Therapeutic Potential of Acalypha wilkesiana in Type 2 Diabetes: A Review
Samuel Inshutiyimana, Patel Dineshbhai Yesh, Michael Matiop Aleu, Aibekhanya Nkosana Sebata, Kenfa Ajumesi, Norhayati

TL;DR
This review explores how Acalypha wilkesiana, a medicinal plant, may help treat type 2 diabetes by lowering blood sugar and protecting organs.
Contribution
The paper provides a comprehensive review of Acalypha wilkesiana's antidiabetic potential and mechanisms, highlighting its potency and safety.
Findings
Ethanolic root bark extracts of Acalypha wilkesiana show greater α-glucosidase and α-amylase inhibition than acarbose.
The plant's leaves have no harmful effects on red blood cells and can restore pancreatic and spleen cell function in diabetic rabbits.
Acalypha wilkesiana shows promise as a safer and more effective antihyperglycemic agent compared to synthetic drugs.
Abstract
Type 2 diabetes mellitus (T2DM) refers to a chronic metabolic disorder that results from insulin resistance, leading to impaired insulin action and uncontrolled plasma glucose levels. Acalypha wilkesiana is among medicinal plants that are ethnobotanically used in the management of T2DM. However, there is a paucity of information on its antidiabetic potential. This review is aimed at providing a current understanding of the mechanism of action, potency, and safety of Acalypha wilkesiana in T2DM therapy. A narrative review was thoroughly conducted by searching Google Scholar and PubMed databases using a predefined combination of keywords. All gathered articles were reviewed for the content regarding T2DM, Acalypha wilkesiana, mechanism of action, and safety. A total of 44 articles were considered in this review. Several experimental studies revealed that extracts of Acalypha wilkesiana…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
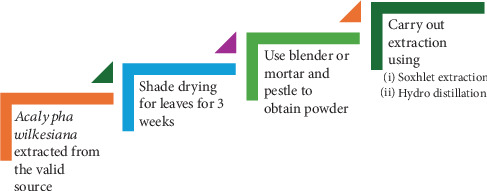 Figure 1
Figure 1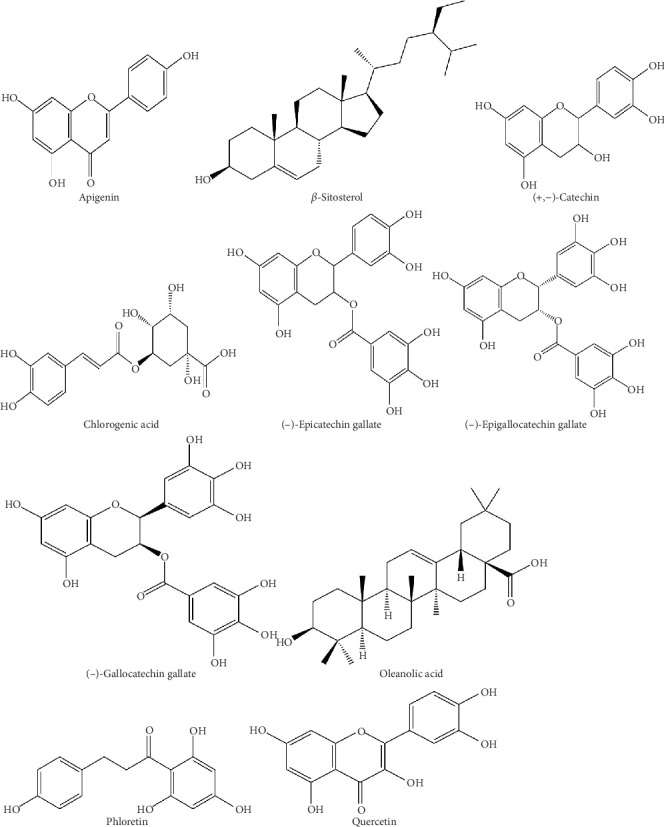 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNatural Antidiabetic Agents Studies · Pharmacological Effects of Medicinal Plants · Natural product bioactivities and synthesis
1. Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by insulin resistance, culminating in impaired insulin secretion and action. Consequently, glucose molecules accumulate in the blood vessels, leading to hyperglycemia and complications such as hyperosmolarity hyperglycemia state [1, 2]. In addition to insulin resistance, progressive dysfunction of pancreatic β-cells, increased hepatic glucose production, and low-grade inflammation are recognized contributors to the pathogenesis of T2DM. These mechanisms together accelerate the metabolic imbalance that underlies chronic hyperglycemia [3]. Although the disorder can be asymptomatic, individuals with T2DM present increased nocturnal urinary frequency, blurry vision, sores that heal slowly, tingling hands, and changes in mental status, among others [4].
Globally, around 500 million adults aged between 20 and 80 years were living with diabetes, according to a 2023 survey by the World Health Organization [5]. As of 2021, this represented 10.5% of the world's population in the age group. In Africa, an estimated 24 million people have diabetes, with an anticipated growth of 55 million by 2045. This is compounded by the fact that more than half (54%) of people living with diabetes in the African region are undiagnosed. In context with the report, 95% of persons diagnosed with diabetes had Type 2 diabetes [5]. In industrialized regions such as North America and Europe, prevalence is highest among adults over 65 years, driven largely by obesity, sedentary lifestyles, and aging populations. By contrast, developing regions experience an earlier onset of T2DM, often before the age of 45, associated with rapid urbanization, nutrition transitions, and limited healthcare access [5].
To counteract this health threat, many studies have documented the use of plants for management of T2DM [6–8]. There has been exploration of phytochemicals and their antidiabetic properties for commonly used medicinal plants such as Allium cepa, Persea americana, and Acalypha wilkesiana [8]. A. wilkesiana has been used in ethnobotanical medicine for diabetes management, but its pharmacological potential remains insufficiently characterized. The shrub, widely cultivated as an ornamental plant, is distinguished by its colorful foliage and is also traditionally applied in the treatment of skin infections, hypertension, and gastrointestinal disorders [9]. Phytochemical screening has identified flavonoids, tannins, saponins, terpenoids, and phenolic compounds, many of which are associated with hypoglycemic or antioxidant activities in other medicinal plants [10]. Unlike Allium cepa or Persea americana, which are well documented, A. wilkesiana represents an understudied but promising candidate for antidiabetic research. Its unique phytochemical profile and traditional relevance provide a compelling rationale for review.
This paper is aimed at thoroughly reviewing the current understanding of critical phytochemicals, pharmacological action, potency, and safety of A. wilkesiana in managing T2DM. This will enhance its validity in contemporary ethnobotanical medicine and provide insights into the urgent future research necessary to advance care among patients with T2DM.
2. Materials and Methods
A narrative review was thoroughly conducted by searching Google Scholar and PubMed databases. The keywords “Type 2 diabetes”, “Type 2 diabetes mellitus”, “t2dm”, “Acalypha wilkesiana”, “copper leaf”, “alpha-glucosidase inhibitors”, “glycemic control”, “blood sugar control”, “mechanism of action”, and “safety” were combined using the Boolean operators “AND” and “OR” to retrieve peer-reviewed papers published up to 2025. The retrieved articles were screened and analyzed based on their relevance to the review's objectives. Snowballing of the retrieved articles was then conducted to collate adequate data. Articles with information irrelevant to the review's aim were excluded. While preparing the final report of this review, all included articles were cross-checked. A total of 44 articles was considered in this review.
3. Results and Discussion
3.1. Current Treatment of T2DM
The management of T2DM involves lifestyle modifications, such as diet, exercise, and weight control. It also includes pharmacological interventions, where patients take medications such as oral antidiabetic drugs (OADs) and insulin injections [11]. Lifestyle changes, such as dietary adjustments, regular physical activity, and weight management, form the cornerstone of T2DM management [12]. The OADs are the first-line therapy for most patients with T2DM, and they can be classified into different categories based on their mechanisms of action [13]. The biguanide class includes medications like metformin, which reduces hepatic glucose synthesis and enhances peripheral glucose uptake [14]. This class is associated with side effects such as gastrointestinal disturbances, lactic acidosis, and vitamin B12 deficiency. Other classes of drugs include sulfonylureas and meglitinides which stimulate insulin secretion from pancreatic beta-cells [15]. Besides, they are accountable for side effects such as weight gain and hypoglycemia. It is therefore significant to monitor blood sugars when these medications are being administered.
Additionally, thiazolidinediones, such as pioglitazone and rosiglitazone, improve insulin sensitivity in muscle and adipose tissue [16]. Dipeptidyl peptidase-4 (DPP-4) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists, such as sitagliptin and liraglutide, boost incretin-mediated insulin secretion while suppressing glucagon release [17]. The major side effects reported by patients who use these drugs include upper respiratory tract infections, urinary tract infections, hypersensitivity, gastrointestinal disturbances, hypoglycemia, pancreatitis, and thyroid cancer [17]. Sodium-glucose cotransporter-2 (SGLT-2) inhibitors, such as dapagliflozin and empagliflozin, inhibit renal glucose reabsorption and increase urinary glucose excretion [18]. This class has been reported to increase cases of genital infections, urinary tract infections, dehydration, ketoacidosis, and bone fractures [18] (see Table 1).
The choice of OADs depends on various factors, such as efficacy, safety, tolerability, cost, and patient preference [18]. The conventional OADs outlined in Table 1 are effective, but they have several significant drawbacks. Several important issues have been identified, including progressive loss of efficacy (secondary failure), weight gain (e.g., sulfonylureas and thiazolidinediones), hypoglycemia risks, gastrointestinal intolerance (e.g., metformin), and cardiovascular safety concerns such as risks of heart failure due to rosiglitazone or saxagliptin [19]. In addition, drug interactions with alcohol, anticoagulants, and antibiotics, among other drugs raise a concern. Genetic variability, such as polymorphisms in drug-metabolizing enzymes, transporters, and receptors can also affect drug response and toxicity [20]. Moreover, compliance issues such as poor adherence, discontinuation, and switching of therapy play a significant role in limiting proper treatment of T2DM disease. Ongoing studies in the field of healthcare are primarily concerned with the search for better treatment options for many noncommunicable diseases, including T2DM. According to Home and Mehta, [21] nanotechnology has rapidly expanded in several research domains, including phytomedicine to alleviate oxidative stress in diabetes [22]. Although OADs are satisfactory for most patients, insulin treatment continues to play a role in patients with definite T2DM or poor control of glycemia [23]. Insulin treatment varies from basal insulin to intensive therapy using rapid-acting analogues. Combination therapy in the form of metformin with SGLT-2 inhibitors or GLP-1 receptor agonists is now also a component of current strategies for overcoming drug resistance and enhancing outcomes [24].
However, the persistent limitations of conventional treatment have highlighted the significance of medicinal plants with antidiabetic properties. A. wilkesiana has exhibited significant hypoglycemic, antioxidant, and antihyperglycemic properties in preclinical settings, with efficacy comparable to conventional medications such as metformin and acarbose, as detailed in Tables 2 and 3. The findings indicate that A. wilkesiana could improve certain deficiencies of existing OADs while providing supplementary systemic advantages. Clinical trials remain necessary for confirming the safety and efficacy of this treatment in humans.
3.2. Overview of A. wilkesiana
A. wilkesiana belongs to the Euphorbiaceae plant family, one of the largest and most genetically diverse plant families that have been discovered for their significant role in the treatment and management of T2DM. It has nearly 322 genera and 8910 species ranging from large woody trees to weeds [32]. With such diversity, the family exhibits a wide array of phytoconstituents. Among the Acalypha species studied for their potential antidiabetic properties, A. wilkesiana has received considerable attention, likely due to its widespread distribution in tropical and subtropical regions and its documented medicinal applications [16]. A. wilkesiana also known by various local names such as copperleaf, fire-dragon, and Jacob's fruit, is not only valued for its medicinal properties but also widely used as an ornamental plant [15].
Medicinal significance of A. wilkesiana has been appreciated and recognized by different studies. In a research carried out to investigate the antifungal activity of this plant, Sherifat et al. observed antifungal activity of A. wilkesiana against Trichophyton rubrum and Candida albicans. Furthermore, they highlighted the plant's antimicrobial, anthelminthic, anticarcinogenic, anti-inflammatory, antioxidant, antimalarial, and hepatoprotective properties [15, 33]. The plant has been used in different areas of the world for a wide range of conditions such as antitumor in Nigeria, anti-inflammatory and treatment of headache and flu in Malaysia, regulation of menstrual flow in Fiji, and for management of rheumatic pains and swellings in Central America [34]. Additionally, an ethnobotanical study of A. wilkesiana revealed high efficacy in the treatment of arterial hypertension in Oyem, Northern Gabon. These results form a database for phytochemical studies for new antihypertensive compounds that can be used concurrently in the treatment of hypertensive diabetic patients [9].
3.3. Extraction and Phytochemicals of A. wilkesiana
Studies looking at A. wilkesiana have generally focused on three main parts of the plant: the root bark, the stem bark, and the leaves. Each of these carries a mix of useful compounds such as saponins, flavonoids, alkaloids, terpenoids, and tannins, but their reported strengths are not the same. Root bark extracts are often highlighted for lowering postprandial glucose, stem bark for its strong antioxidant profile, while the leaves have attracted the most attention overall because of their broader range of effects, such as improving insulin sensitivity and helping preserve β-cell function [35].
To obtain these compounds, researchers have tried different solvents like water, ethanol, methanol, and ethyl acetate, depending on the target isolate [16]. Among these, ethanol and water are most often used, and the bulk of published studies concentrate on leaf extractions [36, 37]. These methods described are similar: leaves are typically dried, powdered, and then processed through techniques such as Soxhlet extraction or hydrodistillation to produce crude extracts or essential oils. A general outline of these approaches is illustrated in Figure 1 [37, 38].
Upon analysis of these extracts, scientists consistently reported a rich chemical profile. The leaves contain polyphenols, terpenoids, flavonoids, and glycosides, along with tannins, alkaloids, and steroids. Some studies note that ethanol extractions reveal a broad spectrum of these compounds, while water extractions often bring out higher levels of saponins [18, 39]. These groups of compounds are not just chemical curiosities; they are associated with diverse biological activities, from antioxidant and antiviral effects to cardiovascular and antimicrobial benefits [39].
Several individual compounds stand out for their relevance to diabetes. For example, saponins like aescin and oleanolic acid have been linked with α-glucosidase inhibition and reduced glucose absorption [27]. Flavonoids such as quercetin and kaempferol act in insulin-like ways, enhancing glucose uptake while also protecting against oxidative stress [16, 35]. Phenolic acids like chlorogenic acid appear to interfere with enzymes such as α-amylase and PTP1B, supporting better insulin signaling [25]. Other receptors on methanolic extracts describe compounds such as rutin, ferulic acid, caffeic acid, and luteolin, which add further antidiabetic and lipid-modulating effects [26]. Representative chemical structures of these phytochemicals are provided in Figure 2, while a concise summary of their classes, properties, and biological targets is presented in Table 2.
3.4. Mechanism of Action, Safety, Potency, and Efficacy of A. wilkesiana
The antidiabetic potential of A. wilkesiana has been consistently supported by various in vivo studies, which highlight multiple mechanisms of action. A central pathway involves the inhibition of carbohydrate-digesting enzymes, particularly α-amylase and α-glucosidase, thereby delaying glucose absorption and reducing postprandial spikes [16, 40]. For example, Iyamu et al. demonstrated that ethanolic root bark extracts inhibited α-glucosidase at levels (50.48%–56.14%) comparable to the standard drug acarbose (51.12%–58.01%), suggesting a pharmacological similarity that warrants further exploration [39]. Complementary findings have shown that different plant parts yield varying inhibitory potencies, with root bark ethanolic extracts displaying the lowest IC₅₀ values against both α-glucosidase and α-amylase, indicating the highest hypoglycemic potential. However, this potency also raises concerns about toxicity, as the narrow therapeutic window could limit safe application.
Beyond enzyme inhibition, A. wilkesiana appears to enhance glucose utilization directly by stimulating uptake in muscle and adipose tissues, while also improving insulin sensitivity [42]. Importantly, it protects pancreatic β-cells by enhancing insulin secretion and shielding them from oxidative stress-induced apoptosis. Such effects are linked to its antioxidant constituents, particularly geraniin and corilagin, which exhibit vigorous free-radical scavenging activity [31]. These dual actions supporting β-cell survival and reducing oxidative stress address key pathophysiological factors in T2DM. Additional animal studies further strengthen this evidence [43].
Isirima and Uahomo also attributed the mechanism of action of A. wilkesiana to glibenclamide, a secretagogue that binds sulfonylurea receptors and stimulates insulin release from the pancreas. Their study also described that A. wilkesiana has a protective function on the liver and spleen. This was supported by the ability of the plant to reverse alloxan-induced insult on the liver and spleen of rat models. They further concluded the antidiabetic potential of A. wilkesiana when they exposed it to a diabetes-induced rat [40].
With regards to safety, Forcados et al. reported a dose-dependent increase in major liver markers, serum aspartate aminotransferase (AST), alkaline phosphatase (ALP), and alanine aminotransferase (ALT) when A. wilkesiana was administered to albino rats. Conversely, when the rats were administered a dose of 100 mg/kg, a decrease in the levels of the major liver markers was noticed. Hence, 100 mg/kg doses and below portrayed hepatoprotection while higher doses showed otherwise [42]. Moreover, the leaves of A. wilkesiana have been reported to have no deleterious effects on the morphology of red blood cells of diabetic rabbits [41]. Additionally, they demonstrated the ability to restore damaged cells of the pancreas and spleen caused by alloxan-induced diabetes [44]. This property of the plant provides a greater advantage over synthetic drugs of T2D as it does not only lower blood glucose levels but also ameliorates the functions of critical organs. Unlike synthetic drugs, which do indeed lower glucose, they cause side effects, harming the vital organs.
From the research conducted by Isirima and Uahomo, A. wilkesiana was efficacious in reducing hyperglycemia in experimental animals in a dose-dependent manner when they used 200 and 400 mg/kg of the plant extract [40]. Another study by Iyamu et al. also supported the hypoglycemic activity of the plant via α-glucosidase inhibition [39]. Furthermore, a study on the inhibitory activity of A. wilkesiana extracts against α-amylase and α-glucosidase, ethanolic root bark, and stem bark extracts demonstrated the lowest minimal extract concentration required for 50% enzyme inhibition (IC_50_) as compared to ethyl acetate and aqueous extracts. Stem ethanolic extracts had IC_50_ (μg mL^–1^) values of −37.10 ± 2.71^a^ and >1000^g^ towards α-glucosidase and α-amylase, respectively. Besides, the IC_50_ (μg mL^–1^) values for the root bark ethanolic extracts against α-glucosidase and α-amylase were 35.75 ± 1.95^a^ and 6.25 ± 1.05^a^, respectively [16]. Among the two parts of the plant, the lowest values of IC_50_ were for the root bark extract, which implies the extract concentration required to produce half of the maximum therapeutic effect. Moreover, the results suggest that root bark ethanolic extract is a potential source of phytochemicals with the highest hypoglycemic potency, and this promises to serve as a direction for better extraction process (see Table 3).
Overall, these findings position A. wilkesiana as a promising candidate for antidiabetic therapy, with mechanisms spanning enzyme inhibition, insulin sensitization, antioxidant defense, and organ protection. However, the balance between potency and toxicity, especially concerning extracts with very low IC₅₀ values remains a critical gap for future research.
The antidiabetic efficacy of A. wilkesiana has been evidenced in streptozotocin-induced animal models, whereas administration of leaf extracts significantly reduced hyperglycemia [43]. In a study, diabetic mice treated with streptozotocin alone exhibited a significant 445.2% increase in serum glucose after 30 days, while cotreatment with A. wilkesiana leaf extract restricted this rise to 305.6%, indicating a 139.6% disparity between the groups [43]. This significant decrease highlights the extract's therapeutic efficacy in the management of T2DM.
Therefore, it is crucial to determine the dosage of the plant extract that produces optimal hyperglycemic activity in humans [18]. In diabetic rats, a methanolic leaf extract at 40 mg/100 g body weight resulted in a 77.37% decrease in blood glucose, closely paralleling the 76.50% decrease reported with metformin [18]. Alongside managing glucose levels, the extract improved liver and kidney function indicators, lipid profiles, and hematological markers, suggesting broader systemic benefits that might enhance treatments.
4. Limitations
This review considered research studies performed using animal models and may not fully replicate the human condition of T2DM. Thus, the findings have limited applicability to human treatment. Moreover, the absence of clinical trials in humans indicates inadequate evidence concerning the safety, efficacy, and appropriate dosage of A. wilkesiana extracts for human application. The review also lacks explicit guidance for dosage and duration, and the observed toxicity at higher concentrations in rats indicates a necessity for future investigation into safe usage. Additionally, this review missed the potential variability in extract efficacy due to factors such as plant age or extraction process. Therefore, while the findings are promising, further research, particularly human clinical trials, is essential to confirm the therapeutic potential of this plant.
5. Conclusion
This comprehensive review has revealed that extracts of A. wilkesiana can lower blood glucose by modulating key enzymes involved in glucose metabolism and insulin signaling. They inhibit α-glucosidase and α-amylase enzymes, which are usually responsible for the breakdown of carbohydrates into glucose. It has been observed that ethanolic root bark extracts of the plant are more potent against the enzymes because of their lowest demonstrated IC_50_ value among other solvents and the standard acarbose, which works in the same biological pathway. Additionally, it can reverse the dysfunction of critical organs such as the spleen and pancreas in alloxan-induced models. Exploring the mechanisms of action, potency, and safety of A. wilkesiana is paramount to validate its ethnobotanical use. It also promises advances in developing antihyperglycemic agents that are more efficacious and safer than synthetic agents. Nevertheless, the safety profile of this plant is still an area of concern because there are no human-tailored standard doses. Thus, further research should focus on clinical trials to establish standard doses and ensure the safety profile of A. wilkesiana in T2DM management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rasouli H. Ramalho T. C. Popović-DjordjevićJ. B. Devkota H. P. Editorial: New Opportunities in Drug Design for the management and Treatment of Type 2 Diabetes Frontiers in Pharmacology 20231410.3389/fphar.2023.118705737089955 PMC 10116046 · doi ↗ · pubmed ↗
- 2Reed J. Bain S. Kanamarlapudi V. A Review of Current Trends With Type 2 Diabetes Epidemiology, Aetiology, Pathogenesis, Treatments and Future Perspectives Diabetes, Metabolic Syndrome and Obesity 2021143567360210.2147/DMSO.S 31989534413662 PMC 8369920 · doi ↗ · pubmed ↗
- 3Młynarska E. Czarnik W. Dzieża N. Type 2 Diabetes Mellitus: New Pathogenetic Mechanisms, Treatment and the Most Important Complications International Journal of Molecular Sciences 2025263 p. 109410.3390/ijms 2603109439940862 PMC 11817707 · doi ↗ · pubmed ↗
- 4CDC Diabetes Symptoms of Diabetes 2024[cited 2025 Oct 23] Available from: https://www.cdc.gov/diabetes/signs-symptoms/index.html
- 5Analytical Fact Sheet: Diabetes, a Silent Killer in Africa[cited 2025 Oct 23]. Available from: https://medbox.org/document/analytical-fact-sheet-diabetes-a-silent-killer-in-africa
- 6Jacob B. Narendhirakannan R. T. Role of Medicinal Plants in the Management of Diabetes Mellitus: A Review 3 Biotech 201991 p. 410.1007/s 13205-018-1528-02-s 2.0-8505885528330555770 PMC 6291410 · doi ↗ · pubmed ↗
- 7Tienda-Vázquez M. A. Melchor-Martínez E. M. Elizondo-Luévano J. H. Antidiabetic Plants for the Treatment of Type 2 Diabetes Mellitus and Associated Bacterial Infections Processes 2023115 p. 129910.3390/pr 11051299 · doi ↗
- 8Muema F. W. Nanjala C. Oulo M. A. Wangchuk P. Phytochemical Content and Antidiabetic Properties of Most Commonly Used Antidiabetic Medicinal Plants of Kenya Molecules 20232820 p. 720210.3390/molecules 2820720237894680 PMC 10609527 · doi ↗ · pubmed ↗