Reporting a Patient Safety Culture in Global Health: Evidence From Sierra Leone
Yanran Li, Ning Yang, Lu Niu, Joseph Benjamin Bangura, Mustapha Kabba, Dan Luo, Li Li, Xiang Chen

TL;DR
This study examines patient safety culture in Sierra Leone, highlighting key challenges and areas needing improvement.
Contribution
This is the first study on patient safety culture in Sierra Leone, revealing unique challenges in resource-limited settings.
Findings
Teamwork had the highest positive response rate (80.83%), while reporting patient safety events had the lowest (49.1%).
Staff working longer hours than ideal for patient care had a low positive response rate (18.09%).
Tenure in the unit significantly predicted patient safety events reported.
Abstract
To explore the level of patient safety culture in Sierra Leone and identify the factors associated with the patient safety grade and patient safety events reported. A cross-sectional study. From February to March 2024, we selected staff members from three representative public hospitals of different types in Sierra Leone. Patient safety culture was assessed with the Hospital patient safety culture survey 2.0. Binary logistic regression was employed to determine the influence of sociodemographic characteristics on the patient safety grade and patient safety events reported. The textual responses to the open-ended question were imported into Nvivo 12.0 for thematic analysis. A total of 247 questionnaires was sent out, of which 202 were effectively received. Among 10 safety culture dimensions, three were strength areas with over 75% positive response rate. The other six dimensions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
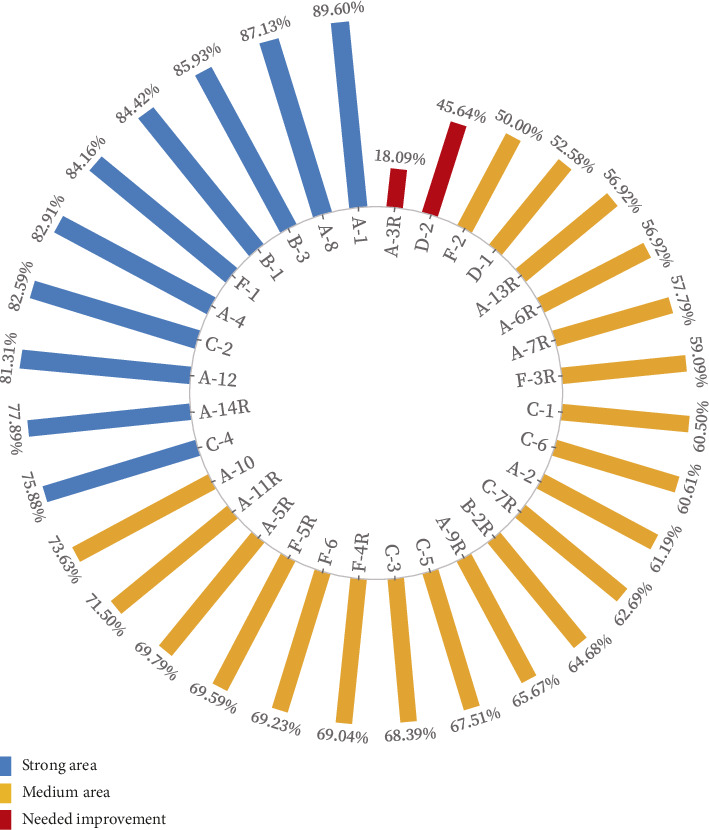 Figure 1
Figure 1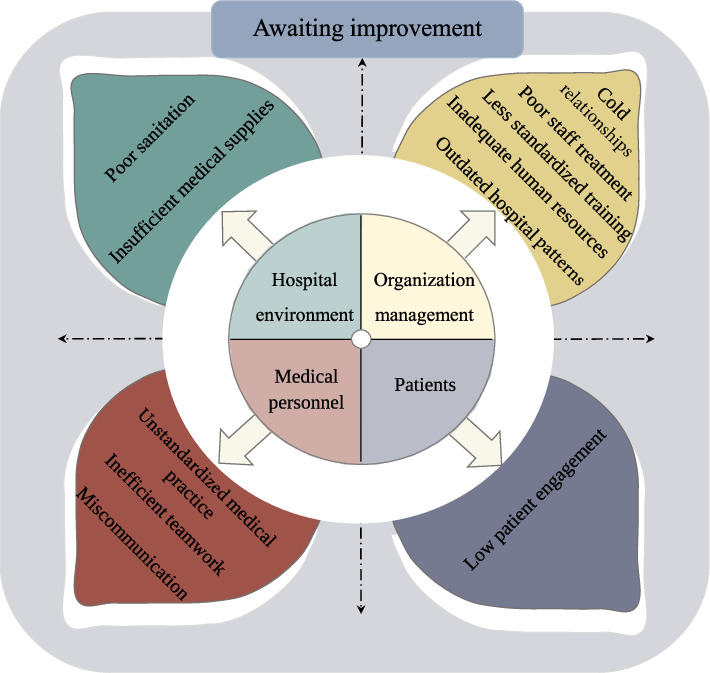 Figure 2
Figure 2- —CHINA MEDICAL BOARD
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient Safety and Medication Errors · Global Health and Surgery · Global Maternal and Child Health
Summary
- • What is already known about this topic?
- ◦ Economically underdeveloped regions are frequently associated with a higher prevalence of patient safety risks due to systemic healthcare disparities.
- ◦ Patient safety culture is internationally recognized as a fundamental component for enhancing patient safety and preventing adverse events.
- ◦ Patient safety culture research is shifting toward developing countries, yet evidence from least developed nations remains critically scarce.
- • What this paper adds?
- ◦ This first patient safety culture survey in Sierra Leone establishes foundational evidence to inform future research, clinical practice, and regional health protection.
- ◦ Patient safety culture in Sierra Leone falls below average, with “Reporting patient safety event” response positivity ranking lowest across all assessed metrics.
- ◦ Hospital staff in Sierra Leone most times work beyond safety thresholds, where fatigue and cognitive overload systematically undermine patient safety.
- ◦ Unique challenges in resource-limited settings were noticed (water/electricity/sanitation), addressing a critical gap in the global patient safety evidence base.
- • Patient or public contribution
- ◦ Nursing administrators from three public hospitals, in collaboration with the China-Africa medical aid team, actively facilitated questionnaire data collection by scheduling interview appointments and providing on-site survey venues.
- ◦ The participants were involved in the design, or conduct, or reporting, or dissemination plans of our research.
1. Introduction
At the latest International Nurses Congress (ICN), patient safety was placed at the top of the agenda, demonstrating its undisputed core priority. There is a significant amount of avoidable patient harm, no matter how advanced the healthcare system [1]. Research shows that 1/10 patients suffers harm during hospital treatment in high-income countries [1], and 13.4 million medical errors occur each year in low- and middle-income countries, resulting in 2.6 million unnecessary deaths [2]. These indirect costs of patient harm amounts to trillions of US dollars each year [3]. A retrospective cohort study shows that adverse events were identified in nearly one in four admissions, and approximately 22.7% events were preventable [4]. Early research efforts concentrated on understanding the extent and typology of human error, which were contributing to patient harm [5]. More recently, the focus of inquiry has shifted towards understanding the role played by human and organizational issues such as leadership, teamwork, and communication in contributing to, as well as preventing, adverse events [6].
Patient safety culture (PSC) was widely recognized as a crucial element in the improvement of patient safety and the prevention of adverse events in healthcare organizations [7, 8], which was sourced from safety culture [9]. Safety culture refers to the beliefs, values, perceptions, and attitudes of patient safety shared among members of the organization and that determined the commitment to, and the style and proficiency of, an organization's health and safety management [10]. PSC is conceptually complex and abstract, which needs interdisciplinary teamwork rather than personal performance and can be viewed within the PSC theoretical framework, which is made up of these components: (a) degree of psychological safety, (b) degree of organizational culture, (c) quality of culture of safety, (d) degree of high reliability organization, (e) degree of deference to expertise, and (f) extent of resilience [11].
Assessing PSC is essential to understand healthcare professionals' perceptions and guide effective interventions. The Hospital Survey on Patient Safety Culture (HSOPSC), developed by the Agency for Healthcare Research and Quality (AHRQ), is one of the most widely used instruments for this purpose in hospitals [12]. Research on PSC has been conducted in various countries to date. A multicenter survey of cancer nurses in four European countries demonstrated that the UK attained the highest patient safety score of 72.0 (17.8), followed by Estonia and the Netherlands, whilst Germany scored the lowest [13]. In a survey of 713 nurses and midwives in Austria, the average score for safety culture that these participants attained was 4.09 ± 0.53 [14]. As patient safety assumes a more prominent role on the global stage, there has been a concomitant shift from developed to developing countries. The mean score achieved by China in relation to its PSC was 72.5 ± 7.6 [15]. A comparative east–west study has revealed that Australian participants reported significantly lower patient safety ratings than their Chinese counterparts [16]. Different demographic characteristics (age, career, work hours, income, educational level, and so on) [17], hospital accreditation [18], work environment [19], interpersonal relationship [20], and communication [21] are all influences on PSC.
It is a matter of concern that PSC is inextricably linked to the regional economy. In some south-east Asian countries, patient safety policy and its application are not prioritized as much as they are in developed countries in the priority [22]. Capnography is universally accepted as an essential patient safety monitor in high-income countries yet is often unavailable in low- and middle-income countries [23]. It is a fundamental right of patients to have access to safe healthcare services, regardless of poverty or wealth. Protecting patient safety in resource-limited settings is an emerging challenge for global healthcare systems [24].
In 2019, AHRQ released a modified HSOPSC, Version 2.0 [25]. Importantly, AHRQ now encourages the use of Version 2.0, and data from the two versions are not directly comparable. Sierra Leone is in the western region of Africa and is one of the least developed countries. Over 60% of people die prematurely before the age of 70 in Sierra Leone, especially women and children, from preventable or treatable causes [26]. A qualitative study revealed a widespread negligence regarding aspects of PSC in African countries, including issues such as material deprivation [27]. There has been limited measurement of PSC in Sierra Leone in previous studies. Thus, this study proposes measuring the level of PSC in Sierra Leone using the latest Version 2.0 and identifying the factors associated with the patient safety grade and patient safety events reported. The findings will fill a gap in previous research and inform administrators and decision makers in promoting a culture of patient safety in Sierra Leone.
2. Methods
2.1. Participants and Settings
During the initial phase, we have selected 3 representative public hospitals in Sierra Leone by purposive sampling to evaluate the status quo of patient safety. Sierra Leone has few hospitals and relies on international assistance. The hospitals chosen are in Freetown and Makeni, where the Chinese, medical teams work. In Freetown, the capital of Sierra Leone, we selected two public hospitals, which also function as the two most heavily trafficked and representative hospitals. The city of Makeni is home to a single public hospital. Specific information is as follows:
-
- Connaught Hospital (principal hospital) (local): Connaught Hospital is Sierra Leone's principal and largest public adult referral hospital. It has staff capacity of 1200 of which 40 are medical doctors (MDs). It comprised of 26 different unites with different specializations, including surgical, radiology, physiotherapy, cancer, epilepsy, mental and psychosocial counseling, accident, and emergency.
-
- Sierra Leone–China Friendship Hospital (partnership hospital) (China). It is a partnership hospital. It is a 59-bed capacity hospital providing various services including maternity, surgical, medical, pediatrics, ENT, laboratory, endoscopy daz scan, and x-ray. It has staff strength of 179 of different categories including MDs, lab technicians, pharmacist, anesthetist, and radiographers.
-
- Makeni Regional Government Hospital (district and regional hospital) (local): The hospital is the only government referral hospital in Bombali district and the main referral hospital in the northern province. It has a 250-bed capacity, providing primary, secondary, and tertiary services. It comprised of the following technical units: OPDs general, accident and emergency, IPC, mental health, surgical, medical, maternity, pediatrics, SCBU, school health clinic, isolation, pharmaceutical, oral health department, laboratory, ANC, radiology, and ICU.
Finally, hospital staff were recruited from three representative public hospitals by convenience sampling, including physicians, nurses, technicians, administrators, and support staff from February to March 2024. The specific inclusion and exclusion criteria were as follows:
- • Inclusion criteria include (1) ≥ 18 years old; (2) participants were legally and formally employed by the respective hospitals; and (3) informed consent.
- • Exclusion criteria include (1) absence from work for 6 months or more due to participation in further training, maternity leave, and so on; and (2) unable to understand the questionnaire.
2.2. Sample Size Calculation
The minimal sample size was detected by applying a single proportion of the population formula (N = Zα/2^2^P(1 − P)/δ^2^) [28], setting α = 0.05, Zα/2 = 1.96, and δ = 0.1P. We determined the required sample size to be 173, using a 69% response rate derived from the 2022 SOPS Hospital 2.0 Database Report on trending hospitals [29]. Moreover, after adding 20% potential invalid responses, final requested sample size was 207.
2.3. Instrumentation
2.3.1. The HSOPSC (2.0 Version).
The HSOPSC 2.0 comprises 40 items, 32 of which are grouped into 10 dimensions which make up the concept of “PSC” [25]. These 32 items are measured on a five-point Likert scale for agreement (from “Strongly disagree” to “Strongly agree”) or frequency (“Never” to “Always”), plus a response option “Does not apply or Don't know.” The instrument also included two single-item outcome measurements, one relating to how often incidents were reported and the other asking respondents to give a patient safety rating in their unit/work area. The six remaining questions request participant data on job position, work unit, length of time working at the hospital and in the present unit/area, weekly hours worked, and whether in direct contact with patients. Percentage of positive responses for each item and dimension was calculated. Responses of “agree” or “strongly agree” and “always” or “most of the time” for the positively worded items indicated positive responses. Additionally, responses of “disagree” or “strongly disagree” and “never” or “rarely” for the negatively worded items indicated positive responses. Positive response rates were used to evaluate attitudes toward PSC in different dimensions. A positive response rate > 75% indicated a strong area of safety culture, while < 50% needed improvement.
Additionally, the survey contained an open-ended item for text entry (please feel free to provide any comments about how things are done or could be done in your hospital that might affect patient safety).
2.4. Data Collection
The study was approved and supported by the partner hospitals. As English is the official language of Sierra Leone, the survey was administered in English following an explanation of the purpose, significance, and consent requirements of the study to the hospital authorities and department heads by two members of the research team. Guided by local hospital staff, the research team visited various departments during working hours and invited all available and willing staff to participate in the study. The hospital staff also served as interpreters, as indigenous languages like Mende and Temne were commonly used alongside English. Prior to the survey, all potential participants were fully informed of the study's purpose, procedures, risks, and benefits. Written informed consent was obtained from each individual following a 1-h reflection period with the information sheet. Participants were assured of the voluntary nature of their participation, their right to withdraw at any time without penalty, and the confidentiality of their data. After obtaining informed consent from participants, questionnaires were distributed (paper version). Data collection was carried out by trained researchers from the long-term medical aid team in Sierra Leone. Participants freely chose private settings to complete the questionnaires, and researchers were available throughout to provide immediate clarification for any questions or points of confusion. The completed questionnaires were collected on the same day. All participants demonstrated strong comprehension of English throughout the process.
2.5. Data Analysis
Data were analyzed using the IBM Statistical Package for the Social Sciences (Statistics), Version 26.0. Descriptive statistics were estimated to characterize participants by position in this hospital/unit, tenure in hospital//unit, hours worked per week in hospital, and interaction with Patients. Categorical variables were presented as frequencies with percentages. All negatively worded items were reverse coded, and percentage of positive responses for each item and dimension was calculated. Binary logistic regression was employed to determine the influence of sociodemographic characteristics on the patient safety grade and patient safety events reported.
The textual responses from the open-ended question were analyzed using Nvivo 12.0. We conducted a thematic analysis of the responses. The coding process involved an initial review to generate common themes, which were then categorized and refined. After analyzing the suggestions from the first two hospitals, we observed that the responses were encompassed by the existing thematic framework. This consistency in themes was further confirmed by analyzing the responses from the third hospital. Throughout the analysis, we focused on identifying and reporting the themes most relevant to the research topic.
2.6. Ethical Approval
The Sierra Leone Ethics and Scientific Review Committee (SLESRC) conducted an expedited review of the above study. The study was conducted in compliance with the latest version of the Declaration of Helsinki. Confidentiality and informed consent were prioritized throughout the investigation. Participants had the option to withdraw from the study at any point with no impact on their work or welfare.
3. Results
3.1. Participant Characteristics
A total of 247 questionnaires were sent out, of which 202 were effectively received (43 incomplete and 2 invalid questionnaires), giving a response rate of 81.78%. Many of the respondents (58.41%) were nurses, 17.1% from medical/surgical units. Of the respondents, 46.03% had worked in the hospital for 1–5 years, while 27.12% worked for 6–10 years. Half of respondents (50.2%) worked 30–40 h a week. Additionally, 74.8% of respondents had direct contact with patients. See Table 1 for details.
3.2. The Positive Response Rate of HSOPSC
Table 2 shows among these 10 safety culture dimensions, three were strength areas with over 75% positive response rate. The other six dimensions ranged from 54.91% to 70.54%. There was one dimension with a positive response rate below 50%, indicating a need for improvement. In this study, the highest positive response rate dimension was “Teamwork” (80.83%) and the lowest was “Reporting patient safety event” (49.1%).
Among the scores of each item of hospital PSC, 10 items are in the strong area, 20 items are in the medium area, and only 2 items are in the needed improvement. Item A-1 (In this unit, we work together as an effective team) has the highest positive response rate, reaching 89.60%. Item A-3R (Staff in this unit work longer hours than is best for patient care) is a reverse item, with a positive response rate of 18.09%, ranking last among all items. Item D-2 (When a mistake reaches the patient and could have harmed the patient, but did not, how often is this reported?) has a positive response rate of 45.64%, only higher than item A-3R. See Figure 1 for details.
3.3. Patient Safety Grade and Patient Safety Events Reported
Table 2 shows the majority of participants showed a positive attitude towards their unit, with more than 1/4 rating the overall patient safety rating as excellent. However, in the past year, a whopping 17.33% of patients reported more than 11 patient safety incidents.
3.4. Binary Logistic Regression Analysis for Patient Safety Grade and Events Reported
We processed missing data and reclassified demographic variables into binary logistic regression models. Table 3 shows that “Tenure in Unit/Work Area” could effectively predict patient safety events reported. The probability of employees who had been employed for more than 5 years reporting patient safety events was 2.083 times that of employees who had been employed for less than 5 years, the differences are statistically significant (B = 1.13, p=0.02). All other results were not significant.
3.5. Awaiting Improvement
The text data came from the last item of the scale survey, and all answers that were clearly written were included in the study. A total of 143 participants filled out the suggestions, of which two phrases whose specific meanings could not be understood were excluded. The suggestions of the remaining 141 participants were included in the final study. Analysis of the open-ended responses revealed a thematic structure comprising four main themes: ① hospital environment aspects, ② organization management aspects, ③ medical personnel aspects, and ④ patients aspects, which branched into eleven subthemes (see Figure 2).
3.5.1. Theme 1: Hospital Environment Aspects
Sierra Leone's hospitals have poor conditions, improper disposal of medical waste, short basic water, electricity and lighting equipment, improper placement of items in the wards, inadequate cleaning, lacking air conditioning and internet, and other problems. The inadequate large quantities of medical supplies, such as ventilators, surgical consumables, masks, and medicines, have brought great challenges to health care services, and even the safety of medical staff themselves is difficult to guarantee.“Lack of medical equipment (2) Improper disposal of medical waste”“The hospital management should provide more or enough medical equipment for the hospital so that patients safety would be assured.eg. oxygen cylinder and more.”“There should be full PPE always…No wheelchair and bed sheets in the wards.”
3.5.2. Theme 2: Organization Management Aspects
At the organizational management level, the nonsatisfactory treatment of medical staff, the limited manpower, limited use of standardized operation guidelines, the outdated hospital model, and the indifferent colleague relationship have brought a series of hidden dangers to patient safety.“Lack of vital equipment and lack of nurses in the ward”“(1) Regular Conducting of training facilities for staff (2) Provision of equipment or consumable for continuity or for smooth running of the hospital (3) Conducting regular meetings with staff (4) Regular monitoring on staff (5) no medical for staff”“The hospital management should have a data Base System that help patient information in the hospital. That can put all the patient card number and time of visit or revisit.”
3.5.3. Theme 3: Medical Personnel Aspects
Poor communication between doctors and nurses will affect teamwork and make it difficult to ensure the safety of patients. In addition, nonstandard medical operations require enhanced awareness and behavioral improvement.“No proper hand washing”“We need to work as a team to improve the safety of our patient”“(5) Poor communication between doctors and nurses”
3.5.4. Theme 4: Patients Aspects
In this topic, little information is obtained, and patient supervision and self-care behaviors need to be added to future medical activities.“Engage patient in their care plan.”
4. Discussion
To the best of our knowledge, this is the first survey on patient safety conducted in Sierra Leone in full response to the call of the AHRQ. These data may facilitate future research and clinical practice related to PSC and safeguard the lives and health of the people in the region.
The overall average positive response rate was 67.62% in our study, which is similar to other low- and middle-income countries (e.g., Iran, 51.32%) and is in the middle of the range [30]. This result is clearly unsatisfactory. It is lower than in some upper-middle-income countries (e.g., Kazakhstan, 73.5%) [31]. “Reporting patient safety event” was the lowest contributing dimension for overall PSC. This means that in Sierra Leone, if a medical worker performs an incorrect medical procedure that does not cause harm to the patient, usually this was not reported. In the regression model, the longer the number of years of service is, the more likely workers were to report adverse events. Combining both, we speculate that there are two reasons: First of all, the reporting behavior of employees is discouraged by a punitive culture [32]. Adverse events trigger a reaction of criticism; younger workers fear this culture and avoid responsibility. The same situation existed in other countries in the past [33], but in recent years, the number of nurses reporting adverse events on their own initiative has gradually increased, thanks to a “nonblame,” communication, and incentives [34]. It is a signal that reporting systems should focus on patient outcomes and learning from systems issues, not blaming individuals. The second is due to irregular report norms, hospital administrators have not made it mandatory for reporting potential adverse events, so young worker do not have the awareness to report [35]. Additionally, even if there was an inclination to report, the irregular report norms would inevitably act as an obstacle. Spontaneous reporting behavior exists among senior staff, as they have more experience related to patient safety and are more aware of the safe practices and benefits of reporting within the hospital [36]. The mentorship is a potential solution to this issue [37]. In international medical assistance aspect, the mentor role (the state that offering relief) not only goes beyond medical tech and services provision but also sets international standards for management. In daily work aspects, the responsibility is shouldered by senior nurses, who are accustomed to providing guidance and support to novice personnel. Furthermore, peer mentoring program is being presented as a viable alternative in consideration of challenging situations [38].
Pay more attention to a phenomenon. Long working hours have become the norm for medical workers in Sierra Leone, which may induce work fatigue and is not conducive to patient safety [39]. Many countries define standard working hours as 35–40 h/week and working ≥ 41 h/week as overtime work [40]; however, about 44% of the participates were working overtime in our study. The shortage of nursing human resources is a common challenge for global health care systems [41]. Whilst other nations can incentivize the migration of nurses via generous remuneration, such expenditures are beyond the financial capacities of African states. The second reason pertains to the act of operating within full manual mode. So far, they lack an electronic database system (mentioned in qualitative information), which means that workers need to spend more time doing some manual and repetitive work. Electronic information systems can assist nurses in timely and standardized nursing operation, yet such systems remain scarce in most low-income countries [42]. There are also major flaws in nursing management. The grassroots nurses are not included in daily nursing management, which will result in nurses no longer feeling a sense of belonging to the hospital. A study revealed that less job embedding represents less innovative behaviors [43]. It is imperative to address the root causes of human resources and manpower management. The reliance on external financial support, such as bailouts, is not a viable long-term solution. The establishment of local medical colleges is a crucial initiative to ensure the effective and sustainable management of these resources. Concurrently, the active involvement and motivation of junior nurses in the management of hospitals may be expected to enhance work efficiency. In addition, in a short conversation with the staff of the hospital, we learned that the hospital would have “volunteers” to assist the regular work in their daily medical activities. In fact, people who do not have the appropriate qualifications are not qualified to practice medicine, which means that the operation of “volunteers” is also one of the risk factors for patient safety.
The analysis of open-ended question highlights a number of existing medical dilemmas, with worrying results. Poor infrastructure such as water, electricity, and lighting, as well as a lack of medical supplies, are the biggest threats to patient safety in Sierra Leone. Obviously, these reality dilemmas are unlikely to change in the short term and no longer a matter of staff awareness. The issue of how to allocate and justify the utilization of healthcare resources has assumed significance in the context of limited resources. Alongside this international assistance, many low- and middle-income countries have established an increasing number of public nongovernmental organization partnerships in the health sector as means of improving public health [44]. In recent years, the medical field has witnessed a paradigm shift towards digital technologies, which has been described as the “digital revolution.” Recent studies have demonstrated the efficacy of mobile health (mHealth) services in addressing issues of scarcity and inequitable distribution of healthcare resources [45]. Daniels noted in his study that the widespread use of geographic information systems for public health issues may be useful for global health outreach planning and resource allocation [46].
A common problem related to hand hygiene. “Unstandardized handwashing” or even “no handwashing” is a patient safety hazard. Standardized training is one way to maintain medical practices and ensure patient safety [47]. User-friendly designs can also promote handwashing; examples include scented hand sanitizers, slogans, dryers, and hand care products.
In summary, the PSC in Sierra Leone is not optimistic, and this requires the contribution and cooperation of various stakeholders. The findings of this study suggest that the state and healthcare organizations should be obliged to implement the following strategies: (1) tolerant workplace culture; (2) mentorship; (3) the establishment of local medical colleges; (4) staff participation in hospital decision-making to build an organizational culture; (5) nongovernmental collaborations; (6) mHealth technology; and (7) standardized training. These strategies are of paramount importance and have the potential to be widely implemented to ensure the delivery of quality care and patient safety.
5. Conclusions
It is acknowledged that this is the first research to be conducted in Sierra Leone about the local PSC. Hospital safety culture in Sierra Leone remains suboptimal overall, with adverse event reporting representing the most significant issue. Our study also uncovers unique patient safety challenges in resource-limited settings (reliable water and electricity supply, proper sanitation, and adequate staffing), addressing a critical gap in the global patient safety evidence base.
5.1. Limitation
First, a nonprobability sampling approach was employed, which inherently resulted in an unrepresentative sample due to the unequal representation of staff groups, thereby introducing systematic over-representation bias. Second, the questionnaires were self-reported by the participants and the question and answer of the questionnaire items were inaccurate due to factors such as social expectations and memory bias. Finally, due to the scarcity of healthcare resources in the region and the small number of public hospitals and staff, the scope of the survey and sample size need to be expanded in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO)Patient Safety [EB/OL]2023 https://www.who.int/news-room/fact-sheets/detail/patient-safety
- 2The LANCET Patient Safety: Too Little, but Not Too Late The Lancet 201939410202 p. 89510.1016/S 0140-6736(19)32080-X 2-s 2.0-8507197804531526719 · doi ↗ · pubmed ↗
- 3Slawomirski L. Klazinga N. The Economics of Patient Safety: From Analysis to Action [EB/OL]2020 http://www.oecd.org/health/health-systems/Economics-of-Patient-Safety-October-2020.pdf
- 4Bates D. W. Levine D. M. Salmasian H. The Safety of Inpatient Health Care New England Journal of Medicine 2023388214215310.1056/NEJ Msa 220611736630622 · doi ↗ · pubmed ↗
- 5Wears R. L. Sutcliffe K. M. Rite E. V. Patient Safety: A Brief but Spirited History (M)2016 https://www.taylorfrancis.com/chapters/edit/10.4324/9781315599700-2/patient-safety-brief-spirited-history-robert-wears-kathleen-sutcliffe-eric-van-rite?context=ub%26ref Id=f 83a 3cbe-a 91c-4cdb-9f 7a-c 4702 db 9c 814
- 6Lee W. Jang I. Effect of Nurses’ Professionalism, Work Environment, and Communication With Health Professionals on Patient Safety Culture (AHRQ 2.0.): A Cross-Sectional Multicenter Study Journal of Nursing Management 2023202311110.1155/2023/1591128 PMC 1191852340225614 · doi ↗ · pubmed ↗
- 7Wang S. J. Chang Y. C. Hu W. Y. Shih Y. H. Yang C. H. Improving Patient Safety Culture During the COVID-19 Pandemic in Taiwan Frontiers in Public Health 202210 p. 88987010.3389/fpubh.2022.889870 PMC 931529035903386 · doi ↗ · pubmed ↗
- 8Moreno-Leal P. Leal-Costa C. Díaz-Agea J. L. Castaño-Molina M. L. Á. Conesa-Ferrer M. B. De Souza-Oliveira A. C. Disruptive Behavior and Factors Associated With Patient Safety Climate: A Cross-Sectional Study of Nurses’ and Physicians’ Perceptions Journal of Nursing Management 20242024 p. 556839010.1155/2024/5568390 PMC 1191864740224803 · doi ↗ · pubmed ↗