Neurosurgical management of geriatric patients with traumatic brain injury in a medium-developed Chinese city: a recent-years overview
Xiao-ting Fan, Hai-ying Zhao, Chuan-fu Wu, Bao-xiang Gao, Jian Li, Yan Xu, Yong-gang Lian, Sheng-ji Wang

TL;DR
This study examines how age affects the treatment and outcomes of traumatic brain injury patients in a Chinese hospital, highlighting the need for tailored care for the elderly.
Contribution
The paper provides insights into the surgical management and outcomes of geriatric TBI patients in a medium-developed Chinese city.
Findings
Elderly TBI patients had higher comorbidity rates and different injury causes compared to younger patients.
Elderly patients required more mechanical ventilation but fewer decompressive craniectomies and had higher disability rates.
Age significantly impacts clinical presentation and outcomes, emphasizing the need for age-specific care strategies.
Abstract
Traumatic brain injury (TBI) is a leading cause of morbidity and mortality worldwide, with outcomes influenced by age and comorbidities. This study aimed to compare the clinical characteristics, surgical management, and outcomes of elderly and younger TBI patients. Between 2017 and 2022, 1,260 TBI patients admitted to our hospital were included and categorized into younger (18–59 years) and elderly (≥60 years) groups. Demographic data, injury mechanisms, types of brain trauma, surgical interventions, and discharge outcomes were analyzed. Elderly patients had higher rates of comorbidities, with traffic accidents as the leading cause of injury and falls predominating in those aged ≥75 years. They showed a higher proportion of subdural hemorrhages, higher preoperative GCS scores, and required more mechanical ventilation and tracheostomy but underwent fewer decompressive craniectomies.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
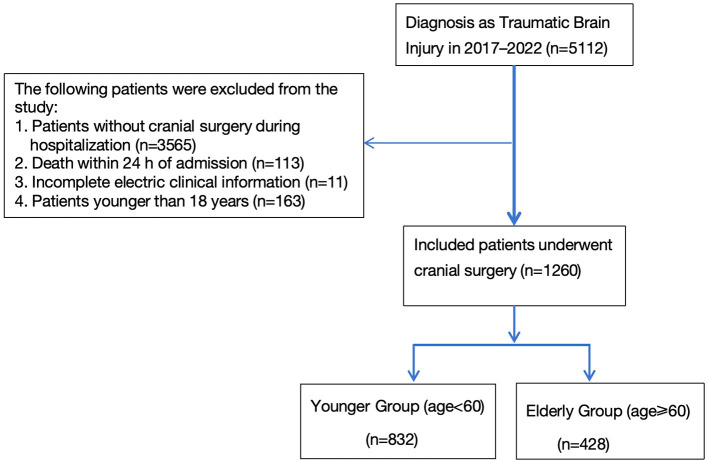 Figure 1
Figure 1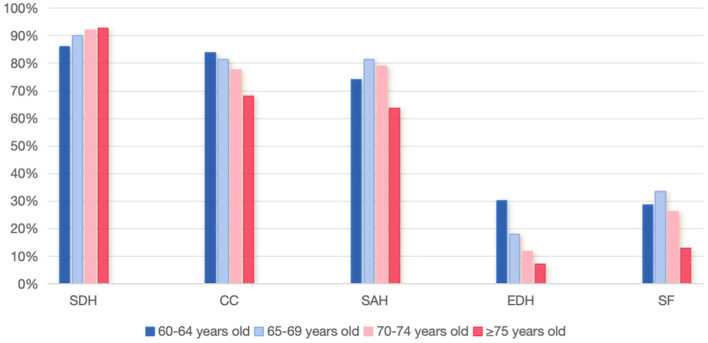 Figure 2
Figure 2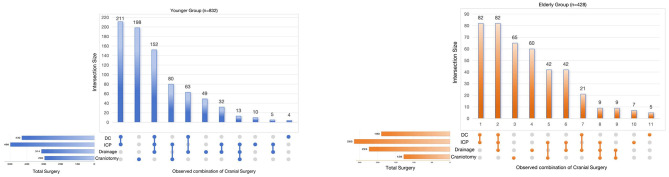 Figure 3
Figure 3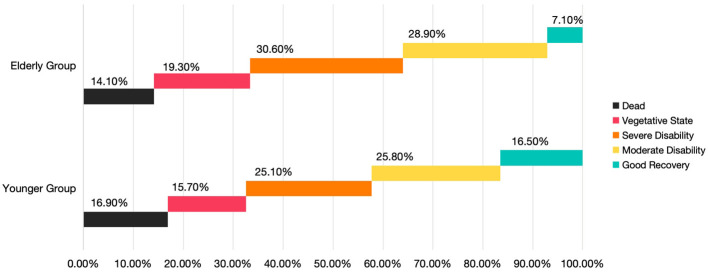 Figure 4
Figure 4|
|
|
|
|
|---|---|---|---|
| Gender (male), | 643 (77.3) | 304 (71.0) | 0.015 |
| Diabetes, | 37 (4.4) | 42 (9.8) | < 0.001 |
| Hypertension, | 71 (8.5) | 95 (22.2) | < 0.001 |
| Cerebral stroke, | 13 (1.6) | 16 (3.7) | 0.015 |
| Aetiology, | < 0.001 | ||
| Road traffic injuries | 367 (44.1) | 237 (55.4) | |
| Fall | 410 (49.3) | 178 (41.6) | |
| Violence | 55 (6.6) | 13 (3.0) | |
| CC | 703 (84.5) | 340 (79.4) | 0.024 |
| SDH | 664 (79.8) | 383 (89.5) | < 0.001 |
| SAH | 656 (78.8) | 324 (75.7) | 0.203 |
| EDH | 415 (49.9) | 82 (19.2) | < 0.001 |
| SF | 352 (42.3) | 110 (25.7) | < 0.001 |
| Traumatic epilepsy, | 38 (4.6) | 23 (5.4) | 0.528 |
| Preoperation GCS | 6 (5.9) | 8 (6.10) | 0.012 |
| Cerebral herniation, | 157 (18.9) | 73 (17.1) | 0.43 |
| Systemic hypotension, | 45 (5.4) | 31 (7.2) | 0.063 |
| Hypoxia, | 106 (12.7) | 68 (15.9) | 0.034 |
| Cardiopulmonary resuscitation, | 14 (1.7) | 14 (3.3) | 0.07 |
| Chest | 257 (30.9) | 141 (32.9) | 0.457 |
| Abdomen | 14 (1.7) | 7 (1.6) | 0.951 |
| Limbs | 50 (6.0) | 18 (4.2) | 0.18 |
| Spine | 115 (13.8) | 58 (13.6) | 0.895 |
| DC | 430 (51.7) | 190 (44.4) | 0.014 |
| ICP monitoring | 498 (59.9) | 265 (61.9) | 0.479 |
| Cranial trephination and drainage | 314 (37.7) | 224 (52.3) | < 0.001 |
| Craniotomy | 295 (35.5) | 128 (29.9) | 0.059 |
| Skull fracture repair surgery | 217 (26.1) | 67 (15.7) | < 0.001 |
| Unplanned second surgery | 52 (6.2) | 26 (6.1) | 0.521 |
| Ventilator, | 27 (3.2) | 26 (6.1) | 0.035 |
| Tracheotomy, | 30 (3.6) | 30 (7.0) | 0.007 |
| Hospital stay, days | 29 (25,30) | 28 (24.29) | 0.874 |
| In-hospital mortality, | 141 (16.9) | 60 (14.1) | 0.039 |
| Medical care fees | 62,880.840 (38,078.943, 84,775.105) | 59,431.845 (38,574.280, 66,840.705) | 0.71 |
| Medicine expenses | 47,278.685 (27,691.293, 59,220.273) | 41,976.510 (28,653.140, 57,743.735) | 0.339 |
| Surgery fee | 28,546.155 (21,586.573, 37,982.695) | 26,850.605 (16,165.480, 35,694.715) | < 0.001 |
| Cost of anti-infective drugs | 6,024.095 (2,556.635, 12,578.475) | 6,556.570 (2,152.333, 102,77.755) | 0.744 |
|
|
|
|
|
|
|
|---|---|---|---|---|---|
| Road traffic injuries | 73 (51) | 83 (59.3) | 48 (63.2) | 33 (47.8) | 0.292 |
| Fall | 63 (44.1) | 54 (38.6) | 27 (35.5) | 34 (49.3) | |
| Violence | 7 (4.9) | 3 (2.1) | 1 (1.3) | 2 (2.9) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Traumatic Brain Injury Research · Trauma and Emergency Care Studies
Introduction
Traumatic brain injury (TBI) is induced by external mechanical forces, including direct impact, rapid acceleration–deceleration, or penetrating head injury, and represents a major global health concern (1). According to a global epidemiological study conducted in 2016, the annual incidence and prevalence of traumatic brain injury (TBI) in the United States were 333 and 605 per 100,000 population, respectively. In China, the corresponding figures were 313 and 742 per 100,000 population, highlighting the substantial burden of TBI in both countries (2). Moreover, due to its large population, the absolute number of TBI cases in China surpasses that of most other countries, resulting in a considerable social and familial burden (3).
Globally, population aging further amplifies this challenge. In 2019, the number of people aged 60 years or older reached one billion, and this figure is projected to rise to 1.4 billion by 2030 and 2.1 billion by 2050 (4). This unprecedented demographic transition, particularly pronounced in developing countries, is expected to be accompanied by a marked increase in injuries and injury-related mortality among the elderly.
At present, research on neurosurgical approaches and prognostic outcomes in elderly patients with TBI remains limited, particularly in developing regions (5). There is an urgent need for further investigations in this underexplored yet rapidly expanding demographic to guide clinical practice and ensure adequate healthcare resource allocation.
Linyi People's Hospital, a Class A tertiary care center in Shandong Province, functions as the primary neurosurgical referral institution for Linyi, the largest developing city in the province, with a population of more than 11 million (6). Against this backdrop, we designed a retrospective study to evaluate the clinical characteristics, surgical interventions, and in-hospital outcomes of elderly patients undergoing neurosurgical treatment for TBI at our institution in recent years.
Methods
Study material
The present study was a retrospective analysis of patients with acute traumatic brain injury (TBI) who underwent neurosurgical treatment at Linyi People's Hospital between 2017 and 2022. Eligible patients were those consecutively admitted within 24 h of injury, aged 18 years or older, with cerebral computed tomography (CT) demonstrating intracranial signs of trauma. Clinical data were extracted from the hospital's electronic medical records and included demographic variables (age, sex), injury-related factors (cause of injury, associated injuries), medical history (comorbidities, prior conditions), preoperative neurological status [Glasgow Coma Scale (GCS) score], treatment details, and outcomes assessed by the Glasgow Outcome Scale (GOS) at discharge.
Inclusion criteria: Patients who underwent neurosurgical treatment during hospitalization, including decompressive craniectomy (DC), craniotomy, skull burr holes/cranial trephination and drainage, intracranial pressure (ICP) catheter implantation, and skull fracture repair.
Exclusion criteria: (1) Patients who did not undergo cranial surgery during hospitalization; (2) Patients who died within 24 h of admission; (3) Patients younger than 18 years; (4) Patients with incomplete electronic clinical information.
In this study, ICP monitoring catheters included both intraventricular and intraparenchymal devices. Cranial trephination and drainage included external ventricular drainage (EVD) and evacuation/drainage of intracranial hematomas. Drainage catheters can be placed epidurally, subdurally, within a hematoma, or intraventricularly. Skull fracture repair procedures included reduction of skull fracture, cranioplasty, elevation and debridement, dural repair, and fixation.
Statistical analysis
The distribution of variables was assessed using the Kolmogorov–Smirnov test. Continuous variables that did not follow a normal distribution were analyzed using the Mann–Whitney U test and presented as medians with interquartile ranges (IQR). Categorical variables were expressed as absolute numbers and percentages, and comparisons were made using the χ^2^ test when no inherent order was present. A p-value of < 0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA).
Results
As shown in Figure 1, from 2017 to 2022, a total of 5,112 TBI patients were admitted to our hospital. After applying exclusion criteria, 1,260 patients were included in the analysis. Patients were divided into two age groups: the Younger Group (18 ≤ age < 60) and the Elderly Group (age ≥ 60). Glasgow Outcome Scale (GOS) scores at discharge were recorded for all patients. Demographic characteristics and clinical management for the two groups are summarized in Table 1. Compared with younger patients, the elderly group had a lower proportion of male patients but a significantly higher prevalence of diabetes, hypertension, and prior stroke.
Patient inclusion and exclusion flowchart.
Traffic accidents were the leading cause of injury in the elderly group (55.4%), followed by falls (41.6%). To further examine injury mechanisms, the elderly group was subdivided into four age subgroups, as shown in Table 2. Notably, falls were the primary cause of injury only in patients aged 75 years or older.
Regarding the types of brain trauma, the elderly group exhibited lower rates of brain contusions, epidural hematomas, and skull/skull base fractures, but a higher proportion of subdural hemorrhages compared with the younger group (Table 1). The comparison of traumatic brain injury types among different age groups is presented in Figure 2. Preoperatively, elderly patients had higher median GCS scores (median 8). No significant differences were observed between the groups in rates of brain herniation or post-traumatic epilepsy. However, the elderly group had higher rates of hypoxemia (15.9 vs. 12.7%) and mechanical ventilation (6.1 vs. 3.2%). Rates of cardiopulmonary resuscitation and hypotension were also higher in the elderly group, though these differences were not statistically significant.
Comparison of brain trauma types in different age groups.
There were no significant differences in concomitant injuries between the two groups. Regarding surgical management, the elderly group had lower rates of decompressive craniectomy (DC) and skull fracture repair procedures (44.4 vs. 51.7%; 15.7 vs. 26.1%) but a higher rate of cranial trephination and drainage (52.3 vs. 37.7%), with statistically significant differences. No significant differences were observed in ICP monitoring, craniotomy, or unplanned secondary surgeries.
In-hospital mortality was lower in the elderly group than in the younger group (14.1 vs. 16.9%), whereas the rate of tracheostomy was higher (7 vs. 3.6%). Length of hospital stay was similar between the groups. Surgical costs were lower in the elderly group, while other hospitalization costs (including medical care, medications, and anti-infective drugs) were comparable.
Surgical approaches were tailored to patient conditions, such as DC combined with ICP catheter implantation or DC combined with cranial trephination and drainage. The comparative surgical characteristics between the two groups are shown in Figure 3.
Selection and combination of cranial surgery types in the two groups. UpSet plots were used to display cranial surgery types. Four primary cranial surgery types about TBI lesion (DC decompressive craniectomy; ICP, intracranial pressure monitoring; Drainage, cranial trephination and drainage; craniotomy).
Prognostic comparisons based on discharge GOS scores are shown in Figure 4. The elderly group exhibited lower mortality and complete recovery rates than the younger group, whereas the proportion of patients in a vegetative state or with moderate-to-severe disability was higher in the elderly group.
Comparison of percentage of patients between the two groups based on GOS class at hospital discharge.
Discussion
Our study analyzed the demographic characteristics, surgical approaches, and prognostic outcomes of elderly patients with acute TBI who underwent neurosurgical intervention. We found that elderly patients were more likely to receive minimally invasive procedures of shorter duration. Although their short-term mortality rate was lower, these patients exhibited a higher likelihood of moderate to severe postoperative disability, necessitating intensive care and prolonged rehabilitation. These findings provide real-world, evidence-based insights to inform future management strategies for elderly patients with TBI.
In our cohort, the main reason for injury among elderly patients was road traffic accidents. By contrast, a study conducted in the United Kingdom by Kehoe et al. (7) reported that more than 80% of elderly patients (≥65 years) sustained TBIs as a result of falls. Similarly, a large epidemiological survey in China indicated that incidental falls (n = 1,044, 43.23%) were the leading cause of TBI in old patients (8). These observations highlight a distinct difference in the predominant mechanisms of injury between developed and developing regions, underscoring the need for region-specific prevention and intervention strategies.
In this study, the incidence of subduralhemorrhage among elderly TBI patients increased with advancing age. This high frequency is thought to be related to age-associated brain atrophy, which enlarges the subdural space and predisposes elderly individuals to such lesions (9).
Elderly individuals frequently present with preexisting conditions such as hypertension and diabetes, making them more vulnerable to post-TBI complications including asphyxia, hypoxia, and shock. It is well-recognized that aging reduces physiological reserve, and the presence of comorbidities—as well as their ongoing treatments—can significantly influence the disease course and clinical outcomes (10). Moreover, the management of blood pressure in elderly hypertensive patients following TBI remains a subject of debate (11, 12). In particular, the optimal systolic blood pressure (SBP) threshold has recently been questioned, especially in developing countries where advanced monitoring tools such as intracranial perfusion pressure and cerebral blood flow measurements are not routinely available (13).
In our study, elderly patients underwent fewer decompressive craniectomies (DC) and craniotomies compared with younger patients. For this population, surgeons appeared to favor shorter, less invasive procedures aimed at rapidly alleviating life-threatening conditions. These findings reflect current trends in surgical decision-making. DC is generally considered a life-saving intervention for TBI patients with pronounced intracranial mass effect and refractory intracranial hypertension (14, 15). However, evidence regarding its long-term benefit remains mixed. In the CENTER-TBI study, comparative effectiveness analyses in patients with acute subdural hematoma demonstrated that institutional preference for an early surgical strategy, compared with initial conservative management, was not significantly associated with improved outcomes (OR 0.92, 95% CI: 0.77–1.09) (16). Similarly, results from the TRACK-TBI trials reported unfavorable long-term neurological outcomes in patients undergoing DC (17).
In addition, the indications for DC in geriatric patients remain undefined. In cases of epidural hematoma (EDH), emergency trephination—creating a small burr hole in the skull—can serve as a life-saving measure by providing temporary decompression of the hematoma (18, 19). Craniotomy remains the standard treatment for acute subdural hematoma (SDH), and placement of a subdural drain postoperatively facilitates removal of residual blood or cerebrospinal fluid (CSF), thereby preventing dangerous elevations in intracranial pressure (20). For selected SDH patients, particularly elderly individuals or those with unstable vital signs, preoperative trephination and drainage performed in the emergency setting may help reduce intracranial pressure, shorten operative duration, and ultimately decrease mortality (17, 21).
In current craniocerebral trauma surgery, ICP monitoring is often initiated first. Guided by ICP readings, elevated intracranial pressure can be gradually and controlledly reduced. Consequently, the incidence of acute encephalocele and contralateral delayed epidural hematoma in patients undergoing stepwise decompression is significantly lower than in those receiving conventional decompression (22). Moreover, this controlled decompression approach can also reduce the rates of vegetative state and 6-month postoperative mortality (23).
Beyond the increasing adoption of ICP monitoring, clinicians are employing more precise techniques to optimize the placement of external ventricular drain (EVD) tubes (24, 25). Minimally invasive strategies are also gaining traction; for instance, initiating a needle craniotomy for extradural hematoma using an EZ-IO device is feasible, allowing more rapid relief of intracranial pressure and providing additional time for definitive neurosurgical intervention (26). According to the Monro-Kellie doctrine, fluid removal decreases intracranial pressure, thereby improving cerebral perfusion and facilitating the delivery of osmotic agents, further supporting medical resuscitation efforts (27).
In the analysis of surgical characteristics, a higher proportion of elderly patients underwent cranial trephination and drainage, with or without ICP catheter implantation. Although a detailed subgroup analysis has not yet been performed, there is reason to believe that minimally invasive surgery may be more appropriate for elderly patients under close ICP monitoring. First, due to age-related brain atrophy, elderly patients generally have greater tolerance to intracranial hypertension and cerebral edema, and the need for decompressive craniectomy (DC) is therefore less urgent than in younger individuals. Second, elderly patients often present with multiple comorbidities, and the surgical trauma and physiological stress associated with conventional craniotomy may exacerbate their pre-existing conditions. Shen et al. (28) reported that patients aged ≥75 years had poor prognoses following traditional surgical interventions.
Wong et al. (29) prospectively collected data on consecutive trauma patients between 2001 and 2008 and demonstrated that advancing age was an unfavorable prognostic factor among patients with multiple trauma requiring neurosurgical intervention. In contrast, Lau et al. (30) prospectively enrolled consecutive patients with head trauma from 2006 to 2009 and found no statistically significant differences between age groups in 30-day mortality or recovery to baseline functional status. In the present study, which included patients admitted between 2017 and 2022, the relatively low in-hospital mortality observed among elderly patients with TBI may be explained by the increasing adoption of ICP monitoring and advanced life-support techniques, including mechanical ventilation. These advances have enabled elderly patients to better withstand the acute critical phase following injury (31).
The results of this study also indicate a higher prevalence of elderly TBI patients in a vegetative state or with severe disability, which aligns with findings from previous studies. While aggressive intensive care unit (ICU) management can improve survival in geriatric TBI patients, it is associated with an increased likelihood of discharge with severe disability (32). Elderly patients often require longer hospital stays, more home health services, and additional support during the first year post-injury (8, 33). In real-world settings, the rehabilitation and care of patients with severe disabilities or vegetative states present substantial challenges. Researchers such as Sveen et al. (34) have recommended a stronger clinical focus on older TBI patients, emphasizing the importance of continuity of care.
Several limitations should be acknowledged. First, potential selection bias may exist due to the relatively small sample size and the single-center study design. Second, the long-term prognosis of elderly patients with TBI was not evaluated. In addition, this study lacks further in-depth analyses, including the assessment of the strengths and limitations of different surgical techniques, the incorporation of the time interval between injury and surgery, and the evaluation of risk factors among patients who developed a vegetative state or severe disability. These aspects warrant further investigation.
In future research, we plan to compare patients with similar injury locations and hemorrhage types who undergo different surgical procedures, incorporate the precise interval between injury and surgery, and perform long-term follow-up to obtain a more comprehensive understanding and generate more robust conclusions. For elderly patients, future outcomes should emphasize not only survival but also changes in quality of life, which may serve as an indirect indicator of the effectiveness of local rehabilitation systems.
In summary, our study found that the in-hospital mortality rate of elderly patients with TBI decreased after surgical treatment, but there were still many patients with severe disability and vegetative state. We concluded that minimally invasive surgical procedures (such as cranial trephination and drainage) and life-support interventions (including mechanical ventilation) are crucial measures for reducing in-hospital mortality among patients with TBI. However, severe disability and a vegetative state remain conditions that require intensive care and long-term rehabilitation. For this specific patient population, greater efforts are needed to minimize disability and promote postoperative neurological recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Keelan RE Mahoney EJ Sherer M Hart T Giacino J Bodien YG . Neuropsychological characteristics of the confusional state following traumatic brain injury. J Int Neuropsychol Soc. (2019) 25:302–13. doi: 10.1017/S 135561771800115730681046 · doi ↗ · pubmed ↗
- 2GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:56–87. doi: 10.1016/S 1474-4422(21)00383-530497965 PMC 6291456 · doi ↗ · pubmed ↗
- 3Jiang JY Gao GY Feng JF Mao Q Chen LG Yang XF . Traumatic brain injury in China. Lancet Neurol. (2019) 18:286–95. doi: 10.1016/S 1474-4422(18)30469-130784557 · doi ↗ · pubmed ↗
- 4The World Health Organization (WHO). Ageing. Available online at: http://www.who.int/health-topics/ageing#tab=tab_1 (Accessed August 5, 2025).
- 5Hume CH Wright BJ Kinsella GJ. Systematic review and meta-analysis of outcome after mild traumatic brain injury in older people. J Int Neuropsychol Soc. (2022) 28:736–55. doi: 10.1017/S 135561772100079534313210 · doi ↗ · pubmed ↗
- 6Wang SJ Cheng ZX Fan XT Lian YG. Development of an optimized risk score to predict short-term death among acute myocardial infarction patients in rural China. Clin Cardiol. (2021) 44:699–707. doi: 10.1002/clc.2359833764508 PMC 8119840 · doi ↗ · pubmed ↗
- 7Kehoe A Smith JE Bouamra O Edwards A Yates D. Older patients with traumatic brain injury present with a higher GCS score than younger patients for a given severity of injury. Emerg Med J. (2016) 33:381–5. doi: 10.1136/emermed-2015-20518026825613 · doi ↗ · pubmed ↗
- 8Yang C Lang L He Z Hui J Jiang J Gao G . Epidemiological characteristics of older patients with traumatic brain injury in China. J Neurotrauma. (2022) 39:850–9. doi: 10.1089/neu.2021.027535171687 · doi ↗ · pubmed ↗