Resistance to imatinib in a ETV6::PDGFRB rearranged myeloid/lymphoid neoplasm with high-risk mutations: a case report
Lucia Cavelier, Leonie Saft, Birgitta Sander, Stefan Deneberg

TL;DR
A patient with a rare blood cancer involving a PDGFRB gene rearrangement developed resistance to imatinib and other treatments, highlighting the need for early molecular testing and stronger therapies.
Contribution
This case report documents resistance to TKI therapy in a PDGFRB-rearranged neoplasm with co-occurring high-risk mutations, emphasizing the need for alternative treatment strategies.
Findings
The patient showed initial response to imatinib but developed resistance despite dose escalation.
High-risk mutations in ASXL1, KRAS, NRAS, SETBP1, and SRSF2 were identified, contributing to poor prognosis.
The patient progressed to AML and died from sepsis despite additional therapies.
Abstract
Platelet-derived growth factor receptor beta (PDGFRB)-rearranged myeloid/lymphoid neoplasms (MLNs) are rare hematologic malignancies typically responsive to tyrosine kinase inhibitors (TKIs) such as imatinib. However, resistance—particularly in the context of co-occurring high-risk mutations—is uncommon and poorly characterized. We report a case of a 65-year-old man diagnosed with a ETV6::PDGFRB-translocated MLN, presenting as atypical chronic myeloid leukemia (aCML), who exhibited a brief response with development of resistance to imatinib. Although the patient initially achieved hematologic and partial cytogenetic remission, residual fibrosis and cytogenetic abnormalities persisted despite dose escalation. Molecular profiling revealed high-risk mutations in ASXL1, KRAS, NRAS, SETBP1, and SRSF2, along with a variant of uncertain significance (VUS) in IDH2. The patient progressed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
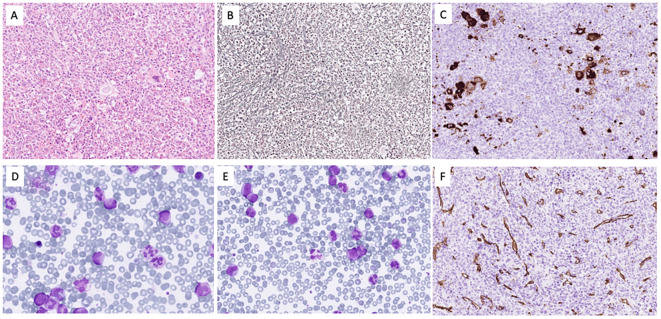 Figure 1
Figure 1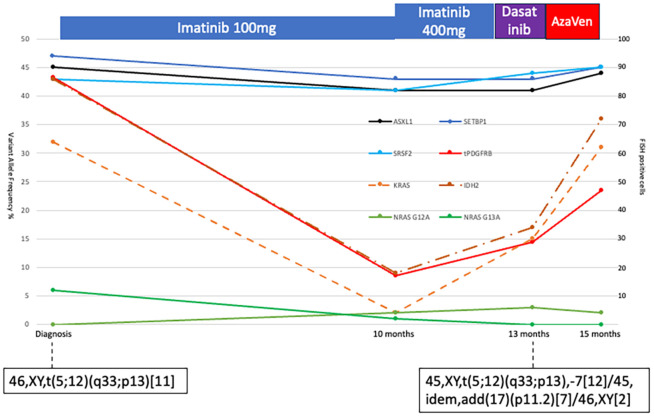 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Chronic Myeloid Leukemia Treatments · Acute Myeloid Leukemia Research
Introduction
Platelet-derived growth factor receptors alpha (PDGFRα) and beta (PDGFRß) are members of the class III receptor tyrosine kinase family, playing central roles in cellular growth, differentiation, and proliferation (1). Myeloid/lymphoid neoplasms with eosinophilia and PDGFRB rearrangements typically present as chronic myeloid neoplasms and are classified as a distinct entity in the World Health Organization (WHO) classification. The ETV6 gene is the most common fusion partner (2).
These rearrangements result in constitutive tyrosine kinase activation, rendering most cases highly sensitive to imatinib (3, 4). Over 40 different fusion partners have been reported, with ETV6 being the most frequent (5).
Patients with PDGFRB translocations may lack eosinophilia, only low grade in this case, and rarely present with additional cytogenetic or molecular abnormalities (4, 6–8).
Although most cases respond well to TKIs, resistance—either primary or acquired—remains poorly understood. Proposed mechanisms include secondary kinase domain mutations or disease progression to AML (9). TKI resistance has also been described in lymphoid malignancies with PDGFRB rearrangements (10, 11), though B-cell acute lymphatic leukemia with such fusions appears highly TKI-sensitive (12).
Here we describe a patient with a ETV6::PDGFRB translocation presenting as aCML, developing resistance to imatinib. The presence of high-risk mutations likely contributed to the resistance and rapid progression to AML. This case emphasizes the need for comprehensive molecular profiling, clonal monitoring, and early consideration of allogeneic stem cell transplantation in MLN cases with PDGFRB rearrangements that do not respond as expected to treatment.
Case description
A 65-year-old man with a history of prostate cancer treated by radical prostatectomy 12 years prior, without adjuvant therapy, presented with splenomegaly (12 cm below the left costal margin), 8-kg weight loss over 2 months, and gout. Laboratory studies revealed leukocytosis (69 × 10^9^/L), mild peripheral eosinophilia (2%), and mild anemia. Bone marrow biopsy showed hypercellularity with myeloid proliferation, dysgranulopoiesis, and grade 2 fibrosis, without increased blasts or significant eosinophilia (Figure 1). Cytogenetics revealed t(5;12)(q33;p13) as the sole abnormality. Fluorescence in situ hybridization (FISH) examination confirmed PDGFRB rearrangement. RNA sequencing confirmed the presence of an ETV6::PDGFRB fusion transcript involving exon 4 of ETV6 (NM_001987.5) and exon 9 of PDGFRB (NM_002609.4). Accordingly, whole genome sequencing identified the translocation breakpoint within intron 4 of ETV6 (NM_001987.5) and intron 8 of PDGFRB (NM_001355017.2). BCR::ABL1 was negative. Targeted sequencing revealed pathogenic mutations in ASXL1, KRAS, NRAS, SETBP1, SRSF2, and a VUS in IDH2 (13).
The bone marrow was hypercellular for age due to expansion of the granulocytopoiesis (A) with fibrosis grade II (B) and clusters of small megakaryocytes with monolobated nuclei (C). In the bone marrow smears (D), the M/E ratio was 8.3 with 1.8% blasts, 3% promyelocytes, and 22.6% myelocytes/metamyelocytes. The eosinophils were 1.6% and the monocytes 4%. In blood (E), blasts constituted 1.5%, promyelocytes 3%, and myelocytes/metamyelocytes 14%. CD34 staining (F) showed no increase in blasts.
Imatinib at 100 mg/day was initiated. Hematologic remission and spleen size normalization occurred within 2 months. However, at 10 months, a follow-up marrow showed only partial response, persistent patchy fibrosis, and 17% FISH positivity for the PDGFRB rearrangement. Imatinib was escalated to 400 mg/day, and transplantation workup was initiated.
Repeat marrow and FISH at 3 months later showed no further cytogenetic improvement and no blast increase. PDGFRB kinase domain sequencing showed no secondary mutations. Dasatinib at 100 mg/day was briefly trialed, but increasing leukocytosis necessitated azacitidine plus venetoclax. Despite therapy, the patient progressed to AML 15 months after diagnosis and died of sepsis with multiorgan failure during a neutropenic episode.
Serial sampling using the same targeted sequencing panel (13) in parallel with FISH for PDGFRB-rearrangement showed a decrease in PDGFRB-rearranged clone burden and parallel decreases in KRAS/NRAS variant allele frequency (VAF) (see Figure 2). In contrast, ASXL1, SETBP1, and SRSF2 VAFs remained stable. Interestingly, the IDH2 VUS VAF declined with the PDGFRB clone, suggesting that the variant was part of that clone. The two NRAS variants were consistently detected at low VAFs. Cytogenetics at AML transformation revealed monosomy 7 in 19/21 metaphases and a 17p11.2 locus loss in seven metaphases, alongside the persistent t(5;12), indicating clonal evolution. No TP53 mutations or new molecular abnormalities were found (Figure 2).
Diagram of bone marrow allele frequencies of ASXL1, SETBP1, SRSF2, KRAS, two NRAS, and IDH2 variants at different time points (scale on the left vertical). The PDGFB-translocation was measured with FISH at the same timepoints. A total of 200 cells were assessed, and the number of PDGFB-translocation-positive cells is plotted in the figure (red solid line, scale on the right vertical). Treatment is indicated above the diagram. Cytogenetic analyses were performed twice, and the results are indicated in the figure.
Discussion
Chronic-phase PDGFRB-rearranged neoplasms are typically sensitive to TKIs such as imatinib. Resistance is rare. Byrgazov et al. reported one imatinib-resistant NDEL1::PDGFRB case with a D850E mutation in the activation loop—a mechanism excluded in our case (9). Other reports describe TKI resistance predominantly in advanced-stage AML or lymphoid malignancies (7, 10, 11).
PDGFRB translocation alone appears to be a leukemogenic driver (14), explaining the usual absence of additional mutations or cytogenetic anomalies—similar to BCR::ABL1 in CML. Among the rare cases of TKI failure, few underwent molecular profiling (15, 16), and no previously identified mutations have been clearly linked to resistance (7, 17).
An exception is a case by Gou et al., who described an ETV6::PDGFRB-positive patient with concurrent NPM1, TET2, and NOTCH3 mutations and 46,XY,del(12)(p13p11.2), who developed a PDGFR-translocation positive T-lymphoblastic lymphoma while on imatinib (10).
In our case, ASXL1, SETBP1, and SRSF2 VAFs remained unchanged during treatment, indicating their independence from the PDGFRB-positive clone. While ASXL1 and SRSF2 mutations may reflect age-related clonal hematopoiesis, SETBP1 is more strongly associated with secondary AML, CMML, and aCML—often co-occurring with ASXL1 and SRSF2 in those neoplasms (18, 19). Given the unusual clinical course with an initial partial response to TKI followed by TKI-insensitive relapse and progression to AML, it is difficult not to think that the co-occurring mutations, in some way, contributed to the dismal outcome, even if it is impossible to conclude this in a single observational study such as this.
This case report has certain limitations, particularly in terms of generalizability—for example, the possibility of a pre-existing myeloproliferative neoplasm (MPN) with adverse mutations preceding the acquisition of the PDGFRB rearrangement cannot be excluded. Therefore, these findings should be interpreted with caution and may serve as a basis for further investigation.
The key message is to consider broad mutational profiling—even in the presence of targetable lesions like PDGFRB rearrangements and especially if signs of poor treatment response occur. In cases with poor molecular risk, rapid TKI response should not be assumed. While similar concerns have been raised in CML (20), this is, to our knowledge, the first report of primary TKI resistance in chronic-phase PDGFRB-rearranged MLN associated with high-risk mutations and adverse outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guérit E Arts F Dachy G Boulouadnine B Demoulin JB . PDGF receptor mutations in human diseases. Cell Mol Life Sci. (2021) 78:3867–81. doi: 10.1007/s 00018-020-03753-y, PMID: 33449152 PMC 11072557 · doi ↗ · pubmed ↗
- 2Shomali W Gotlib J . World Health Organization and International Consensus Classification of eosinophilic disorders: 2024 update on diagnosis, risk stratification, and management. Am J Hematol. (2024) 99:946–68. doi: 10.1002/ajh.27287, PMID: 38551368 · doi ↗ · pubmed ↗
- 3Apperley JF Gardembas M Melo JV Russell-Jones R Bain BJ Baxter EJ . Response to imatinib mesylate in patients with chronic myeloproliferative diseases with rearrangements of the platelet-derived growth factor receptor beta. N Engl J Med. (2002) 347:481–7. doi: 10.1056/NEJ Moa 020150, PMID: 12181402 · doi ↗ · pubmed ↗
- 4David M Cross NC Burgstaller S Chase A Curtis C Dang R . Durable responses to imatinib in patients with PDGFRB fusion gene-positive and BCR-ABL-negative chronic myeloproliferative disorders. Blood. (2007) 109:61–4. doi: 10.1182/blood-2006-05-024828, PMID: 16960151 · doi ↗ · pubmed ↗
- 5Saft L Kvasnicka HM Boudova L Gianelli U Lazzi S Rozman M . Myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase fusion genes: A workshop report with focus on novel entities and a literature review including paediatric cases. Histopathology. (2023) 83:829–49. doi: 10.1111/his.15021, PMID: 37551450 · doi ↗ · pubmed ↗
- 6Patnaik MM Lasho TL Finke CM Pardanani A Tefferi A . Targeted next generation sequencing of PDGFRB rearranged myeloid neoplasms with monocytosis. Am J Hematol. (2016) 91:E 12–4. doi: 10.1002/ajh.24267, PMID: 26662677 · doi ↗ · pubmed ↗
- 7Baer C Muehlbacher V Kern W Haferlach C Haferlach T . Molecular genetic characterization of myeloid/lymphoid neoplasms associated with eosinophilia and rearrangement of PDGFRA, PDGFRB, FGFR 1 or PCM 1-JAK 2. Haematologica. (2018) 103:e 348–e 50. doi: 10.3324/haematol.2017.187302, PMID: 29567772 PMC 6068021 · doi ↗ · pubmed ↗
- 8Metzgeroth G Steiner L Naumann N Lübke J Kreil S Fabarius A . Myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase gene fusions: reevaluation of the defining characteristics in a registry-based cohort. Leukemia. (2023) 37:1860–7. doi: 10.1038/s 41375-023-01958-1, PMID: 37454239 PMC 10457188 · doi ↗ · pubmed ↗