipleProbably recurrence- difficult to check the lymph node pictureAlNahwe RW2023No histologyNo histologyNo histologyQuality clinicalW Xu2023Histology of primary parotidNo histologyRecurrence- no PA histology pictureNo histology pictureNiels Rupp2023No histology includedNo histologyMPA in the kidneyPLAG1 IHC + Tsai WH2024Histology of primary parotidHistology of recurrenceMost suggestive of recurrence
Conclusion
This systematic review synthesizes current evidence on MPA, demonstrating that, despite its benign histologic appearance, Uncontrolled recurrence is a risk factor for metastatic potential to both regional and distant sites, most notably to bone. These findings underscore the importance of long-term clinical surveillance and meticulous documentation. Furthermore, the review identifies a significant gap in consistent molecular and immunohistochemical profiling. In this regard, incorporating analyses of chromosomal deletions (particularly 9p), as well as markers such as CD105 and HMGA2::TMTC2, may enhance understanding of tumor biology and aid in risk stratification. By highlighting these, this study lays the groundwork for future multicenter investigations that integrate molecular diagnostics to improve the accuracy of diagnosis, optimize management strategies, and refine follow-up protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Classification of Tumours Editorial Board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer; 2022. (WHO classification of tumours series, 5th ed.; vol. 9). https://publications.iarc.fr/
- 233www.ncbi.nlm.nih.gov/gene/160335#:~:text=160335%20%2D%20Gene%20Result TMTC 2%20transmembrane%20O,targeting%20cadherins%202%20%5B%20(human)%5D