Modification of the Low FODMAP Diet Is Feasible in the Treatment of Irritable Bowel Syndrome: A Randomised Crossover Study
Line Graser Jensen, Marie Kjær, Jens Rikardt Andersen

TL;DR
A modified low FODMAP diet focusing on specific carbohydrates can relieve IBS symptoms as effectively as the standard diet.
Contribution
The study identifies that restricting fructooligosaccharides and galactooligosaccharides is as effective as the full low FODMAP diet for IBS.
Findings
The low FOS + GOS diet provided significant symptom relief comparable to the standard low FODMAP diet.
The low polyol diet did not significantly improve symptoms in IBS patients.
75% of patients experienced clinically relevant symptom relief on the low FOS + GOS diet.
Abstract
Irritable bowel syndrome (IBS) can be dietary managed by applying restrictions in the diet of fermentable oligosaccharides, disaccharides, monosaccharides and polyols—the low FODMAP diet. However, many patients have major difficulties integrating the diet into their daily lives. We aimed to investigate if the three carbohydrate groups eliminated in the traditional low FODMAP diet are equally important in relieving gastrointestinal symptoms in IBS. Nine patients with IBS according to the Rome IV criteria and referred to specialised diet therapy in private clinics were randomised in a crossover design to three different carbohydrate-modified diets: (A) low polyol diet, (B) low FOS + GOS diet and (C) low standard FODMAP diet for 4 weeks on each diet. Symptoms were assessed by the Birmingham IBS questionnaire and adequate relief (IBS-AR) and quality of life by the IBS Quality of Life…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
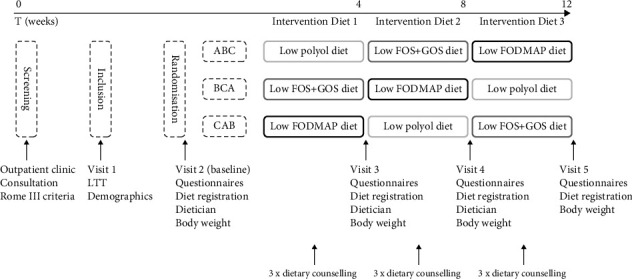 Figure 1
Figure 1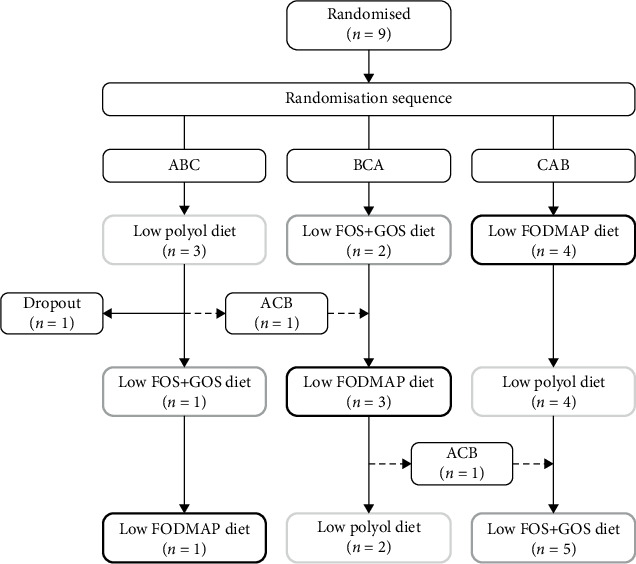 Figure 2
Figure 2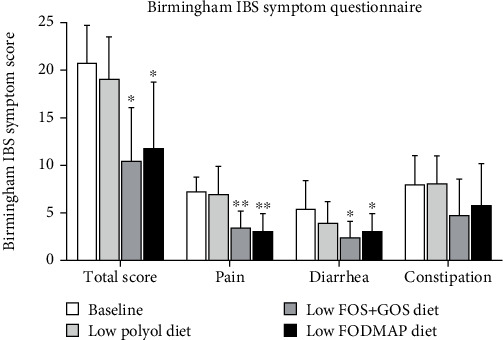 Figure 3
Figure 3- —Københavns Universitet
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Inflammatory Bowel Disease · Diet and metabolism studies
1. Introduction
Irritable bowel syndrome (IBS) is the most common functional gastrointestinal disorder affecting 10%–20% of the population globally and is characterised by chronic symptoms such as recurrent abdominal pain in combination with bloating as well as diarrhoea, constipation or both [1, 2]. The symptoms are often severe, and IBS can substantially impact patients' health-related quality of life and is associated with increased healthcare utilisation and has socioeconomic consequences [2–6]. However, even though IBS is a highly prevalent gastrointestinal disorder, the pathophysiology is poorly understood [4].
Dietary restriction of highly fermentable oligosaccharides, disaccharides, monosaccharides and polyols (low FODMAP diet) is a well-documented therapeutic measure in the symptomatic management of IBS [7–9]. The underlying hypothesis of the low FODMAP diet suggests that restricting the intake of these groups of poorly absorbed and highly fermentable short-chain carbohydrates reduces intestinal osmolarity and gas production, thus reducing gastrointestinal symptoms, particularly pain, bloating and diarrhoea, thus improving the quality of life [10, 11]. The low FODMAP diet is considered the first-line treatment in patients with IBS, with a clinical response in 50%–76% of patients [12–15]. However, patients find it difficult to comply with the low FODMAP diet due to the extensive elimination of foods in their daily life [16, 17]. There is increasing evidence that the standard low FODMAP diet can be simplified to increase compliance [9, 18–20].
Due to the highly restrictive nature of the standard low FODMAP diet, we aimed to investigate if all carbohydrate groups eliminated in the low FODMAP diet are equally important in relieving gastrointestinal symptoms in IBS.
2. Material and Methods
2.1. Study Participants
Consecutive (recruited in the order of appearance in the clinics without preselection besides the exclusion criteria mentioned below) patients, age 18–65 years and with a BMI of 18.5–25.0 kg/m^2^ (to avoid the influence of weight-reducing diets), diagnosed with IBS according to the Rome IV criteria [17] were recruited from private outpatient clinics specialised in gastroenterology in the Copenhagen area after exclusion of other diseases responsible for their symptoms.
All patients were referred for specialised dietary treatment and had to pay for this in the normally free Danish health system, thereby being highly motivated. All patients were of Subtype M. Patients were not included if they had problems with the Danish language, had structural gastrointestinal diseases, were pregnant, eliminated foods from their habitual diet, were medicated with drugs that could potentially interfere with the end points or had a prior history of eating disorders. None of the patients received medications for chronic diseases.
2.2. Study Design and Randomisation
The study design, timeline and measurements are illustrated in Figure 1. Patients were randomised in a crossover design to three intervention diets for 4 weeks each without wash-out periods for a total period of 12 weeks. Patients were allocated by sealed opaque envelopes with three different sequences determining the order of the intervention diets, ABC, BCA or CAB, as standard block randomisation.
2.3. Intervention
The intervention consisted of three different carbohydrate-modified diets in randomised order: (A) low polyol diet, (B) low fructooligosaccharides (FOS) + galactooligosaccharides (GOS) diet and (C) low FODMAP diet. The three intervention diets were based on the original low FODMAP principles [8], where foods included or excluded were based on data from the Monash University database regarding the content of FODMAPs in foods [21] The low polyol diet (A) excluded foods containing polyols. The low FOS + GOS diet (B) excluded oligosaccharides (FOS and GOS). The low FODMAP diet (C) excluded oligosaccharides, disaccharides, monosaccharides and polyols. For all three intervention diets, free fructose in the range of a maximum of three pieces of fruit per day was allowed free of choice to improve compliance with the study protocol. Traditional IBS dietary advice was given routinely and kept constant during the three treatment periods along with the special instructions.
Prior to every intervention diet, all patients were instructed by an experienced, certified clinical dietitian on how to adhere to each specific diet. In addition, a list of foods to be included or excluded for each diet, together with daily meal suggestions, was provided and reviewed with the patients. During every intervention period, the patients received weekly dietary counselling, either as outpatient visits or phone calls by the same dietician. Diet registrations were performed to ensure adherence to the intervention diets for all patients.
2.4. Outcomes
The primary outcome of the study was the change in gastrointestinal symptoms assessed by the Birmingham IBS questionnaire [22] from baseline and after each intervention diet. Secondary outcomes were the proportion of patients who experienced adequate relief of their IBS symptoms (IBS-AR) and the change in health-related quality of life (IBS-QOL). All questionnaires were translated into Danish.
2.5. Questionnaires
The questionnaires at baseline and after the completion of each intervention diet during outpatient visits included the following: Birmingham IBS symptom questionnaire [22], adequate relief of IBS symptoms (IBS-AR) [23] and IBS Quality of Life Scale questionnaire (IBS-QOL) [24].
2.6. Assessment of IBS Symptom Severity
Gastrointestinal symptoms were assessed by the Birmingham IBS, a disease-specific tool developed to measure the presence and severity of IBS symptoms. The Birmingham IBS symptom questionnaire consists of 11 questions based on the frequency of IBS symptoms on a 6-point Likert response scale, ranging from 0 (none of the time) to 5 (all the time). Responses are presented as a total score and scores for each of the three underlying variables: pain, diarrhoea and constipation [19]. Higher scores indicate higher symptom severity. The adequate relief of IBS symptoms assessment (IBS-AR), a dichotomous response question, was applied to assess whether the patients had experienced adequate or satisfactory relief of their IBS symptoms because of the intervention diets.
2.7. Assessment of Quality of Life
Health-related quality of life was evaluated by the IBS-QOL questionnaire [24]. The IBS-QOL questionnaire is a validated disease-specific tool used to assess the impact of gastrointestinal symptoms and the effects of treatment for IBS and is composed of 34 questions evaluating eight subscale domains found to be of relevance for patients with IBS: dysphoria, interference with activity, body image, health worry, food avoidance, social reaction, sexual and relationships. Each item has a 5-point Likert response scale, ranging from 0 (not at all) to 5 (extremely). In the present study, the individual responses to the IBS-QOL questionnaire were summed and averaged for a total score, with lower scores indicating improved quality of life [24].
2.8. Statistical Analysis
The Wilcoxon paired-rank test and Friedman rank-sum test were applied to assess changes in Birmingham IBS symptom scores and IBS-QOL scores. Dichotomous variables for patient-reported adequate relief of IBS symptoms were compared using Fisher's exact test. Categorical variables were presented as numbers or percentages, and continuous variables were presented as the mean ± SD. The intention to treat population was defined as patients who were assessed more than one time since baseline. The level of statistical significance was set to p < 0.05. The sample size calculation (n = 9) was based on 80% power, a level of significance of 0.05 (two-sided) and a need for a difference in symptoms of 20% to be clinically relevant.
2.9. Ethical Statements
The study was approved by the Committees of Health Research Ethics in the Capital Region of Denmark (H62014044) and the Danish Data Protection Agency (2012-58-0004). Oral and written informed consents were obtained from all study participants, and the study was in accordance with the Principles of Helsinki.
3. Results
The patient's demographics are presented in Table 1. Nine patients were randomly allocated to a randomisation sequence ABC (n = 3), BCA (n = 2) and CAB (n = 4), determining the order of the three intervention diets. In randomisation sequence ABC, one patient dropped out after completing the first intervention diet due to bad tolerance to the low polyol diet. In the same group, one patient unexpectedly changed randomisation sequence from ABC to BCA after completing the first intervention diet (Figure 2). No patients had comorbidities that could compromise the evaluation.
Changes in IBS symptom severity assessed by the Birmingham IBS symptom questionnaire are shown in Figure 3. Compared with baseline (score: 20.8 ± 3.9), patients demonstrated a significant reduction in gastrointestinal symptoms on the low FOS + GOS diet and the low FODMAP diet (score: 10.5 ± 5.6 and 11.8 ± 7.0, respectively, p < 0.05). Further, the three underlying variables of the Birmingham IBS questionnaire (pain, diarrhoea and constipation) were also reduced compared to baseline on the low FOS + GOS diet (scor: pain, 7.3 ± 1.5 vs. 3.4 ± 1.8, p < 0.01; diarrhoea, 5.4 ± 3.0 vs. 2.4 ± 1.7, p < 0.01; constipation, 8.0 ± 3.0 vs. 4.8 ± 3.7, p > 0.05) and the low FODMAP diet (score: pain, 7.3 ± 1.5 vs. 3.0 ± 1.9, p < 0.05; diarrhoea, 5.4 ± 3.0 vs. 3.0 ± 1.9, p < 0.05; constipation, 8.0 ± 3.0 vs. 5.8 ± 4.4, p > 0.05); however, though constipation scores were numerically lower compared to both baseline and the low polyol diet (score: 8.1 ± 2.9), the differences were not statistically significant (Figure 3). No difference in Birmingham IBS symptom scores was found between the low FOS + GOS diet and the low FODMAP diet. Patients demonstrated significantly higher IBS symptom severity on the low polyol diet compared to both the low FOS + GOS diet and the low FODMAP diet (p < 0.05 and p < 0.05, respectively), and no change in Birmingham IBS symptom scores was found on the low polyol diet compared to baseline (score: 19.1 ± 4.4 vs. 20.8 ± 3.9).
When evaluating adequate relief (IBS-AR), none of the patients (0%) on the low polyol diet experienced adequate or satisfactory relief of their IBS symptoms. In contrast, the proportion of patients reporting adequate relief was 75% on the low FOS + GOS diet and 62.5% on the low FODMAP diet, which were significantly higher compared to the low polyol diet (p < 0.01 and p < 0.01, respectively). No significant difference in adequate relief was found between the low FOS + GOS diet and the low FODMAP diet.
Quality of life was significantly improved on the low FOS + GOS diet compared to baseline, with an overall IBS-QOL score of 25.5 ± 15.1 compared to 44.0 ± 13.2 at baseline (p < 0.05). The following subscale domains were also improved on the low FOS + GOS diet: body image (p < 0.05), health worry (p < 0.05) and sexual function (p < 0.01). The overall IBS-QOL score was numerically lower on the low FODMAP diet compared to baseline, but the difference was not statistically significant (score: 30.2 ± 19.6 vs. 44.0 ± 13.2). However, evaluating IBS-QOL subscale domains for the low FODMAP diet, body image and health worry improved statistically significantly compared to baseline (p < 0.05 and p < 0.05). No change in IBS-QOL scores was observed on the low polyol diet compared to baseline (score: 41.4 ± 11.2 vs. 44.0 ± 13.2) (Table 2).
4. Discussion
In this crossover study, we investigated if all carbohydrate groups eliminated in the low FODMAP diet have the same impact in relieving gastrointestinal symptoms in patients with IBS. Our main findings were that only eliminating oligosaccharides from the diet improved gastrointestinal symptoms equally to the restricted low FODMAP diet in patients with IBS. In addition, the proportion of patients who were satisfied with their symptoms was 75% on the low FOS + GOS diet and 62.5% on the low FODMAP diet, similar to prior studies assessing the effect of the low FODMAP diet in patients with IBS [15, 25, 26]. Results from the Birmingham IBS symptom questionnaire also indicated that the low FOS + GOS diet and the low FODMAP diet induce a similar reduction of gastrointestinal symptoms in patients with IBS, strengthening the conclusion. However, there is a lack of evidence on the general effect of polyols on intestinal function and conflicting results pertaining to polyol malabsorption in IBS [27]. Polyol malabsorption has been found to increase when polyols are ingested in combination with other carbohydrates and may induce laxative effects, as well as flatulence, bloating and abdominal discomfort in sensitive individuals [27, 28]. In addition, polyol ingestion can lead to intestinal dysmotility in patients with IBS [27]. However, when polyols were eliminated from the present study's diet, there was no improvement in any of the common symptoms of intestinal dysmotility (abdominal pain, nausea, vomiting, bloating and constipation). We found that solely eliminating polyols from the diet did not affect gastrointestinal relief of IBS symptoms or quality of life, indicating that polyols alone may not play a major role in the dietary management of IBS. Furthermore, a generalised alleviation of the low FODMAP diet was shown to reduce the beneficial effects of the treatment [29]. This adds to the conclusion that moderation of the low FODMAP diet should be conducted by allowing the intake of polyols in these highly selected patients referred for dietary changes. This finding is not in agreement with a study reintroducing sorbitol and finding abdominal pain within 1 day [18]. Probably, the dose of polyols is a determining factor.
Our findings point towards a specific combination of carbohydrates (FOS and GOS) as the main drivers responsible for provoking exacerbations of gastrointestinal symptoms in IBS. This is in line with a study by Biesiekierski et al. [30], who also suggest that oligosaccharides may be responsible for the symptoms experienced by patients with IBS [31]. This challenges the current FODMAP hypothesis, suggesting that IBS symptoms are induced in a dose-dependent manner and not by individual carbohydrates [32].
Although this study shows great potential to modify the low FODMAP and alleviate the extent of foods eliminated from the diet, there are some limitations to this study. Despite the crossover design of the study reducing the biological variation and the highly selected patients, the number of participants is low. However, a small sample showing clear results is not an indication of a Type 1 error. A disadvantage of the crossover design is the risk of carry-over effects between the three diets. This risk may be reduced by a washout period. However, it would be problematic, as the washout diet should be the habitual diet, and the patients were referred for help in changing that diet and paid for that. It is reasonable to assume that 4 weeks is sufficient to eliminate or markedly reduce a potential carry-over effect. In the study, significant differences in gastrointestinal symptoms are found between the low polyol diet and both the low FOS + GOS diet and low FODMAP diet, meaning that this carry-over effect is probably small. The study's external validity may be reduced by the fact that most participants were female, but that is the general finding in every investigation and very characteristic for Danish IBS patients. Furthermore, the recruitment model involved private clinics and some payment in a dominating free-of-charge public health system, which could give rise to selection bias with restricted possibilities to extrapolate the results to the total population of patients with IBS. The adherence to the diets with low GOS and FOS, however, was extremely good, probably due to a very high degree of motivation if treatment is paid for. However, despite this, the results of this study are clear and of a clinically relevant size of order despite the limited number of patients. The low polyol diet was related to poorer adherence than the others, also indicating that the patients did not find it useful. Nine patients were insufficient to define risk factors for different outcomes and for comparisons of subgroups.
5. Conclusion
Low FOS/low GOS diets improved gastrointestinal symptoms equally to the standard low FODMAP diet in patients with IBS, but polyol restriction did not have any clinically relevant effect. We recommend that the starting point in patients with IBS should be a low FOS/low GOS diet supplemented by standard dietary advice to IBS patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Longstreth G. F. Thompson W. G. Chey W. D. Houghton L. A. Mearin F. Spiller R. C. Functional Bowel Disorders Gastroenterology 200613051480149110.1053/j.gastro.2005.11.0612-s 2.0-3364620168416678561 · doi ↗ · pubmed ↗
- 2Card T. Canavan C. West J. The Epidemiology of Irritable Bowel Syndrome Clinical Epidemiology 20146718010.2147/CLEP.S 402452-s 2.0-8489354510324523597 PMC 3921083 · doi ↗ · pubmed ↗
- 3Agarwal N. Spiegel B. M. R. The Effect of Irritable Bowel Syndrome on Health-Related Quality of Life and Health Care Expenditures Gastroenterology Clinics of North America 2011401111910.1016/j.gtc.2010.12.0132-s 2.0-7995156970021333898 · doi ↗ · pubmed ↗
- 4Saha L. Irritable Bowel Syndrome: Pathogenesis, Diagnosis, Treatment, and Evidence-Based Medicine World Journal of Gastroenterology 20142022 p. 675910.3748/wjg.v 20.i 22.67592-s 2.0-84902206375 PMC 405191624944467 · doi ↗ · pubmed ↗
- 5Mönnikes H. Quality of Life in Patients With Irritable Bowel Syndrome Journal of Clinical Gastroenterology 201145 S 98S 10110.1097/MCG.0b 013e 31821 fbf 442-s 2.0-7995881103621666428 · doi ↗ · pubmed ↗
- 6Donker G. A. Foets M. Spreeuwenberg P. Patients With Irritable Bowel Syndrome: Health Status and Use of Health Care Services British Journal of General Practice 199949447 p. 787PMC 131352810885081 · pubmed ↗
- 7Shepherd S. J. Lomer M. C. E. Gibson P. R. Short-Chain Carbohydrates and Functional Gastrointestinal Disorders American Journal of Gastroenterology 2013108570771710.1038/ajg.2013.962-s 2.0-8487758333323588241 · doi ↗ · pubmed ↗
- 8Gibson P. R. Shepherd S. J. Evidence-Based Dietary Management of Functional Gastrointestinal Symptoms: The FODMAP Approach Journal of Gastroenterology and Hepatology 201025225225810.1111/j.1440-1746.2009.06149.x 2-s 2.0-7614914178420136989 · doi ↗ · pubmed ↗