Stroke severity and other predictors of venous thromboembolism in stroke patients—a population-based cohort study
Ditte Vestergaard Hansen, Nick van Es, Henrik Toft Sørensen, Jonathan M. Coutinho, Nils Skajaa

TL;DR
This study identifies stroke severity, active cancer, and prior VTE as strong predictors of post-stroke venous thromboembolism, helping identify high-risk patients.
Contribution
The study provides new evidence that stroke severity is a consistent predictor of post-stroke VTE across both acute and subacute phases.
Findings
Severe stroke, active cancer, and previous VTE were strong predictors of post-stroke VTE.
The risk of VTE was 2- to 5-fold higher in patients with these risk factors.
Findings were consistent for both ischemic stroke and intracerebral hemorrhage.
Abstract
Venous thromboembolism (VTE) frequently occurs after stroke, particularly within the first 3 months after diagnosis. Poststroke VTE is associated with increased mortality. Stroke severity is a known predictor of adverse prognosis; however, its ability to predict VTE is unclear. Knowledge regarding other predictors of poststroke VTE is lacking. To identify clinical predictors of poststroke VTE in the subacute and acute phases, and to assess the association between stroke severity and poststroke VTE. In a population-based cohort study, we identified patients (aged ≥18 years and without recent VTE) with first-time ischemic stroke (N = 129,345) or intracerebral hemorrhage (N = 16,887) from 2004-2021. We computed the cumulative incidence proportion and subdistribution hazard ratio for VTE for each potential predictor in the subacute phase (3 months) and acute phase (7 days). For stroke…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
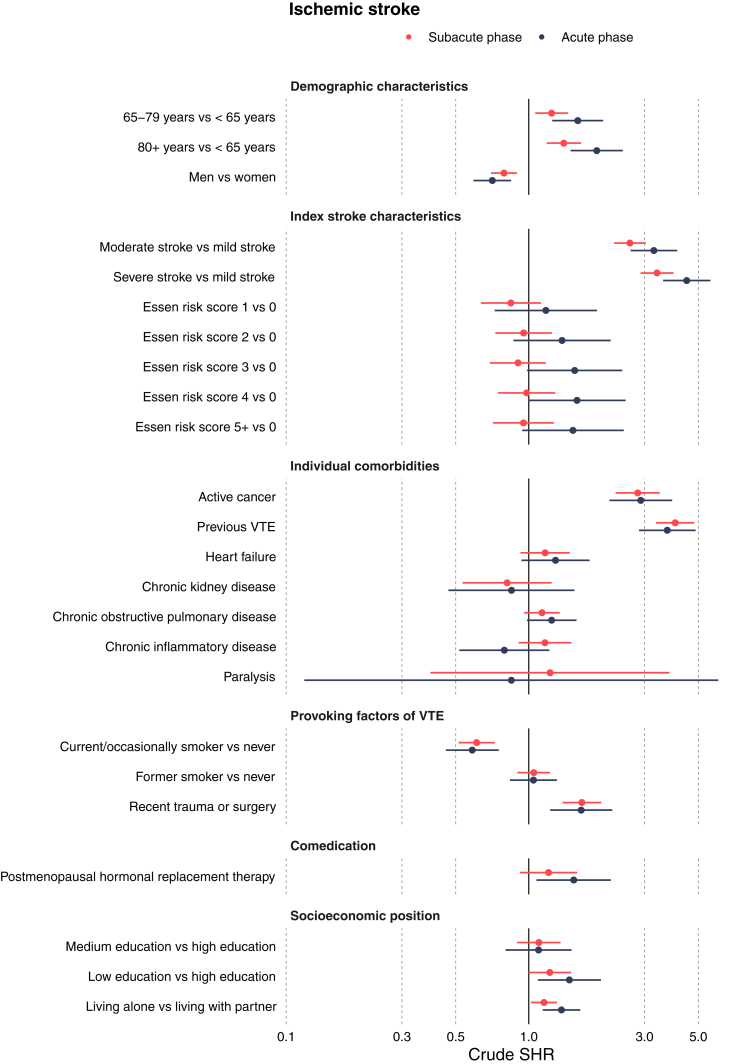 Figure 1
Figure 1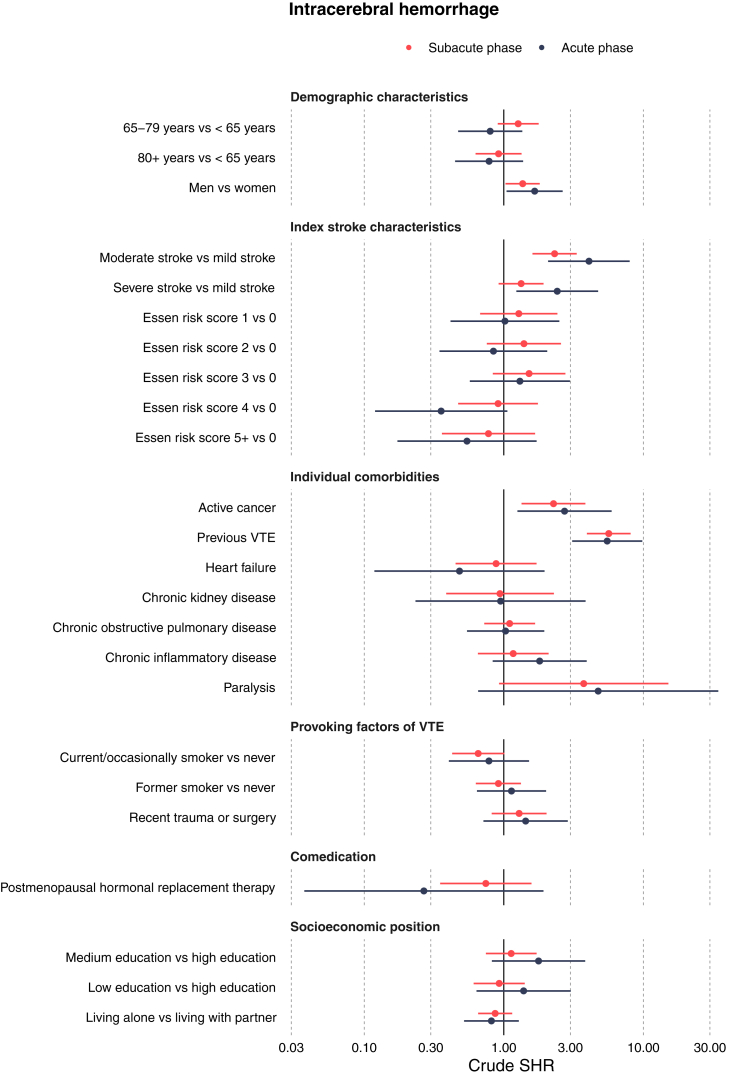 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Venous Thromboembolism Diagnosis and Management
Introduction
1
Venous thromboembolism (VTE), a composite of deep vein thrombosis and pulmonary embolism, is a known complication of stroke, particularly during hospitalization and immediately thereafter [1,2]. Compared with the general population, patients with stroke have a 4- to 5-fold greater risk of VTE in the first 3 months after diagnosis, and poststroke VTE is associated with increased mortality [3,4]. Thromboprophylaxis with low molecular weight heparin is recommended for immobilized patients, regardless of their stroke subtype, and is typically discontinued after discharge [5].
Although findings from large randomized controlled studies do not support extended thromboprophylaxis in acutely ill hospitalized patients [[6], [7], [8], [9]], a recent meta-analysis focusing on the subgroup of patients with ischemic stroke within those studies found a clinically relevant 30% decrease in VTE with extension of thromboprophylaxis as long as 4 weeks after discharge [10]. Thus, identifying patients with stroke at higher risk of VTE after stroke may improve the risk-benefit ratio. However, little information on the clinical predictors of VTE in patients with stroke is currently available, and high-quality studies are lacking [4,[11], [12], [13], [14], [15], [16], [17]]. More than half of the existing studies had relatively small sample sizes (N < 600), and several studies did not report important information, such as the number of initial eligible participants or reasons for exclusion [11,[14], [15], [16], [17]]. Importantly, previous studies on stroke severity and VTE have either been inconsistent or have not investigated specific stroke subtypes, such as intracerebral hemorrhage [11,[14], [15], [16], [17], [18]]. Therefore, whether stroke severity is an important predictor of poststroke VTE remains unclear. Stroke severity is as a well-established predictor of other poststroke outcomes, including mortality, recovery, disability, mental health conditions, and workforce participation [[19], [20], [21], [22]].
In a Danish nationwide cohort study, we aimed to identify clinical predictors of poststroke VTE during both the subacute (3 months after diagnosis) and the acute (7 days after diagnosis) phases. Additionally, we evaluated the association between stroke severity and poststroke VTE.
Methods
2
Design and setting
2.1
We performed a cohort study using routinely collected data from Danish registries with nationwide, population-based coverage. The Danish healthcare system is universal and tax-supported and provides equal and free access to primary and hospital care, including acute stroke treatment [23]. Denmark has a rich array of population-based registries, which are linked at the individual patient level through the unique personal identification number assigned to all residents at birth or immigration [23]. In this study, we used data from the Danish Stroke Registry (Stroke Registry) [24], the Danish Civil Registration System [25], the Danish National Patient Registry (Patient Registry) [26], the Danish National Prescription Registry (Prescription Registry), and the Attainment Register [27,28]. Data sources are described in detail in Supplementary Table 1. Although the registries provide comprehensive coverage, certain limits exist. Of particular concern, medications administered during hospitalization, such as thromboprophylaxis relevant to stroke patients, are not captured. This limitation should be considered when interpreting our findings.
Ethical approval is not required for registry-based studies in Denmark. This study was approved by the Danish Data Protection Agency at Aarhus University (no. 2016-051-000001-1502). We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines [29].
Stroke management in Denmark
2.2
In Denmark, patients with suspected stroke are transported to specialized stroke units across the country and treated by a multidisciplinary team of healthcare professionals [30]. Effective prehospital and in-hospital management is in place in the country; ∼24% of patients with ischemic stroke receive reperfusion therapy, thrombolysis, or thrombectomy in Denmark, whereas the corresponding proportion in the United States is only 13% [31]. Clinicians are obligated to report stroke events and related clinical patient data to the Stroke Registry, a nationwide quality database with complete data from May 1, 2004 [24]. The sensitivity and positive predictive value of the coded diagnoses for stroke in this registry have been estimated to exceed 90% [32,33].
The national guidelines of the Danish Neurological Society recommend therapeutic anticoagulation (eg, low molecular weight heparin/unfractionated heparin or direct oral anticoagulant) for secondary prevention in patients with cardioembolic ischemic stroke (eg, in the presence of atrial fibrillation) [34], which is in agreement with the American Stroke Association and European Stroke Organisation guidelines for ischemic stroke [5,35]. For patients with noncardioembolic ischemic stroke, antiplatelet treatment (eg, aspirin) is recommended immediately, if they are not eligible for reperfusion therapy (thrombolysis or thrombectomy) [34]. For patients receiving reperfusion therapy, antiplatelet treatment is recommended, but administration is generally delayed until 24 hours after reperfusion therapy [36]. For patients with intracerebral hemorrhage, the optimal thromboprophylaxis remains complex and unclear because of concerns about worsening of intracerebral bleeding [[37], [38], [39]]. National and international guidelines emphasize that determining optimal treatment is challenging for clinicians, and the decision to initiate thromboprophylaxis is often evaluated on the individual patient level [40,41].
Study cohort
2.3
We identified Danish residents aged ≥18 years hospitalized with a first-time diagnosis of ischemic stroke or intracerebral hemorrhage between May 1, 2004 and December 31, 2021, as recorded in the Stroke Registry. The admission date of the first-time stroke event was classified as the index date. Patients with a history of VTE within 3 months before the index date were excluded to mitigate the risk of misclassification of recurrent events.
In the sensitivity analyses, study participants were excluded if they either had a hospital diagnosis of atrial fibrillation before the index date or had filled ≥1 prescriptions for an anticoagulant medication within 90 days before the index date. Additionally, study participants were censored if they filled a prescription for an anticoagulant medication during follow-up.
Stroke severity and other potential predictors
2.4
We assembled a list of 16 potential predictors according to previously constructed VTE prediction scores and clinical knowledge (detailed description of each potential predictor is provided in Supplementary Table 2) [11,42,43]. These predictors included stroke severity; active cancer; previous VTE; smoking; recent trauma or surgery; other comorbidities, such as heart failure, chronic kidney disease, chronic obstructive pulmonary disease, chronic inflammatory disease, and paralysis; postmenopausal hormone replacement therapy; Essen risk score; educational level; and cohabitation status. The Essen risk score is a well-known, simple clinical score used to predict recurrent ischemic stroke and other cardiovascular outcomes (detailed description is provided in Supplementary Table 3) [44]. Potential predictors were identified from records in the Stroke Registry, hospital-based diagnoses recorded in the Patient Registry, and filled prescriptions recorded in the Prescription Registry.
Specifically for stroke severity, we looked further into its role as an independent predictor given its applicability to all stroke patients. Several scales have been developed to quantify neurologic impairments after stroke, such as the Scandinavian Stroke Scale (SSS) [45]. The SSS is a validated neurologic scale conceptually similar to the National Institutes of Health Stroke Scale (NIHSS) and assessed in patients with stroke at admission to a stroke unit [46]. SSS scores range from 0 (worst) to 58 (best) [45]. We grouped strokes into mild (SSS: 43-58), moderate (SSS: 26-42), or severe (SSS: 0-25) categories, which have been shown to correspond well with conventional NIHSS groups (mild [NIHSS: 0-5], moderate [NIHSS: 6-14], and severe [NIHSS: 15-31]) [46]. Supplementary Table 4 provides a detailed description of the SSS.
VTE and follow-up
2.5
The outcome was VTE, defined as a composite endpoint of deep vein thrombosis in the lower extremities and pulmonary embolism. VTE events were identified from primary and secondary inpatient or outpatient discharge diagnoses recorded in the Patient Registry after the index date. Since the positive predictive value differs immensely between the emergency department and all other departments (31% and 75%, respectively), the emergency department diagnoses were ignored to avoid misclassification [47].
We created 2 follow-up periods with the aim of examining the risk of VTE in the acute and subacute settings. Starting from the index date, study participants contributed with follow-up for 3 months (subacute phase) and 7 days (acute phase), or until the date of VTE diagnosis, emigration, death, or December 31, 2021, whichever occurred first.
Statistical analyses
2.6
To assess potential predictors, univariable analyses with 95% CIs for each potential predictor were performed with the Aalen-Johansen estimator, to estimate cumulative incidence proportions, and the Fine-Gray regression, to estimate subdistribution hazard ratios (SHRs) [48]. Death from any cause was considered a competing event. To evaluate the association between stroke severity and poststroke VTE and whether stroke severity is an independent predictor, we calculated adjusted SHRs in 2 multivariable analyses including age and sex (model 1), and selected predictors identified from the univariable analyses (model 2). Selected predictors were chosen if the SHR was either >1.10 or <0.90, with a 95% CI not overlapping 1 [49]. All analyses were calculated for ischemic stroke and intracerebral hemorrhage separately as for the subacute (3 months) and acute (7 days) phases.
In a sensitivity analysis, we repeated the analyses among patients not actively using anticoagulant therapy. Missing data were handled under the assumption of missing completely at random by applying complete-case analysis, including only individuals with complete information on all variables [50].
Results
3
Baseline characteristics
3.1
We identified 129,345 patients with first-time ischemic stroke and 16,887 patients with first-time intracerebral hemorrhage during 2004-2021. Among the patients with ischemic stroke, 1016 developed VTE (0.8%) in the first 3 months (subacute phase) and 487 (0.4%) developed VTE in the first 7 days (acute phase); the corresponding numbers after intracerebral hemorrhage were 200 (1.2%) and 78 (0.5%), respectively. The median age was 72 years (IQR: 62-81), and 46% were women. A total of 71% and 40% of the strokes were mild in patients with ischemic stroke and patients with intracerebral hemorrhage, respectively. Other baseline characteristics of the study participants are shown in Table 1.Table 1. Baseline characteristics of patients with ischemic stroke and intracerebral hemorrhage.CharacteristicIschemic stroke,N = 129,345Intracerebral hemorrhage,N = 16,887Age, median (IQR)72 (62, 81)73 (62, 82)Age group, n (%) <65 y38,482 (30%)4865 (29%) 65-79 y53,138 (41%)6697 (40%) ≥80 y37,725 (29%)5325 (32%)Sex, n (%) Female59,487 (46%)8108 (48%) Male69,858 (54%)8779 (52%)Stroke severitya, n (%) Mild86,225 (71%)6019 (40%) Moderate21,046 (17%)3553 (24%) Severe14,480 (12%)5507 (37%) Unknown75941808Active cancer, n (%)4712 (3.6%)585 (3.5%)Previous VTE, n (%)4810 (3.7%)646 (3.8%)Smoking status, n (%) Current/occasional38,736 (35%)3235 (27%) Former32,216 (29%)3618 (30%) Never40,349 (36%)5297 (44%) Unknown18,0444737Trauma/fracture or surgery 8 wk before, n (%)10,711 (8.3%)1415 (8.4%)Heart failure, n (%)8362 (6.5%)847 (5.0%)Chronic kidney disease, n (%)3419 (2.6%)445 (2.6%)COPD, n (%)18,544 (14%)2281 (14%)Chronic inflammatory diseases, n (%)7274 (5.6%)875 (5.2%)Paralysis, n (%)314 (0.2%)46 (0.3%)Postmenopausal hormone replacement therapy, n (%)5866 (4.5%)786 (4.7%)Essen stroke risk score, n (%) 08,302 (6.4%)1346 (8.0%) 120,220 (16%)2841 (17%) 227,788 (21%)3638 (22%) 332,180 (25%)4208 (25%) 424,293 (19%)3146 (19%) 5+16,562 (13%)1708 (10%)Education level, n (%) High17,267 (14%)2558 (16%) Low54,329 (45%)7026 (45%) Medium48,377 (40%)6103 (39%) Unknown93721200Cohabitation, n (%) Living alone59,892 (46%)7740 (46%) Living with partner69,135 (54%)9105 (54%) Unknown31842COPD, chronic obstructive pulmonary disease; VTE, venous thromboembolism,aAccording to Scandinavian Stroke Scale (SSS): Mild stroke (SSS: 43-58), moderate stroke (SSS: 26-42), and severe stroke (SSS: 0-25).
Predictors of VTE
3.2
Figures 1 and 2 provide an overview of the SHRs for all potential predictors in the subacute and acute phases for ischemic stroke and for intracerebral hemorrhage. Overall, the cumulative incidence proportions for VTE ranged from 0.2% to 2.8% across the potential predictors after ischemic stroke and from 0.1% to 5.6% after intracerebral hemorrhage.Figure 1. Forest plot with subdistribution hazard ratios for univariable analysis of potential predictors in ischemic stroke patients at subacute and acute phases. SHR, subdistribution hazard ratio; VTE, venous thromboembolism.Figure 2. Forest plot with subdistribution hazard ratios in univariable analyses of potential predictors in patients with intracerebral hemorrhage, in subacute and acute phases. SHR, subdistribution hazard ratio; VTE, venous thromboembolism.
In patients with ischemic stroke, greater stroke severity was associated with a higher risk of VTE. The SHRs in the subacute phase were 2.61 (95% CI: 2.25, 3.04) for moderate stroke and 3.38 (95% CI: 2.89, 3.95) for severe stroke, compared with mild stroke. A similar pattern with an even greater risk increase was observed in the acute phase. Among patients with intracerebral hemorrhage, those with moderate stroke had the highest risk of VTE. The SHRs during the subacute phase were 2.31 (95% CI: 1.61, 3.33) for moderate stroke and 1.33 (95% CI: 0.92, 1.93) for severe stroke, compared with mild stroke. A similar pattern with elevated risk was present in the acute phase.
Active cancer was associated with an elevated risk of VTE after ischemic stroke, with an SHR of 2.81 (95% CI: 2.28, 3.46) in the subacute phase. Comparable risks were found in the acute phase for ischemic stroke as well as in both time periods for patients with intracerebral hemorrhage. The risk of VTE after ischemic stroke was 4-fold higher in individuals with a history of previous VTE in the subacute phase (SHR: 4.01; 95% CI: 3.35, 4.81), a finding consistent with the risk in the acute phase. Similarly, patients with intracerebral hemorrhage with and without a history of previous VTE had comparable risk. More details on the cumulative incidence proportions and SHRs for all potential predictors in the subacute phase and acute phase are shown in Table 2 and Supplementary Table 5, respectively.Table 2. Risks and subdistribution hazard ratios for venous thromboembolism in the subacute phase for ischemic stroke and intracerebral hemorrhage.Potential predictorsIschemic stroke (N = 129,345)Intracerebral hemorrhage (N = 16,887)CIP, % (95% CI)Crude SHR (95% CI)CIP, % (95% CI)Crude SHR (95% CI)Stroke severity Mild0.50 (0.45, 0.55)Ref.0.84 (0.60, 1.07)Ref. Moderate1.30 (1.15, 1.45)2.61 (2.25, 3.04)1.92 (1.47, 2.38)2.31 (1.61, 3.33) Severe1.70 (2.49, 1.91)3.38 (2.89, 3.95)1.15 (0.87, 1.43)1.33 (0.92, 1.93)Age <65 y0.65 (0.57, 0.73)Ref.1.09 (0.80, 1.39)Ref. 65-79 y0.80 (0.73, 0.88)1.24 (1.06, 1.45)1.40 (1.11, 1.68)1.27 (0.90, 1.78) ≥80 y0.91 (0.81, 1.00)1.40 (1.19, 1.64)1.02 (0.75, 1.29)0.92 (0.63, 1.34)Sex Female0.89 (0.81, 0.96)Ref.1.00 (0.79, 1.22)Ref. Male0.70 (0.64, 0.76)0.79 (0.70, 0.89)1.36 (1.12, 1.60)1.36 (1.03, 1.81)Active cancer No0.74 (0.69, 0.79)Ref.1.14 (0.98, 1.30)Ref. Yes2.07 (1.66, 2.48)2.81 (2.28, 3.46)2.58 (1.29, 3.87)2.27 (1.34, 3.84)Previous VTE No0.71 (0.66, 0.76)Ref.1.01 (0.86, 1.17)Ref. Yes2.82 (2.35, 3.29)4.01 (3.35, 4.81)5.62 (3.84, 7.41)5.65 (3.94, 8.10)Smoking Never0.88 (0.79, 0.97)Ref.1.36 (1.05, 1.68)Ref. Current/occasional0.54 (0.36, 0.61)0.61 (0.51, 0.72)0.90 (0.57, 1.23)0.66 (0.43, 1.01) Former0.92 (0.82, 1.02)1.05 (0.90, 1.22)1.25 (0.89, 1.61)0.91 (0.63, 1.33)Recent trauma, fracture, or surgery (8 wk before) No0.75 (0.70, 0.80)Ref.1.16 (0.99, 1.33)Ref. Yes1.24 (1.03, 1.45)1.66 (1.38, 1.99)1.49 (0.86, 2.12)1.29 (0.82, 2.02)Heart failure No0.78 (0.73, 0.83)Ref.1.20 (1.03, 1.36)Ref. Yes0.91 (0.71, 1.12)1.17 (0.92, 1.47)1.07 (0.38, 1.77)0.88 (0.45, 1.72)Chronic kidney disease No0.79 (0.74, 0.84)Ref.1.19 (1.02, 1.36)Ref. Yes0.65 (0.38, 0.92)0.81 (0.53, 1.24)1.13 (0.15, 2.12)0.94 (0.39, 2.29)Chronic obstructive pulmonary disease No0.77 (0.72, 0.83)Ref.1.20 (1.03, 1.38)Ref. Yes0.88 (0.74, 1.01)1.13 (0.96, 1.34)1.10 (0.67, 1.53)0.91 (0.63, 1.33)Chronic inflammatory disease No0.78 (0.73, 0.83)Ref.1.18 (1.01, 1.35)Ref. Yes0.91 (0.69, 1.13)1.17 (0.91, 1.50)1.38 (0.60, 2.15)1.17 (0.65, 2.09)Paralysis No0.79 (0.74, 0.84)Ref.1.18 (1.02, 1.34)Ref. Yes0.96 (0.00, 2.04)1.22 (0.39, 3.80)4.35 (0.00, 10.24)3.74 (0.93, 15.12)Postmenopausal hormone replacement therapy No0.78 (0.73, 0.83)Ref.1.20 (1.03, 1.37)Ref. Yes0.94 (0.69, 1.19)1.21 (0.92, 1.58)0.89 (0.23, 1.55)0.74 (0.35, 1.58)Essen stroke risk score 00.85 (0.65, 1.04)Ref.0.97 (0.44, 1.49)Ref. 10.71 (0.60, 0.83)0.84 (0.63, 1.12)1.24 (0.83, 1.65)1.28 (0.68, 2.42) 20.81 (0.70, 0.91)0.95 (0.73, 1.25)1.35 (0.98, 1.73)1.39 (0.76, 2.57) 30.76 (0.67, 0.86)0.90 (0.69, 1.18)1.48 (1.11, 1.84)1.52 (0.83, 2.76) 40.83 (0.72, 0.94)0.98 (0.75, 1.29)0.90 (0.57, 1.23)0.91 (0.47, 1.76) 5+0.81 (0.67, 0.94)0.95 (0.71, 1.27)0.77 (0.35, 1.18)0.78 (0.36, 1.68)Education level High0.70 (0.57, 0.82)Ref.1.18 (0.76, 1.60)Ref. Medium0.77 (0.69, 0.85)1.10 (0.90, 1.35)1.33 (1.04, 1.62)1.13 (0.74, 1.72) Low0.85 (0.78, 0.93)1.22 (1.00, 1.49)1.10 (0.86, 1.34)0.93 (0.61, 1.41)Cohabitation Living with partner0.74 (0.67, 0.80)Ref.1.27 (1.04, 1.50)Ref. Living alone0.85 (0.78, 0.92)1.16 (1.02, 1.31)1.10 (0.87, 1.34)0.87 (0.66, 1.15)CIP, cumulative incidence proportion; Ref., reference; SHR, subdistribution hazard ratio; VTE, venous thromboembolism.
Association between stroke severity and VTE
3.3
The results from all multivariable analyses of stroke severity for both stroke subtypes and both time periods are shown in Table 3. Overall, additional adjustment for age and sex had little to no effect on the association between stroke severity and VTE. Estimates did not meaningfully change in the multivariable model with predictors selected from the univariable analyses. This pattern was observed in patients with ischemic stroke and those with intracerebral hemorrhage for both phases.Table 3. Subdistribution hazard ratios in multivariable analyses in acute and subacute phases after the index date for patients with ischemic stroke and intracerebral hemorrhage.Stroke severityIschemic stroke (N = 129,345)Intracerebral hemorrhage (N = 16,887)Model 1: crude SHR (95% CI)Model 2: adjusted SHRa (95% CI)Model 3: adjusted SHR (95% CI)Model 1: crude SHR (95% CI)Model 2: adjusted SHRa (95% CI)Model 3: adjusted SHR (95% CI)Acute phase MildRef.Ref.Ref.Ref.Ref.Ref. Moderate3.28 (2.63, 4.09)3.24 (2.57, 4.08)3.03 (2.35, 3.92)b4.07 (2.08, 7.98)4.20 (2.17, 8.13)4.19 (2.13, 8.24)c Severe4.48 (3.58, 5.61)4.37 (3.41, 5.59)4.83 (3.69, 6.33)b2.41 (1.23, 4.74)2.56 (1.29, 5.10)2.51 (1.27, 4.99)cSubacute phase MildRef.Ref.Ref.Ref.Ref.Ref. Moderate2.61 (2.25, 3.04)2.66 (2.27, 3.11)2.46 (2.07, 2.93)d2.31 (1.61, 3.33)2.34 (1.63, 3.37)2.36 (1.64, 3.40)c Severe3.38 (2.89, 3.95)3.44 (2.90, 4.09)3.66 (3.04, 4.41)d1.33 (0.92, 1.93)1.37 (0.94, 2.00)1.37 (0.94, 1.99)cRef., reference; SHR, subdistribution hazard ratio; VTE, venous thromboembolism.aAdjusted for age and sex.bAdjusted for selected predictors: stroke severity, age, sex, active cancer, previous VTE, smoking, recent trauma or surgery, postmenopausal hormone replacement therapy, education level, and cohabitation status.cAdjusted for selected predictors: stroke severity, sex, active cancer, and previous VTE.dAdjusted for selected predictors: stroke severity, age, sex, active cancer, previous VTE, smoking, recent trauma or surgery, and cohabitation status.
Sensitivity analyses
3.4
Supplementary Tables 6 and 7 show the results of the analyses restricted to patients with stroke who were not actively using anticoagulant therapy. The association between stroke severity and VTE was stronger in this study group compared with the original study group, for both ischemic stroke and intracerebral hemorrhage. The association between active cancer and VTE was also stronger, whereas the association between previous VTE and VTE was weaker. Similarly to findings in the main analyses, we did not observe substantial differences in SHRs for stroke severity from the univariable analyses after adjustment for both stroke subtypes and time periods (details in Supplemental Table 8).
Discussion
4
Principal findings
4.1
Our population-based cohort study indicated an increased risk of VTE ranging from 2-fold to 5-fold for stroke severity, active cancer, and previous VTE for both ischemic stroke and intracerebral hemorrhage, across both the subacute (3 months poststroke) and acute phases (7 days poststroke). The association between stroke severity and poststroke VTE remained strong after adjustment for both age and sex and predictors selected from univariable analyses.
Comparison with previous literature
4.2
Several studies have examined stroke severity and the risk of poststroke VTE in patients with ischemic stroke, but their findings on stroke severity as a predictor have been inconsistent [[14], [15], [16], [17], [18]]. Most of those studies were conducted in Asia, had short follow-up periods, and were at risk of selection bias (eg, by excluding patients who died within the first 7 days or were transferred to another hospital). A study by Kelly et al. [51], which used the Barthel Index to assess stroke severity, found that a subgroup of stroke patients with severe disability had an increased risk of VTE despite receiving standard thromboprophylaxis. Although the study had a small sample size, its findings are consistent with ours.
We found that patients with severe ischemic stroke were at highest risk of VTE, which is in line with several earlier studies [14,16,17]. In contrast, patients with moderate severity intracerebral hemorrhage were at highest risk of VTE compared with those with severe stroke. We are not aware of any other studies that evaluated stroke severity, as measured by a neurologic score scale, among patients with intracerebral hemorrhage. An explanation for the finding of moderate severity in patients with intracerebral hemorrhage having the highest risk might be a higher early mortality rate in the severe group than the moderate group. This may have resulted in a lower SHR for the severe group. Furthermore, our study showed that patients with intracerebral hemorrhage had a higher cumulative incidence of VTE compared with ischemic stroke patients. This may be explained by the differences in stroke severity; a greater proportion of intracerebral hemorrhage cases were classified as moderate to severe, whereas most ischemic stroke cases were mild. These findings support our conclusion that stroke severity is a key predictor of poststroke VTE—the more severe the stroke, the higher the likelihood of VTE.
Active cancer and previous VTE appeared to be strong predictors of VTE after stroke, both in the subacute and acute settings. These findings are consistent with those from existing studies in patients with ischemic stroke or stroke in general [1,4,13,18]. However, limited evidence is available regarding intracerebral hemorrhage alone. An American study of 2902 patients with intracerebral hemorrhage found a 6-fold elevated risk of developing VTE after stroke in patients who had a history of VTE. The study did not investigate cancer as a predictor [12].
Implications
4.3
The present study provides key information regarding clinical predictors of poststroke VTE, such as stroke severity, cancer, and previous VTE. These characteristics may aid clinicians in identifying patients at high risk of VTE after stroke. Notably, as stroke severity is assessed in every patient with stroke at admission, it is an important predictor applicable to all stroke patients.
Although VTE may be preventable with adequate thromboprophylaxis, continuing or initiating thromboprophylaxis after discharge is not yet common practice due to the inherent risk of bleeding. In subgroup analyses of randomized clinical trials, extended thromboprophylaxis for up to 4 weeks was associated with a 33% decreased risk of VTE among patients with ischemic stroke, corresponding to a number needed to treat of 40 [10]. Furthermore, the risk of major bleeding did not increase substantially by extending thromboprophylaxis from standard practice (major bleeding occurred in 1 more patient per 1000 in extended thromboprophylaxis compared to standard thromboprophylaxis) [10]. By identifying high-risk patients, our findings may help to improve the risk-benefit ratio of extended thromboprophylaxis beyond hospitalization. Additionally, future studies could build on these findings to develop a prediction model with relevant variables.
The benefit of extended thromboprophylaxis has been widely debated. For intracerebral hemorrhage, a survey from the United Kingdom has indicated that stroke physicians do not agree on the optimal method for VTE prevention. Some stroke physicians were uncertain about which patients should receive prophylaxis and the optimal type and duration of prophylaxis [37]. The correct answer should not necessarily be reduced to a single solution and is likely to vary by situation. Currently, guidelines do not advocate extended thromboprophylaxis, whereas for intracerebral hemorrhage, the decisions for each individual are almost completely at physicians’ discretion. Gaining a deeper understanding of clinical characteristics, particularly those predictive of adverse outcomes such as poststroke VTE, has the potential to assist clinicians in making better-informed decisions.
Limitations
4.4
This large population-based cohort study was based entirely on national registries with high quality and detailed data, and little to no loss of follow-up information. Nevertheless, our study should be interpreted within the context of its limitations. We had limited knowledge regarding medications during hospitalization and at other in-hospital facilities, such as hospital-based rehabilitation centers. Not all medications administered at hospitals is recorded in the registries; consequently, information on thromboprophylaxis during or after hospitalization was not available. The Danish Neurological Society’s guidelines are unclear for whom thromboprophylaxis is recommended during hospitalization, as well as the type and duration of thromboprophylaxis. Thus, our assumptions on thromboprophylaxis in hospitals were based on more general guidelines from the European Stroke Organisation or American Stroke Association [5,35,39]. These limitations might potentially have led to a misrepresentation of which patients actually received thromboprophylaxis during hospitalization, but it did not affect the main results of the study because we included all patients with stroke, regardless of their anticoagulant use. However, this aspect did limit our ability to further investigate the potential predictors in patients who did or did not receive thromboprophylaxis. Another limitation was the unavailable information on race/ethnicity, as ethnicity is not systematically recorded in the Patient Registry or Danish Civil Registration System [25,26]. The Danish population has a relatively stable and homogenous demography with regard to race.
Although the coding of first-time VTE diagnoses have high positive predictive value (88%) in the Patient Registry [52], distinguishing between first-time and recurrent VTE events is challenging. To decrease the risk of misclassification, we separated VTE events by time-related criteria in our study population (excluding patients with VTE event within the 90 days prior to the index date). Further, a relatively low sensitivity of VTE is expected in the Danish registries as only symptomatic events will receive medical attention and ultimately be coded. Due to this presumed underdiagnosis, the absolute risks in this study were almost certainly underestimated. For example, the CLOTS (The Clots in Legs Or sTockings after Stroke) trials showed a higher risk of poststroke VTE (∼10%) [53].
Immobilization is a well-established risk-factor for VTE. However, we were unable to identify valid surrogate markers for poststroke immobility [5]. We assume that diagnosis codes for paralysis primarily capture permanent deficits, whereas rather acute and potentially reversible impairments, more relevant in early poststroke phases, are not reliably recorded. It should also be noted that we did not to stratify VTE into deep vein thrombosis and pulmonary embolism in our analyses. Although such stratification could offer additional clinical insights, pulmonary embolism is notoriously difficult to diagnose. Consequently, undiagnosed fatal cases may not be captured in the registries, introducing considerably uncertainty into the estimates.
Conclusion
5
Our study shows that stroke severity, active cancer, and previous VTE are strong predictors of poststroke risk of VTE in both subacute and acute phases. Among these predictors, stroke severity is strongly associated with poststroke VTE even after adjustments. These findings offer valuable insights for clinicians and can be used to identify patients at elevated risk of VTE in whom extended thromboprophylaxis may be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Corraini P.Ording A.G.Henderson V.W.Szépligeti S.Horváth-PuhóE.Sørensen H.T.Cancer, other comorbidity, and risk of venous thromboembolism after stroke: a population-based cohort study Thromb Res 147201688932771085710.1016/j.thromres.2016.09.029 · doi ↗ · pubmed ↗
- 2Rinde L.B.Småbrekke B.Mathiesen E.B.Løchen M.L.Njølstad I.Hald E.M.Ischemic stroke and risk of venous thromboembolism in the general population: the Tromsø Study J Am Heart Assoc 52016 e 00431110.1161/JAHA.116.004311 PMC 521033227821402 · doi ↗ · pubmed ↗
- 3Piazza G.Goldhaber S.Z.Kroll A.Goldberg R.J.Emery C.Spencer F.A.Venous thromboembolism in patients with prior stroke Clin Appl Thromb Hemost 20201443492363700410.1177/1076029613487430 · doi ↗ · pubmed ↗
- 4Pongmoragot J.Rabinstein A.A.Nilanont Y.Swartz R.H.Zhou L.Saposnik G.Investigators of Registry of Canadian Stroke Network (RCSN) and University of Toronto Stroke Program for Stroke Outcomes Research Canada (SOR Can [www.sorcan.ca]) Working Group. Pulmonary embolism in ischemic stroke: clinical presentation, risk factors, and outcome J Am Heart Assoc 22013 e 00037210.1161/JAHA.113.000372 PMC 388677824275627 · doi ↗ · pubmed ↗
- 5Dennis M.Caso V.Kappelle L.J.Pavlovic A.Sandercock P.European Stroke Organisation European Stroke Organisation (ESO) guidelines for prophylaxis for venous thromboembolism in immobile patients with acute ischaemic stroke Eur Stroke J 120166193100826310.1177/2396987316628384 PMC 6301216 · doi ↗ · pubmed ↗
- 6Cohen A.T.Harrington R.A.Goldhaber S.Z.Hull R.D.Wiens B.L.Gold A.APEX Investigators Extended thromboprophylaxis with betrixaban in acutely ill medical patients N Engl J Med 37520165345442723264910.1056/NEJ Moa 1601747 · doi ↗ · pubmed ↗
- 7Spyropoulos A.C.Ageno W.Albers G.W.Elliott C.G.Halperin J.L.Hiatt W.R.MARINER Investigators Rivaroxaban for thromboprophylaxis after hospitalization for medical illness N Engl J Med 3792018111811273014594610.1056/NEJ Moa 1805090 · doi ↗ · pubmed ↗
- 8Cohen A.T.Spiro T.E.Büller H.R.Haskell L.Hu D.Hull R.MAGELLAN Investigators Rivaroxaban for thromboprophylaxis in acutely ill medical patients N Engl J Med 36820135135232338800310.1056/NEJ Moa 1111096 · doi ↗ · pubmed ↗