Prognostic value of [18F]fluorodeoxyglucose PET/CT in the new staging system for non-small cell lung cancer
Wonseok Whi, Hyunjong Lee, Sang-Won Um, Hong Kwan Kim, Hong Ryul Pyo, Myung-Ju Ahn, Joon Young Choi

TL;DR
This study shows that adding FDG PET/CT tumor uptake to the new NSCLC staging system improves survival prediction and risk stratification for patients.
Contribution
The study proposes a new staging system for NSCLC that integrates FDG SUVmax for better prognostic accuracy.
Findings
Primary tumor FDG uptake was an independent prognostic factor for overall and disease-free survival.
Incorporating SUVmax into staging improved risk stratification, especially in intermediate stages.
Abstract
This study aims to explore the prognostic value of primary tumor [18F]fluorodeoxyglucose (FDG) uptake in non-small cell lung cancer (NSCLC) patients treated with curative therapy, particularly when considered alongside the new 9th edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) staging system. A single-center retrospective study analyzed 3070 NSCLC patients who underwent pretherapeutic FDG PET/CT for initial staging. The survival analyses considered clinical variables, disease stage, and the primary tumor’s maximum standardized uptake value (SUVmax). Univariate and multivariate analyses evaluated the prognostic significance of disease stage and SUVmax in predicting overall and disease-free survival. A new staging system incorporating SUVmax is proposed and compared with the conventional staging. Two thousand nine hundred…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
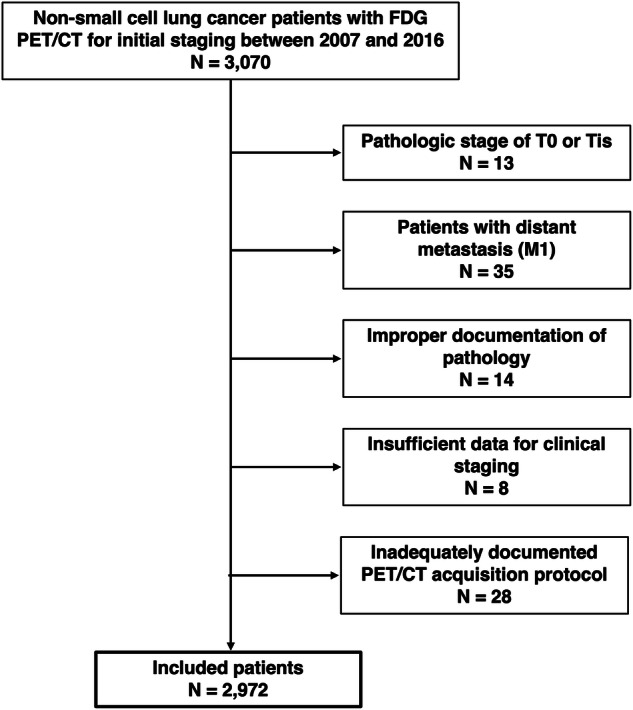 Figure 1
Figure 1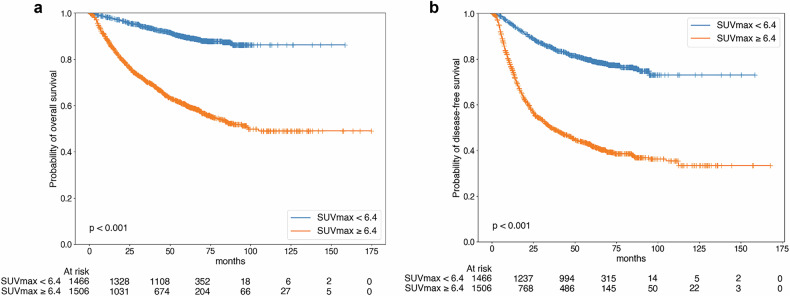 Figure 2
Figure 2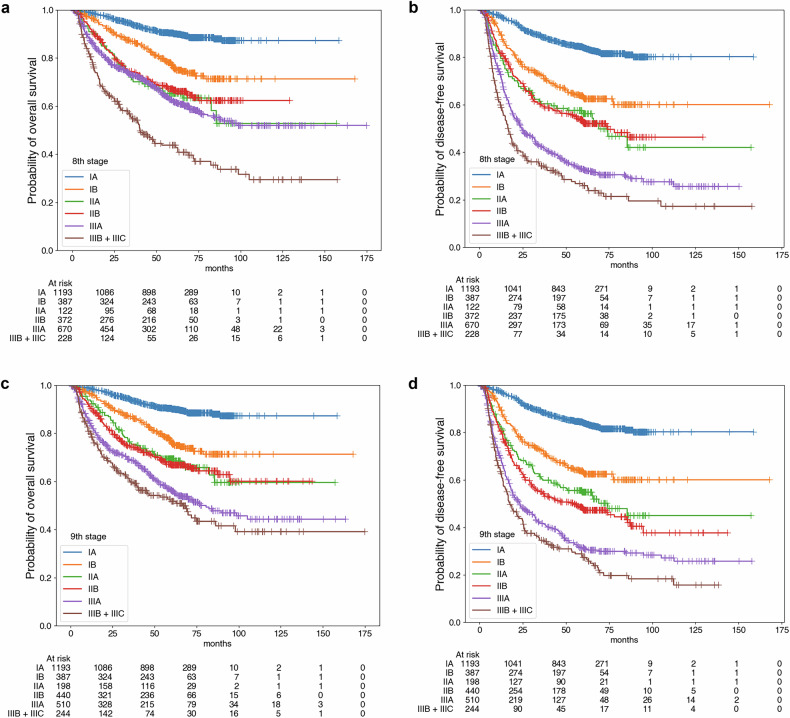 Figure 3
Figure 3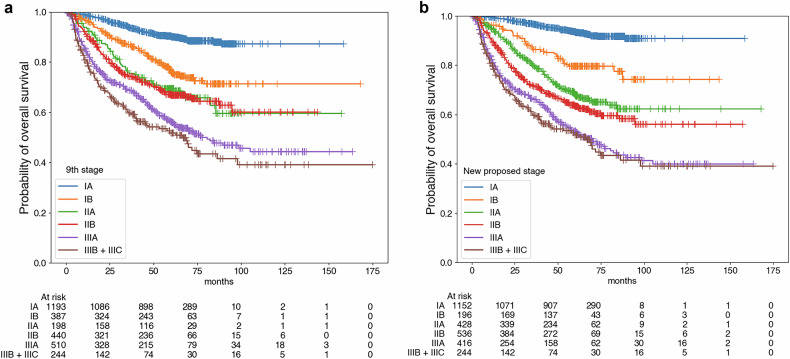 Figure 4
Figure 4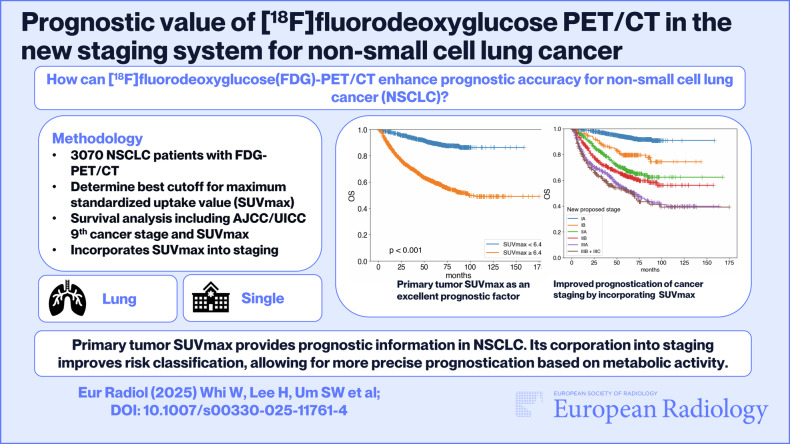 Figure 5
Figure 5- —National Research Foundation of Korea (NRF)
- —Samsung Medical Center
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Medical Imaging Techniques and Applications · Radiomics and Machine Learning in Medical Imaging
Introduction
Lung cancer remains one of the leading causes of cancer-related mortality worldwide, with non-small cell lung cancer (NSCLC) accounting for approximately 84% of all lung cancer cases [1]. Accurate staging and prognosis assessment of NSCLC after definitive therapy are crucial for guiding treatment and optimizing patient care. [^18^F]Fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) is an essential tool in the initial staging and prognostication of NSCLC [2, 3]. In addition to detecting metastatic lesions, PET/CT provides metabolic parameters such as the maximum standardized uptake value (SUVmax), which reflects tumor glucose metabolism. Numerous studies have demonstrated that higher SUVmax values are associated with poorer prognoses in various cancers, including NSCLC [4, 5]. Notably, a previous study has reported that incorporating SUVmax into the current staging system may enhance prognostic accuracy [6].
The cancer staging system developed and suggested by the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) is the most widely adopted framework for assessing the extent and progression of malignancies, including NSCLC. This system provides a standardized approach for classifying a tumor’s primary size and extent (T), lymph node involvement (N), and presence of metastases (M) to guide clinical decision-making and prognostication. In 2024, the 9th edition of the AJCC/UICC staging system for NSCLC was proposed [7, 8]. A notable change between the 8th and 9th editions of the system is the further subdivision of the N2 stage into N2a and N2b based on the number of involved lymph node stations, which were previously classified as N2 metastasis. This modification has led to the reclassification of stages II and III and their respective substages. Additionally, the 9th edition introduced a distinction within the M1c category, further dividing it into M1c1 and M1c2 based on the number of organs involved in metastases. The criteria for the T stage have remained consistent. In a survival analysis, the staging system based on the 9th edition showed enhanced prognostic stratification compared with the 8th edition [7]. However, no prior studies have investigated the independent prognostic significance of FDG PET/CT parameters, such as SUVmax, within the framework of the 9th edition AJCC/UICC staging system for lung cancer.
In this retrospective study, we investigated the prognostic value of primary tumor FDG uptake shown as SUVmax according to the 8th and 9th editions of the AJCC/UICC staging system in a large cohort of patients with NSCLC. Additionally, we explored whether incorporating SUVmax into the 9th edition AJCC/UICC staging could further enhance prognostic accuracy.
Materials and methods
Subjects
Our institutional review board (IRB) approved this retrospective study and waived the requirement for informed consent (IRB No. 2024-12-095). We retrospectively enrolled 3,070 consecutive patients who underwent FDG PET/CT examination for initial staging of NSCLC and subsequent definitive therapies between January 2007 and December 2016. Among them, 13 patients with a pathologic stage of T0 or Tis and 35 patients with distant metastasis (M1) were excluded. Fourteen patients without properly documented pathologic information were also excluded, along with eight patients whose data were inadequate for clinical staging. Finally, 28 patients without an adequately documented FDG PET/CT acquisition protocol were excluded. Therefore, data from 2972 patients were analyzed in this study.
All primary lung cancer lesions were pathologically confirmed using one of the following methods: surgical specimens for patients who underwent surgical resection, or biopsy and cytology for patients who did not undergo surgery. For all included NSCLC patients, chest X-ray, contrast-enhanced chest CT, FDG PET/CT, and bronchoscopy were performed as the standard protocol for initial staging of the disease. Additional radiologic tests, including endobronchial ultrasound-guided biopsy, brain magnetic resonance imaging (MRI), contrast-enhanced abdominal CT, contrast-enhanced adrenal CT, and liver MRI, were performed as clinically indicated based on findings from prior examinations that warranted further evaluation of specific regions.
FDG PET/CT acquisition and analysis
All patients fasted for at least 6 h, and the blood glucose concentration was restricted to < 200 mg/dL at the time of FDG injection. Imaging was performed using a Discovery LS (GE Healthcare) or Discovery STE (GE Healthcare) after 60 min of FDG distribution (5 MBq/kg or 13.5 μCi/kg). Continuous spiral CT scans were performed using eight-slice helical CT (140 keV, 40–120 mA, Discovery LS) or 16-slice helical CT (140 keV, 30–170 mA, Discovery STE). Emission scans were obtained from head to thigh, at 4 min per frame in 2D mode (Discovery LS) or 2.5 min per frame in 3D mode (Discovery STE). PET images were reconstructed with CT for attenuation correction using the ordered-subsets expectation maximization algorithm with 28 subsets and two iterations (matrix 128 × 128, voxel size 4.3 × 4.3 × 3.9 mm, Discovery LS) or the ordered-subsets expectation maximization algorithm with 20 subsets and two iterations (matrix 128×128, voxel size 3.9 × 3.9 × 3.3 mm, Discovery STE). The SUV was calculated with adjustment for the administered FDG dose and body weight.
All images were interpreted by two or more experienced nuclear medicine physicians, and at least one had more than 10 years of experience in reading FDG PET/CT results. Image interpretation was based on visual inspection with semiquantitative analyses. Using volume viewer software on a GE Advantage Workstation version 4.7, the primary tumor SUVmax was measured in a spherical volume of interest, as no other volumetric parameters were utilized in this study.
Collection of clinical variables
Clinical information (sex, age, and histological grade of the primary tumor) was obtained by reviewing electronic medical records. We assigned a pathologic stage for each patient undergoing initial curative surgery and a clinical stage for those treated with definitive radiotherapy or curative surgery preceded by neoadjuvant concurrent chemoradiotherapy (CCRT). Pathology reports acquired from surgery were reviewed to determine the pathologic stage. Radiologic reports of FDG PET/CT and chest CT scans were reviewed for clinical staging. The size of the primary tumor was determined based on the CT scan. The clinical nodal stage was evaluated by considering a lymph node station as positive if any of the FDG PET/CT, chest CT, or fine needle aspiration biopsy (if performed) results showed positivity. Both staging procedures were performed based on the 8th and 9th editions of the AJCC/UICC staging system.
For 2043 surgically treated patients, hilar and mediastinal lymphadenectomy was performed in 1666 (81.5%) cases. Among them, systematic lymph node dissection was conducted in 1550 (93.0%) cases, while lymph node sampling was performed in 116 (7.0%) cases based on intraoperative findings and surgical judgment. Adjuvant therapy after surgery was performed based on the patient's situation and the physician's decision. After surgery, all patients were monitored regularly to obtain accurate information about recurrence. Patients were scheduled for routine follow-up every 3–6 months for the first three years after curative-intent therapy and then every six months thereafter. Every follow-up evaluation included a physical examination, laboratory tests, biochemical screening, chest X-ray, and chest CT scan. FDG PET/CT or other relevant tests were also performed if clinically indicated. Recurrence or metastasis was considered when there was an abnormal finding on serial imaging studies or pathologically confirmed malignancy. The events for survival analysis were defined as recurrence or metastasis and death from any cause. The overall survival (OS) and disease-free survival (DFS) durations were defined as the intervals from the date of histological diagnosis to the date of death, disease recurrence, or the last follow-up.
Statistical analysis
Age was divided into three ranges as a discrete scale according to tertile points for the log-rank tests and multivariate analyses. SUVmax values were harmonized to remove batch effects due to varying PET/CT instruments, using the package neuroCombat in R. Harmonized SUVmax values were divided into two groups as a discrete scale (high and low) at the value that best discriminated the OS in all subjects; in other words, the cutoff was statistically determined by maximizing the rank-based test statistic for OS. An area under the receiver operating characteristic curve (AUC) analysis was additionally performed to evaluate the discriminatory performance of this cutoff. Cutoff values were applied not only for the log-rank tests and multivariate analyses but also as suggestions for a reference value in the new staging system.
Sex, age (as both continuous and discrete variables), adjuvant therapy, histological grade of the primary tumor, pathological/clinical T/N stages, stage (e.g., IA and IB) based on 8th and 9th editions of the AJCC/UICC staging system, and SUVmax (as both discrete and continuous scales) were used in the univariate survival analyses. Due to the small sample size of Stage IA1 and the complexity of the study design, Stage IA subgroups (IA1, IA2, and IA3) were analyzed as a combined Stage IA group.
Both OS and DFS were endpoints of the analyses. The Cox proportional hazards model was used to evaluate each variable’s prognostic power. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated. Log-rank statistics were obtained using the Kaplan–Meier method. Variables significant in the univariate survival analyses (log-rank statistics with a p-value less than 0.05) were included in the multivariate survival analyses. Variables with collinearity were excluded.
Patients in each 9th-edition staging group were divided into two groups based on the reference values for SUVmax. HRs and 95% CIs based on OS were estimated, and log-rank statistics were obtained using the Kaplan–Meier method. Subgroup members were upstaged or downstaged to new groups as needed based on the HRs, with some remaining in their original group. Pair-wise Kaplan–Meier analyses were conducted in the newly classified groups. All statistical analyses were performed using Pandas software version 2.2 (NumFOCUS) and R software (v.4.0.4, R Foundation for Statistical Computing). p-values lower than 0.05 were considered statistically significant.
Results
Demographic data
A total of 2972 patients were included in the analysis (Fig. 1). The clinical characteristics and demographics of the subjects are described in Table 1. Of the total patients, 63.5% were male. The median age of the subjects was 65 years, and the median SUVmax was 6.6. The cutoff value for SUVmax was determined to be 6.4 (AUC = 0.73, c-index = 0.68, sensitivity = 0.58, specificity = 0.79), which was identified as optimal using both rank-based and AUC-based analyses. Stage IA was the most common group according to both the 8th and 9th edition staging criteria, and stage IIIA was the most common clinical substage according to both the 8th and 9th edition criteria. Because the number of subjects with stage IIIC (the criterion for which is unchanged in the 9th edition) was small (n = 35), those patients were combined with the IIIB group for analysis.Fig. 1. Inclusion and exclusion criteria. This study retrospectively enrolled 3070 consecutive patients with FDG PET/CT results from an initial staging of NSCLC and subsequent definitive therapies between January 2007 and December 2016. Among them, patients with a pathologic stage of T0 or Tis, with distant metastasis (M1), without properly documented pathologic information, without data adequate for clinical staging, or without an adequately documented FDG PET/CT acquisition protocol were excluded. After exclusions, data for 2972 patients were analyzed in this studyTable 1Demographic and clinical characteristics of the included NSCLC patientsVariableNumber (%)Age at diagnosis, range (median)21–97 (65) Younger (< 61)1019 (34.3%) Intermediate (61–69)949 (31.9%) Older (> 69)1004 (33.8%)Sex Male1888 (63.5%) Female1084 (36.5%)SUVmax, median6.6 < 6.41466 (49.3%) ≥ 6.41506 (50.7%)Cell type Adenocarcinoma2039 (68.6%) Non-adenocarcinoma933 (31.4%)Treatment modality Initial surgery ± adjuvant chemotherapy2043 (68.7%) Definitive radiotherapy ± adjuvant chemotherapy482 (16.2%) Neoadjuvant chemoradiotherapy + surgery447 (15.0%)T stage T1a127 (4.3%) T1b586 (19.7%) T1c764 (25.7%) T2a637 (21.4%) T2b287 (9.6%) T3394 (13.3%) T4177 (6.0%)8th N stage N01986 (66.8%) N1251 (8.4%) N2710 (23.9%) N325 (0.8%)9th N stage N01986 (66.8%) N1251 (8.4%) N2a471 (15.8%) N2b239 (8.0%) N325 (0.8%)8th stage group IA1193 (40.1%) IB387 (13.0%) IIA122 (4.1%) IIB372 (12.5%) IIIA670 (22.5%) IIIB193 (6.5%) IIIC35 (1.2%)9th stage group IA1193 (40.1%) IB387 (13.0%) IIA198 (6.7%) IIB440 (14.8%) IIIA510 (17.2%) IIIB209 (7.0%) IIIC35 (1.2%)Instrument Discovery LS736 (24.8%) Discovery STE2236 (75.2%)SUVmax maximum standardized uptake value
Survival analysis data
In univariate survival analysis, age, sex, treatment modality, cell type, T stage, N stage (8th/9th), stage group (8th/9th), and SUVmax as both a continuous and discrete scale were significant prognostic factors for both OS and DFS (Table 2).Table 2. Univariate Cox regression analyses and log-rank analyses of survival in NSCLC patientsVariableCategoriesOSDFSHR (95% CI)pLog-rankHR (95% CI)pLog-rankAge< 61< 0.001< 0.00161–692.03 (1.64–2.51)< 0.0011.22 (1.05–1.42)0.01> 693.90 (3.20–4.76)< 0.0011.80 (1.56–2.07)< 0.001Age (cont.)1.06 (1.05–1.07)< 0.001< 0.0011.02 (1.02–1.03)< 0.001< 0.001SexFemale< 0.001< 0.001Male2.56 (2.14–3.06)< 0.0011.66 (1.46–1.89)< 0.001TreatmentSurgery^a^< 0.001< 0.001Definitive RT^a^5.98 (5.05–7.10)< 0.0013.12 (2.69–3.63)< 0.001Neoadjuvant CCRT^b^3.18 (2.64–3.84)< 0.0013.69 (3.21–4.24)< 0.001Cell typeAdenocarcinoma< 0.001< 0.001Non-adenocarcinoma2.95 (2.55–3.42)< 0.0011.71 (1.52–1.93)< 0.001T stageT1a< 0.001< 0.001T1b1.78 (0.89–3.56)0.101.76 (1.03–3.02)0.04T1c2.49 (1.26–4.90)0.0083.07 (1.82–5.18)< 0.001T2a4.30 (2.20–8.42)< 0.0015.10 (3.05–8.58)< 0.001T2b7.43 (3.37–14.66)< 0.0017.23 (4.26–12.28)< 0.001T39.04 (4.62–17.67)< 0.0017.90 (4.68–13.33)< 0.001T410.97 (5.51–21.80)< 0.0018.86 (5.15–15.24)< 0.0018th N stageN0< 0.001< 0.001N12.17 (1.71–2.76)< 0.0012.55 (2.10–3.10)< 0.001N22.66 (2.27–3.11)< 0.0013.97 (3.50–4.50)< 0.001N37.48 (4.53–12.36)< 0.0016.95 (4.39–11.00)< 0.0019th N stageN0< 0.001< 0.001N12.17 (1.71–2.76)< 0.0012.56 (2.10–3.11)< 0.001N2a2.57 (2.14–3.08)< 0.0013.84 (3.33–4.43)< 0.001N2b2.87 (2.29–3.59)< 0.0014.26 (3.58–5.08)< 0.001N37.49 (4.53–12.37)< 0.0016.95 (4.39–11.01)< 0.0018th stage groupIA< 0.001< 0.001IB2.50 (1.89–3.30)< 0.0012.54 (2.04–3.17)< 0.001IIA4.28 (3.02–6.07)< 0.0013.70 (2.74–4.98)< 0.001IIB3.91 (3.03–5.05)< 0.0013.69 (2.99–4.54)< 0.001IIIA4.75 (3.80–5.92)< 0.0016.48 (5.45–7.69)< 0.001IIIB + IIIC^c^8.88 (6.88–11.46)< 0.0018.75 (7.08–10.82)< 0.0019th stage groupIA< 0.001< 0.001IB2.50 (1.89–3.30)< 0.0012.54 (2.04–3.17)< 0.001IIA3.64 (2.67–4.96)< 0.0013.64 (2.83–4.68)< 0.001IIB3.84 (3.00–4.91)< 0.0014.33 (3.57–5.26)< 0.001IIIA5.80 (4.63–7.26)< 0.0016.73 (5.62–8.06)< 0.001IIIB + IIIC^c^7.18 (5.54–9.31)< 0.0018.32 (6.76–10.25)< 0.001SUVmax (categorized)< 6.4< 0.001< 0.001≥ 6.44.74 (3.97–5.67)< 0.0013.87 (3.39–4.42)< 0.001SUVmax (continuous)1.09 (1.08–1.10)< 0.001< 0.0011.08 (1.07–1.08)< 0.001< 0.001HR hazard ratio, CI confidence interval, RT radiotherapy, CCRT concurrent chemoradiotherapy, SUVmax maximum standardized uptake value^a^ With or without subsequent adjuvant chemotherapy^b^ Followed by surgery^c^ Due to the small sample size of stage group IIIC, it was combined into the IIIB group
Due to multicollinearity issues, the multivariate survival analysis was performed for each PET parameter and staging system. In the multivariate survival analysis, age, sex, treatment modality (definitive radiotherapy group vs initial surgery group), stage group (8th/9th), and SUVmax were significant prognostic factors for OS, and treatment modality (neoadjuvant CCRT + surgery group vs initial surgery group), stage group (8th/9th), and SUVmax were significant prognostic factors for DFS (Supplementary Tables 1 and 2). Survival curves according to SUVmax and the 8th/9th edition stage groups are displayed in Figs. 2 and 3.Fig. 2. Kaplan–Meier survival curves according to SUVmax. SUVmax discriminated by the best cutoff value for discriminating the prognosis of OS was a significant prognostic factor in both overall (a) and DFS (b)Fig. 3. Survival curves for each prognostic stage group suggested by the AJCC/UICC staging guidelines, 8th and 9th editions. For the 8th edition, the prognostic stage group was a significant prognostic factor for both overall (a) and disease-free (b) survival. The result was the same for the stage groups in the 9th edition for overall (c) and disease-free (d) survival
Proposing a new staging system including SUVmax
Subgroup analyses were performed to explore the role of SUVmax in each stage and adjust the staging system to achieve more accurate prognoses. HRs for OS were calculated in subgroups classified according to each 9th edition cancer stage and SUVmax group (Supplementary Table 3). Our proposed new staging system was designed based on those results. Stage IB subjects with low SUVmax were downstaged to a new stage IA. Stage IIA and IIB subjects with low SUVmax were downstaged to a new stage IB. Stage IA and IB subjects with high SUVmax were upstaged to stage IIA. Stage IIA patients with high SUVmax were upstaged, and stage IIIA patients with low SUVmax were downstaged to the new stage IIB. These changes are summarized in Table 3.Table 3. The new proposed staging system is based on the AJCC/UICC 9th edition stage group and SUVmaxAJCC/UICC 9th ed. stage groupSUVmax^a^New proposed stage groupIALowIAIBLowIIALowIBIIBLowIAHighIIAIBHighIIAHighIIBIIBHighIIIALowIIIAHighIIIAIIIBIIIBIIICAJCC American Joint Committee on Cancer, UICC Union for International Cancer Control, SUVmax maximum standardized uptake value^a^ Categorized by a cutoff value of 6.4, as determined to discriminate the OS best
In the conventional staging system, OS did not differ significantly between subjects in stages IIA/IIB (HR =1.06, p = 0.72) and IIIA/IIIB (HR = 1.22, p = 0.08). In the new staging system, subjects in stages IIA and IIB did differ significantly in OS (HR = 1.27, p = 0.04), though subjects in stages IIIA and IIIB were still not discriminated (HR = 1.10, p = 0.42) (Table 4). Compared with survival curves based on the 9th edition stage groups, those based on our proposed staging system better discriminated prognoses between stages IIA and IIB (Fig. 4).Fig. 4. Survival curves according to AJCC/UICC 9th edition cancer stages and the new proposed stages. Compared with survival curves based on the 9th edition stage groups (a), subjects in stages IIA and IIB in the new proposed staging system showed significant differences in OS when SUVmax was incorporated into the staging system (b). However, the new staging system still did not discriminate against subjects in stages IIIA and IIIBTable 4Univariate Cox regression analyses (pairwise) of OS according to the conventional system and the newly proposed staging system that considers the SUVmax of the primary NSCLC lesionConventional staging (9th ed.)New proposed stagingHR (95% CI)pHR (95% CI)pStage IA vs IB2.54 (1.92–3.36)< 0.0013.20 (2.17–4.73)< 0.001Stage IB vs IIA1.47 (1.06–2.03)0.021.74 (1.21–2.50)0.003Stage IIA vs IIB1.06 (0.78–1.43)0.721.27 (1.01–1.58)0.04Stage IIB vs IIIA1.50 (1.21–1.86)< 0.0011.45 (1.18–1.77)< 0.001Stage IIIA vs IIIB^a^1.22 (0.97–1.54)0.081.10 (0.87–1.39)0.42HR hazard ratio, CI confidence interval^a^ Incorporates stage IIIC from the conventional system
Discussion
In this study, we identified the SUVmax of primary tumors from FDG PET/CT scans as a significant prognostic factor for patients with NSCLC, independent of the 8th and 9th edition AJCC/UICC tumor, node, metastasis (TNM) staging systems. Both our univariate and multivariate analyses demonstrated the prognostic power of SUVmax, highlighting its ability to provide additional stratification within individual stage groups. Incorporating SUVmax into the staging system improved prognostic discrimination compared with the conventional staging methods alone. Thus, a staging system integrating primary tumor FDG uptake could be a refined tool for risk assessment.
The SUVmax of the primary tumor, the most widely used semi-quantitative parameter from FDG PET/CT, reflects tumor glucose metabolism and serves as an indicator of biological aggressiveness [9]. Numerous studies have emphasized its utility, consistently showing that higher SUVmax values are linked to poorer outcomes across various cancers, including NSCLC [10–13]. One of the key advantages of this metric is its ease of measurement and high reproducibility, making it particularly suitable for routine clinical application. As a result, SUVmax is widely adopted in clinical practice as a versatile and practical parameter.
FDG PET/CT plays a pivotal role in both the diagnostic and prognostic landscapes of NSCLC [14]. Previous studies have demonstrated the prognostic relevance of SUVmax in NSCLC. For example, elevated SUVmax values have been associated with poor survival [4, 11] and high recurrence rates [5, 12]. However, most prior research has been limited by small cohorts or not based on recent staging revisions. For example, Takeda et al recruited 95 patients who received stereotactic body radiotherapy [5], Imamura et al enrolled 62 NSCLC patients receiving chemotherapy [15], and Yoo et al used 80 patients without lymph node metastasis [16]. Some meta-analyses included multiple studies and a larger number of patients: Berghsmans et al enrolled 13 studies and 1474 NSCLC patients [4], and Paesman et al included 2637 patients from 21 studies [11]. To our knowledge, the present study is the first single-center study to analyze the prognostic significance of SUVmax in a cohort of this scale under the framework of the updated 9th edition AJCC/UICC staging system.
In current practice, the management of NSCLC is primarily guided by the TNM staging system, with treatment options ranging from surgical resection for early-stage disease to systemic therapy for advanced stages [17, 18]. However, our study suggests that incorporating SUVmax from FDG PET/CT scans could refine this approach, particularly for patients with stage II or lower NSCLC. Patients with high SUVmax, even within the early stages, might represent a high-risk group that could benefit from more aggressive treatment strategies or closer surveillance. For instance, stage II patients with high SUVmax might be considered for more intensive adjuvant therapy or shorter follow-up intervals, similar to the approach for higher-stage disease. Conversely, patients with low SUVmax values might be candidates for less intensive follow-up regimens. This nuanced approach could lead to more personalized treatment plans, potentially improving outcomes while avoiding overtreatment in lower-risk patients. Further prospective studies are needed to validate the clinical impact of incorporating SUVmax into treatment algorithms, but our findings suggest that it is a promising avenue for enhancing the precision of NSCLC management.
Despite its potential, this study has limitations. First, pathological staging was available only for surgically treated patients, and significant delays between clinical and pathological staging may have introduced bias. However, a subgroup analysis restricted to patients with pathological staging showed consistent results, supporting the robustness of our findings (Supplementary Tables 7 and 8). Second, as a retrospective study, treatment strategies were based on the 6th and 7th editions of the AJCC/UICC staging systems, potentially introducing heterogeneity and not accounting for recent advancements in treatment modalities and concepts, which have significantly improved survival outcomes in NSCLC patients. To address this concern, we performed an additional subgroup analysis limited to patients initially staged and managed according to the 7th edition, which demonstrated consistent prognostic results (Supplementary Tables 9 and 10). Third, as a retrospective study, detailed nodal information required for rigorous pathological nodal staging according to the latest 9th TNM edition was not fully available due to practical considerations, given the invasive nature and associated risks of procedures. Moreover, quantitative nodal FDG uptake parameters from PET/CT, which might have provided additional prognostic value, were not systematically analyzed, warranting further prospective studies. Fourth, volume-based PET parameters, such as metabolic tumor volume or total lesion glycolysis, which are generally considered superior to SUVmax for prognostic prediction [19, 20], were not included in this study. However, SUVmax is more clinically applicable than volume-based parameters due to its simplicity and ease of measurement, and the favorable results of this study demonstrate its value. Fifth, while our proposed staging system demonstrated improved prognostic stratification, the modified clinical decisions by up- or down-staging regarding treatment are not reflected in the prognosis. Prospective validation studies are required to clarify its role in guiding treatment decisions. Finally, as a single-center study, our proposed staging system incorporating SUVmax requires external validation through collaboration with other high-volume lung cancer centers to confirm reproducibility and generalizability.
In conclusion, the primary tumor FDG uptake, shown as SUVmax on PET/CT scans, was identified as an independent prognostic factor in NSCLC patients receiving curative treatment, along with the stage group according to both the 8th and 9th editions of the AJCC/UICC staging systems. The newly proposed staging system incorporating SUVmax demonstrates the potential to discriminate prognoses better than the conventional staging approach.
Supplementary information
ELECTRONIC SUPPLEMENTARY MATERIAL
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rami-Porta R, Nishimura KK, Giroux DJ et al (2024) The International Association for the Study of Lung Cancer Lung Cancer Staging project: proposals for revision of the TNM stage groups in the forthcoming (Ninth) edition of the TNM classification for lung cancer. J Thorac Oncol 19:1007–102710.1016/j.jtho.2024.02.01138447919 · doi ↗ · pubmed ↗
- 2Detterbeck FC, Woodard GA, Bader AS et al (2024) The proposed 9th edition TNM classification of lung cancer. Chest 166:882–89510.1016/j.chest.2024.05.02638885896 · doi ↗ · pubmed ↗