Evaluating Risk Factors for Surgical Site Occurrences: Infection and Wound Dehiscence Post Definitive Surgery for Sacrococcygeal Pilonidal Sinus Disease
Ellen G Maclean, Mary M Teoh, Cian Casey, Eoghan Blount, David Walsh, Alexander Armanios, Munyaradzi G Nyandoro

TL;DR
This study identifies risk factors for infections and wound dehiscence after surgery for a common condition in young adults, offering insights to improve surgical outcomes.
Contribution
The study provides a multi-centre evaluation of risk factors for surgical complications in sacrococcygeal pilonidal sinus disease using diverse surgical techniques.
Findings
Surgical site infections and wound dehiscence occurred in nearly 29% of patients each.
Secondary intention techniques and overweight status significantly increased infection risk.
Modified Karydakis flap showed the most favorable risk profile for wound dehiscence.
Abstract
Background: Sacrococcygeal pilonidal sinus disease (SPD) predominantly affects young adults and is associated with high morbidity after surgery. Surgical site infections (SSIs) and wound dehiscence (WD) are frequent and clinically significant complications. This study evaluated their rates and identified associated risk factors across multiple surgical techniques. Methods: A retrospective multi-centre cohort study was conducted across eight hospitals in Western Australia (2010-2019). Patients aged ≥15 years undergoing elective definitive SPD surgery with flap or secondary intention techniques were included. Data were extracted from medical records and electronic databases. SSI risk was analysed with univariate and multivariate logistic regression, while WD was examined using Cox proportional hazards modelling. Outcomes included 30-day re-presentation and readmission rates, with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2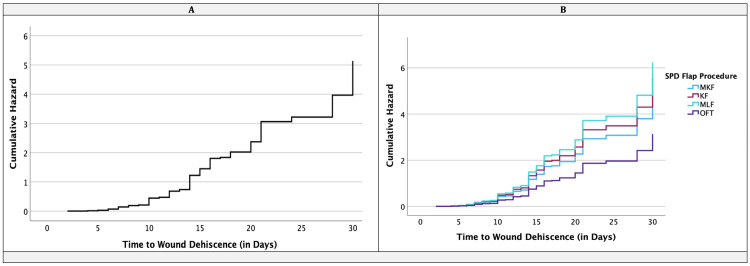 Figure 3
Figure 3| Variable (N = 774) | Cohort | SPD a Surgery Procedures | |||||||
| Total Sample | KF | MKF | MLF | SIT | OFT | p-value | |||
| Total Sample | N= | 774 | 302 | 242 | 92 | 90 | 48 | ||
| Sex | Male | n= | 617 | 235 | 189 | 74 | 77 | 42 | 0.309 |
| % | 79.7% | 77.8% | 78.1% | 80.4% | 85.6% | 87.5% | |||
| Female | n= | 157 | 67 | 53 | 18 | 13 | 6 | ||
| % | 20.3% | 22.2% | 21.9% | 19.6% | 14.4% | 12.5% | |||
| BMI group b | Healthy Weight | n= | 221 | 85 | 73 | 27 | 25 | 11 | 0.971 |
| % | 28.6% | 28.1% | 30.2% | 29.3% | 27.8% | 22.9% | |||
| Overweight | n= | 266 | 101 | 87 | 30 | 31 | 17 | ||
| % | 34.4% | 33.4% | 36.0% | 32.6% | 34.4% | 35.4% | |||
| Obese | n= | 287 | 116 | 82 | 35 | 34 | 20 | ||
| % | 37.1% | 38.4% | 33.9% | 38.0% | 37.8% | 41.7% | |||
| Age group | 15 to 19yrs | n= | 161 | 57 | 57 | 18 | 21 | 8 | 0.542 |
| % | 20.8% | 18.9% | 23.6% | 19.6% | 23.3% | 16.7% | |||
| 20 to 29yrs | n= | 371 | 148 | 103 | 48 | 44 | 28 | ||
| % | 47.9% | 49.0% | 42.6% | 52.2% | 48.9% | 58.3% | |||
| 30yrs + | n= | 242 | 97 | 82 | 26 | 25 | 12 | ||
| % | 31.3% | 32.1% | 33.9% | 28.3% | 27.8% | 25.0% | |||
| Diabetes | No | n= | 699 | 271 | 225 | 88 | 76 | 39 | 0.013* |
| % | 90.3% | 89.7% | 93.0% | 95.7% | 84.4% | 81.3% | |||
| Yes | n= | 75 | 31 | 17 | 4 | 14 | 9 | ||
| % | 9.7% | 10.3% | 7.0% | 4.3% | 15.6% | 18.8% | |||
| Hirsutism | No | n= | 570 | 226 | 189 | 72 | 58 | 25 | 0.001* |
| % | 73.6% | 74.8% | 78.1% | 78.3% | 64.4% | 52.1% | |||
| Yes | n= | 204 | 76 | 53 | 20 | 32 | 23 | ||
| % | 26.4% | 25.2% | 21.9% | 21.7% | 35.6% | 47.9% | |||
| Smoker | No | n= | 380 | 137 | 131 | 45 | 46 | 21 | 0.305 |
| % | 49.1% | 45.4% | 54.1% | 48.9% | 51.1% | 43.8% | |||
| Yes | n= | 394 | 165 | 111 | 47 | 44 | 27 | ||
| % | 50.9% | 54.6% | 45.9% | 51.1% | 48.9% | 56.3% | |||
| Ex-smoker / recent <3months | No | n= | 693 | 277 | 214 | 78 | 83 | 41 | 0.228 |
| % | 89.5% | 91.7% | 88.4% | 84.8% | 92.2% | 85.4% | |||
| Yes | n= | 81 | 25 | 28 | 14 | 7 | 7 | ||
| % | 10.5% | 8.3% | 11.6% | 15.2% | 7.8% | 14.6% | |||
| Financial | Public | n= | 721 | 285 | 219 | 85 | 88 | 44 | 0.156 |
| % | 93.2% | 94.4% | 90.5% | 92.4% | 97.8% | 91.7% | |||
| Private | n= | 53 | 17 | 23 | 7 | 2 | 4 | ||
| % | 6.8% | 5.6% | 9.5% | 7.6% | 2.2% | 8.3% | |||
| Variable (N = 774) | Cohort | SPD a Surgery Procedures | |||||||
| Total Sample | KF | MKF | MLF | SIT | OFT | p-value | |||
| Total Sample | N= | 774 | 302 | 242 | 92 | 90 | 48 | ||
| Re-do procedure | No | n= | 658 | 280 | 214 | 75 | 63 | 26 | < 0.001* |
| % | 85.0% | 92.7% | 88.4% | 81.5% | 70.0% | 54.2% | |||
| Yes | n= | 116 | 22 | 28 | 17 | 27 | 22 | ||
| % | 15.0% | 7.3% | 11.6% | 18.5% | 30.0% | 45.8% | |||
| IVABS on induction b | No | n= | 15 | 5 | 4 | 1 | 5 | 0 | 0.154 |
| % | 1.9% | 1.7% | 1.7% | 1.1% | 5.6% | 0.0% | |||
| Yes | n= | 759 | 297 | 238 | 91 | 85 | 48 | ||
| % | 98.1% | 98.3% | 98.3% | 98.9% | 94.4% | 100.0% | |||
| Query infected site | No | n= | 729 | 292 | 234 | 88 | 68 | 47 | < 0.001* |
| % | 94.2% | 96.7% | 96.7% | 95.7% | 75.6% | 97.9% | |||
| Yes | n= | 45 | 10 | 8 | 4 | 22 | 1 | ||
| % | 5.8% | 3.3% | 3.3% | 4.3% | 24.4% | 2.1% | |||
| Wound classification | Clean | n= | 101 | 25 | 42 | 14 | 8 | 12 | < 0.001* |
| % | 13.0% | 8.3% | 17.4% | 15.2% | 8.9% | 25.0% | |||
| Clean/ Contaminated | n= | 548 | 234 | 171 | 63 | 50 | 30 | ||
| % | 70.8% | 77.5% | 70.7% | 68.5% | 55.6% | 62.5% | |||
| Contaminated | n= | 125 | 43 | 29 | 15 | 32 | 6 | ||
| % | 16.1% | 14.2% | 12.0% | 16.3% | 35.6% | 12.5% | |||
| Drain-situ | No | n= | 407 | 160 | 126 | 23 | 90 | 8 | < 0.001* |
| % | 52.6% | 53.0% | 52.1% | 25.0% | 100.0% | 16.7% | |||
| Yes | n= | 367 | 142 | 116 | 69 | 0 | 40 | ||
| % | 47.4% | 47.0% | 47.9% | 75.0% | 0.0% | 83.3% | |||
| Methylene blue used | No | n= | 582 | 258 | 143 | 53 | 87 | 41 | < 0.001* |
| % | 75.2% | 85.4% | 59.1% | 57.6% | 96.7% | 85.4% | |||
| Yes | n= | 192 | 44 | 99 | 39 | 3 | 7 | ||
| % | 24.8% | 14.6% | 40.9% | 42.4% | 3.3% | 14.6% | |||
| Skin prep type | Povidone | n= | 644 | 256 | 206 | 70 | 81 | 31 | 0.002* |
| % | 83.2% | 84.8% | 85.1% | 76.1% | 90.0% | 64.6% | |||
| Chlorhexidine | n= | 130 | 46 | 36 | 22 | 9 | 17 | ||
| % | 16.8% | 15.2% | 14.9% | 23.9% | 10.0% | 35.4% | |||
| Variable (N = 774) | Cohort | SPD a Surgery Procedures | |||||||
| Total Sample | KF | MKF | MLF | SIT | OFT | p-value | |||
| Total Sample | N= | 774 | 302 | 242 | 92 | 90 | 48 | ||
| Recurrence | No | n= | 600 | 220 | 206 | 83 | 62 | 29 | <0.001* |
| % | 77.5% | 72.8% | 85.1% | 90.2% | 68.9% | 60.4% | |||
| Yes | n= | 174 | 82 | 36 | 9 | 28 | 19 | ||
| % | 22.5% | 27.2% | 14.9% | 9.8% | 31.1% | 39.6% | |||
| Surgical site infection | No | n= | 551 | 206 | 189 | 70 | 61 | 25 | 0.002* |
| % | 71.2% | 68.2% | 78.1% | 76.1% | 67.8% | 52.1% | |||
| Yes | n= | 223 | 96 | 53 | 22 | 29 | 23 | ||
| % | 28.8% | 31.8% | 21.9% | 23.9% | 32.2% | 47.9% | |||
| Dehiscence (n=684) | No | n= | 464 | 190 | 181 | 64 | - | 29 | <0.001* |
| % | 67.8% | 62.9% | 74.8% | 69.6% | - | 60.4% | |||
| Yes | n= | 220 | 112 | 61 | 28 | - | 19 | ||
| % | 32.2% | 37.1% | 25.2% | 30.4% | - | 39.6% | |||
| Hematoma | No | n= | 709 | 275 | 222 | 90 | 79 | 43 | 0.081 |
| % | 91.6% | 91.15 | 91.7% | 97.85 | 87.8% | 89.6% | |||
| Yes | n= | 65 | 27 | 20 | 2 | 11 | 5 | ||
| % | 8.4% | 8.9% | 8.3% | 2.2% | 12.2% | 10.4% | |||
| Seroma | No | n= | 763 | 296 | 241 | 92 | 87 | 47 | 0.111 |
| % | 98.6% | 98.0% | 99.6% | 100% | 96.7% | 97.9% | |||
| Yes | n= | 11 | 6 | 1 | 0 | 3 | 1 | ||
| % | 1.4% | 2.0% | 0.4% | 0.0% | 3.3% | 2.1% | |||
| Any post-op complication | No | n= | 486 | 180 | 169 | 61 | 50 | 26 | 0.033* |
| % | 62.8% | 59.6% | 69.8% | 66.3% | 55.6% | 54.2% | |||
| Yes | n= | 288 | 122 | 73 | 31 | 40 | 22 | ||
| % | 37.2% | 40.4% | 30.2% | 33.7% | 44.4% | 45.8% | |||
| Clear margins b | No | n= | 137 | 63 | 36 | 10 | 22 | 6 | 0.014* |
| % | 21.0% | 24.8% | 17.8% | 12.0% | 30.6% | 14.3% | |||
| Yes | n= | 516 | 191 | 166 | 73 | 50 | 36 | ||
| % | 79.0% | 75.2% | 82.2% | 88.0% | 69.4% | 85.7% | |||
| Cosmetic complaints | No | n= | 728 | 286 | 232 | 86 | 79 | 45 | 0.090 |
| % | 94.1% | 94.7% | 95.9% | 93.5% | 87.8% | 93.8% | |||
| Yes | n= | 46 | 16 | 10 | 6 | 11 | 3 | ||
| % | 5.9% | 5.3% | 4.1% | 6.5% | 12.2% | 6.3% | |||
| Variable | Number (Proportion) | |
| (n) | % | |
| Persistent wound discharge | 227 | 29.3 |
| Referred to other specialties | 29 | 3.7 |
| Plastics | 24 | 82.8 a |
| Wound hypergranulation | 40 | 5.2 |
| Fistula | 11 | 1.4 |
| Seroma | 11 | 1.4 |
| Sphincter damage | 8 | 1.0 |
| 30-day mortality | 0 | 0.0 |
| Variable (N = 774) | Surgical Site Infection Risk Factors | |||
| SSI (n) | SSI (%) | p–value | ||
| Age | 15 to 19 years | 39 | 24.2% | 0.133 |
| 20 to 29 years | 119 | 32.1% | ||
| Older than 30 years | 65 | 26.9% | ||
| Region | SMHS | 106 | 27.9% | 0.002* |
| EMHS | 47 | 22.3% | ||
| NMHS | 70 | 38.3% | ||
| Gender | Male | 179 | 29.0% | 0.808 |
| Female | 44 | 28.0% | ||
| BMI a | Healthy weight | 50 | 22.6% | 0.055 |
| Overweight | 84 | 31.6% | ||
| Obese | 89 | 31.0% | ||
| IVABs on induction b | No | 3 | 20.0% | 0.573 |
| Yes | 220 | 29.0% | ||
| Drain in-situ | No | 106 | 26.0% | 0.073 |
| Yes | 117 | 31.9% | ||
| Query infected site | No | 199 | 27.3% | <0.001* |
| Yes | 24 | 53.3% | ||
| Type of skin-prep | Povidone/Iodine | 170 | 26.4% | 0.001* |
| Chlorhexidine | 53 | 40.8% | ||
| Procedure index | Primary procedure | 181 | 27.5% | 0.056 |
| Re-do procedure | 42 | 36.2% | ||
| Closure technique | Primary closure | 194 | 28.4% | 0.447 |
| Secondary intention | 29 | 32.2% | ||
| Methylene blue | No | 180 | 30.9% | 0.024* |
| Yes | 43 | 22.4% | ||
| SPD procedure c | KF | 96 | 31.8% | 0.002* |
| MKF | 53 | 21.9% | ||
| MLF | 22 | 23.9% | ||
| SIT | 29 | 32.2% | ||
| OFT | 23 | 47.9% | ||
| Diabetes | No | 189 | 27.0% | 0.001* |
| Yes | 34 | 45.3% | ||
| Smoker | No | 90 | 23.7% | 0.002* |
| Yes | 133 | 33.8% | ||
| Hirsutism | No | 131 | 23.0% | <0.001* |
| Yes | 92 | 45.1% | ||
| Wound classification | Clean | 21 | 20.8% | 0.140 |
| Clean/Contaminated | 162 | 29.6% | ||
| Contaminated | 40 | 32.0% | ||
| Hematoma | No | 200 | 28.2% | 0.221 |
| Yes | 23 | 35.4% | ||
| Dehiscence | No | 153 | 27.6% | 0.244 |
| Yes | 70 | 31.8% | ||
| Seroma | No | 220 | 28.8% | 1.000 |
| Yes | 3 | 27.3% | ||
| Any post-op complication | No | 13 | 2.7% | <0.001* |
| Yes | 210 | 72.9% | ||
| Involved margins | No | 75 | 54.7% | <0.001* |
| Yes | 117 | 22.7% | ||
| Variable (N = 684) | Wound Dehiscence Risk Factors | |||
| Dehiscence (n) | Dehiscence (%) | p–value | ||
| Age | 15 to 19 years | 32 | 22.9% | 0.030* |
| 20 to 29 years | 113 | 34.6% | ||
| Older than 30 years | 75 | 34.6% | ||
| Region | SMHS | 110 | 33.5% | 0.075 |
| EMHS | 48 | 25.8% | ||
| NMHS | 62 | 36.5% | ||
| Gender | Male | 177 | 32.8% | 0.506 |
| Female | 43 | 29.9% | ||
| BMI a | Healthy Weight | 49 | 24.0% | <0.001* |
| Overweight | 68 | 28.9% | ||
| Obese | 103 | 42.2% | ||
| IVABs on Induction b | No | 2 | 20.0% | 0.514 |
| Yes | 218 | 32.2% | ||
| Drain in-situ | No | 85 | 26.8% | 0.005* |
| Yes | 135 | 36.8% | ||
| Query infected site | No | 206 | 31.2% | 0.003* |
| Yes | 14 | 60.9% | ||
| Type of skin-prep | Povidone/Iodine | 165 | 29.3% | <0.001* |
| Chlorhexidine | 55 | 45.5% | ||
| Procedure index | Re-do procedure | 35 | 39.3% | 0.121 |
| Primary procedure | 185 | 31.1% | ||
| Strict Bed rest | No | 23 | 41.1% | 0.136 |
| Yes | 197 | 31.4% | ||
| Methylene Blue | No | 170 | 34.3% | 0.048* |
| Yes | 50 | 26.5% | ||
| SPD Procedure c | KF | 112 | 37.1% | 0.018* |
| MKF | 61 | 25.2% | ||
| MLF | 28 | 30.4% | ||
| OFT | 19 | 39.6% | ||
| Diabetes | No | 182 | 29.2% | <0.001* |
| Yes | 38 | 62.3% | ||
| Smoker | No | 86 | 25.7% | <0.001* |
| Yes | 134 | 38.3% | ||
| Hirsutism | No | 127 | 24.8% | <0.001* |
| Yes | 93 | 54.1% | ||
| Wound Classification | Clean | 24 | 25.8% | 0.053 |
| Clean/Contaminated | 157 | 31.5% | ||
| Contaminated | 39 | 41.9% | ||
| Hematoma | No | 218 | 32.1% | 0.597 |
| Yes | 2 | 50.0% | ||
| Surgical Site Infection | No | 55 | 11.2% | <0.001* |
| Yes | 165 | 85.1% | ||
| Seroma | No | 220 | 32.4% | 0.182 |
| Yes | 0 | 0.0% | ||
| Any post-op complication | No | 0 | 0.0% | <0.001* |
| Yes | 220 | 88.7% | ||
| Involved Margins | No | 124 | 26.6% | <0.001* |
| Yes | 69 | 60.0% | ||
| Variable (N=684) | B | SE | Sig. | Exp(B) | (B) 95.0% CI | ||
| Lower | Upper | ||||||
| SPD Flap Procedure † | MKF | 0.45 | 0.28 | 0.111 | 1.57 | 0.90 | 2.73 |
| KF | 0.58 | 0.28 | 0.037 | 1.78 | 1.04 | 3.05 | |
| MLF | 0.69 | 0.32 | 0.031 | 1.99 | 1.06 | 3.73 | |
| Age | Years | 0.01 | 0.01 | 0.554 | 1.04 | 0.99 | 1.02 |
| BMI (kg/m2) | nn | 0.01 | 0.01 | 0.704 | 1.03 | 0.99 | 1.02 |
| Sex ‡ | Male | 0.10 | 0.19 | 0.590 | 1.11 | 0.77 | 1.59 |
| Smoker § | Yes | 0.31 | 0.15 | 0.040 | 1.37 | 1.02 | 1.85 |
| IVABs on Induction § | Yes | 0.42 | 0.74 | 0.574 | 1.52 | 0.36 | 6.45 |
| Drain In-Situ § | Yes | 0.03 | 0.15 | 0.857 | 1.03 | 0.77 | 1.37 |
| SSI Index Inpatient § | Yes | 0.62 | 0.68 | 0.363 | 1.85 | 0.49 | 7.02 |
| Region || | SMHS | 0.29 | 0.18 | 0.097 | 1.34 | 0.95 | 1.89 |
| EMHS | 0.06 | 0.21 | 0.787 | 1.06 | 0.70 | 1.60 | |
| Diabetes ¶ | No | 0.05 | 0.21 | 0.811 | 1.05 | 0.70 | 1.57 |
| Hirsutism ¶ | No | 0.02 | 0.16 | 0.885 | 1.02 | 0.75 | 1.40 |
| Query Infected Site ¶ | No | 0.12 | 0.30 | 0.696 | 1.12 | 0.63 | 2.01 |
| Re-Do Procedure ¶ | No | 0.12 | 0.21 | 0.576 | 1.12 | 0.75 | 1.70 |
| Hematoma Index Inpatient ¶ | No | 0.20 | 0.80 | 0.808 | 1.22 | 0.25 | 5.81 |
| Variable (N=774) | SPD a Surgery Procedures | ||||||
| Represented in the 1st month | |||||||
| Cohort | KF | MKF | MLF | SIT | OFT | p-value | |
| No | 565 | 202 | 193 | 70 | 67 | 33 | 0.015* |
| 73.0% | 35.8% | 34.2% | 12.4% | 11.9% | 5.8% | ||
| Yes | 209 | 100 | 49 | 22 | 23 | 15 | |
| 27.0% | 47.8% | 23.4% | 10.5%; | 11.0% | 7.2% | ||
| Representation destination | |||||||
| Cohort | KF | MKF | MLF | SIT | OFT | p-value | |
| Emergency department (ED) b | 105 | 50 | 24 | 9 | 13 | 9 | 0.034* |
| 50.2% | 47.6% | 22.9% | 8.6% | 12.4% | 8.6% | ||
| Ward | 9 | 2 | 6 | 1 | 0 | 0 | |
| 4.3% | 22.2% | 66.7% | 11.1% | 0.0% | 0.0% | ||
| Outpatient clinic | 66 | 30 | 12 | 12 | 8 | 4 | |
| 31.6% | 45.5% | 18.2% | 18.2% | 12.1% | 6.1% | ||
| General practitioner (GP) c | 29 | 18 | 7 | 0 | 2 | 2 | |
| 13.9% | 62.1% | 24.1% | 0.0% | 6.9% | 6.9% | ||
| Representation reason | |||||||
| Cohort | KF | MKF | MLF | SIT | OFT | p-value | |
| Pain | 8 | 2 | 3 | 1 | 3 | 0 | <0.001* |
| 4.3% | 22.2% | 33.3% | 11.1% | 33.3% | 0.0% | ||
| SSI d | 104 | 64 | 22 | 5 | 7 | 6 | |
| 49.8% | 61.5% | 21.2% | 4.8% | 6.7% | 5.8% | ||
| WD e | 70 | 27 | 19 | 16 | 0 | 8 | |
| 33.5% | 38.6% | 27.1% | 22.9% | 0.0% | 11.4% | ||
| Pain & SSI | 12 | 4 | 5 | 0 | 2 | 1 | |
| 5.7% | 33.3% | 41.7% | 0.0% | 16.7% | 8.3% | ||
| High output drain or Vac issues | 5 | 0 | 0 | 0 | 5 | 0 | |
| 2.4% | 0.0% | 0.0% | 0.0% | 100.0% | 0.0% | ||
| Tertiary bleeding | 6 | 2 | 0 | 0 | 4 | 0 | |
| 2.9% | 33.3% | 0.0% | 0.0% | 66.7% | 0.0% | ||
| Hypergranulation | 2 | 0 | 0 | 0 | 2 | 0 | |
| 1.0% | 0.0% | 0.0% | 0.0% | 100.0% | 0.0% | ||
| Constipation | 1 | 1 | 0 | 0 | 0 | 0 | |
| 0.5% | 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||
| Variable (N=774) | SPD a Surgery Procedures | ||||||
| Readmitted 1st Month | |||||||
| Total cohort | KF | MKF | MLF | SIT | OFT | p-value | |
| No | 716 | 282 | 228 | 87 | 76 | 43 | 0.027* |
| 92.5% | 39.4% | 31.8% | 12.2% | 10.6% | 6.0% | ||
| Yes | 58 | 20 | 14 | 5 | 14 | 5 | |
| 7.5% | 34.5% | 24.1% | 8.6% | 24.1% | 8.6% | ||
| Readmission Reason | |||||||
| Sub-group | KF | MKF | MLF | SIT | OFT | p-value | |
| Pain | 2 | 2 | 0 | 0 | 0 | 0 | 0.029* |
| 3.4% | 100.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||
| SSI b | 20 | 8 | 5 | 2 | 3 | 2 | |
| 34.5% | 40.0% | 25.0% | 10.0% | 15.0% | 10.0% | ||
| WD c | 18 | 8 | 4 | 2 | 1 | 3 | |
| 31.0% | 44.4% | 22.2% | 11.1% | 5.6% | 16.7% | ||
| Pain & SSI b | 8 | 2 | 4 | 0 | 2 | 0 | |
| 13.8% | 25.0% | 50.0% | 0.0% | 25.0% | 0.0% | ||
| High output drain or Vac d | 9 | 0 | 1 | 1 | 7 | 0 | |
| 15.5% | 0.0% | 11.1% | 11.1% | 77.8% | 0.0% | ||
| Refashion wound | 1 | 0 | 0 | 0 | 1 | 0 | |
| 1.7% | 0.0% | 0.0% | 0.0% | 100.0% | 0.0% | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnorectal Disease Treatments and Outcomes · Pelvic floor disorders treatments · Hidradenitis Suppurativa and Treatments
Introduction
Sacrococcygeal pilonidal sinus disease (SPD), first described by Mayo in 1833, predominantly affects young men and has experienced a notable increase in incidence over the last two decades [1-8]. The term ‘pilonidal’, derived from the Latin words pilus (hair) and nidus (nest), was introduced by Hodges in 1880 [6]. SPD is considered an acquired disease originating in the hair follicles of the natal cleft in the sacrococcygeal region. Established risk factors include male sex, hirsutism, obesity, a deep gluteal cleft, and a sedentary lifestyle [1-4,6-11]. A range of surgical techniques has been developed for the management of SPD, although no consensus exists regarding a gold standard procedure. This lack of agreement arises from high complication rates, including recurrence, surgical site infections (SSIs), wound dehiscence (WD), haematoma, seroma, sphincter injury and flap oedema [2-4,7-14]. Current literature supports flap reconstruction techniques as primary options for chronic SPD yet provides no clear guidance on which specific flap should be used [12-16]. The ideal procedure should require minimal hospitalisation, cause little discomfort, have low recurrence rates, allow for rapid return to work or study, and impose a limited burden on the health system [2,6,9,16,17].
The purpose of this study was to evaluate the occurrence of SSIs and WD, together with their associated risk factors, following definitive surgery for chronic SPD. Both flap-based reconstruction and secondary intention procedures were assessed, with the additional aim of identifying predictors of surgical site complications that may inform future practice.
This research represents the first Australian multi-centre cohort study to investigate SSIs and WD across different surgical approaches to SPD, including both flap and secondary intention techniques. Previous studies have often been limited to single centres or individual surgeons and have not examined risk factors in detail [8,10,11,18-21]. Their applicability to the Australian context is uncertain, given differences in patient demographics and healthcare systems. By addressing these limitations, the present study contributes to a clearer understanding of current surgical practice, local disease burden and associated outcomes. These insights may help refine decision-making, reduce complication rates and improve patient outcomes in the management of this common condition.
Materials and methods
This multi-centre observational analytical retrospective cohort study reviewed medical records from eight hospitals in Western Australia between January 2010 and December 2019. Hospitals A, B and G were part of the East Metropolitan Health Service (EMHS), C, D and F belonged to the South Metropolitan Health Service (SMHS), and E and H were within the North Metropolitan Health Service (NMHS). These sites included both tertiary teaching centres and peripheral hospitals, thereby providing a representative cross-section of surgical practice in the state. The choice of procedure at each site was influenced by surgeon preference, disease characteristics, and patient factors, thereby representing real-world clinical practice patterns. Each participating centre had fellowship-trained surgeons with substantial operative experience, ensuring uniformity in procedural expertise and minimising inter-centre variability.
Eligible participants were patients aged 15 years or older who underwent elective definitive surgery for chronic SPD. Both flap-based reconstruction and procedures managed by secondary intention, including laying open with marsupialisation, were included. Cases were identified through the Western Australian health databases TOPAS, WebPAS and iSOFT using ICD-10-AM codes and the procedure codes (30676-01) for excision or marsupialisation of a pilonidal cyst. Patients were excluded if surgery was performed as an emergency or if active infection with an abscess was present at the time of operation. Each patient was included only once, and all re-do cases in this study were patients who had their index procedures performed at centres outside the study catchment area, for which the investigators did not have access to the original procedure and follow-up details. The sample size was based on all available eligible cases during the study period. See Figure 1 for an overview of case selection.
Case selection †I & D = Incision and drainage of an acute abscess
Data were extracted by seven independent investigators (EM, MT, CC, EB, DW, AA, MGN) from medical records and cross-referenced with electronic databases to ensure accuracy. Missing data were assessed for randomness and excluded pairwise from analyses. Variables collected included demographics, comorbidities, operative details, histopathology, recurrence, and re-presentation or readmission. Information on outpatient clinic utilisation, wound care services, and hospital-in-the-home (HITH) involvement was also recorded. Thirty-day re-presentation and readmission rates were recorded. Patients were considered not to have experienced SPD recurrence if no re-admission or re-presentation with SPD was registered during the study period.
Definitions for key clinical variables were standardised prior to analysis. Hirsutism was categorised into abundant, little or none. BMI was categorised according to WHO definitions. Immediate complications referred to events occurring during the index hospital admission, whereas delayed complications were those occurring within 30 days. Recurrence was defined as reappearance of SPD beyond 30 days. SSI was defined using the Dell criteria and classified as superficial or deep. WD was defined as separation of the wound either during the index admission or at re-presentation to the hospital and wounds were classified according to the CDC surgical wound classification system.
The primary objective was to identify independent risk factors associated with SSIs following definitive surgery for SPD. The secondary objective was to evaluate predictors of WD and overall surgical site occurrences.
Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate. Continuous variables were compared using Student’s t-test or Mann-Whitney U test, depending on data distribution.
Univariate analyses were performed for all candidate variables, with those achieving p<0.1 entered into multivariate logistic regression models to identify independent predictors of SSI. Cox regression models were used to analyse time-to-event data. All analyses were conducted using IBM SPSS Statistics for Windows, Version 29 (Released 2023; IBM Corp., Armonk, New York, United States). A two-tailed p-value of <0.05 was considered statistically significant.
For SSIs, univariate analyses were followed by multivariate binary logistic regression to estimate odds ratios (ORs) with 95% confidence intervals (CIs). Independent variables considered included patient characteristics (BMI, diabetes, smoking status, hirsutism, sex, and age), perioperative factors (antibiotic prophylaxis, type of skin preparation, methylene blue use, operative duration, drain use, and whether it was a redo procedure), and pathological findings (surgical margins, wound classification).
For WD, univariate analyses were followed by Cox proportional hazards regression to model time to wound separation. WD was defined as a clinically diagnosed wound separation occurring during the index admission or at hospital re-presentation. Covariates considered included the same baseline, operative and pathological variables, in addition to post-operative complications (SSI, haematoma, seroma). Hazard ratios (HRs) with 95% CIs were reported. Proportional hazards assumptions were tested, and all variables meeting significance in univariate analysis were assessed in the multivariate model.
This study was approved by the South Metropolitan Health Service Human Research Ethics Committee (RGS511) and the University of Western Australia Human Research Ethics Committee (RA/4/20/4547) as a low-risk project. A waiver of consent was granted for this retrospective arm of the overarching study as all data were fully de-identified prior to analysis, in accordance with the National Statement on Ethical Conduct in Human Research (National Health and Medical Research Council Act, NHMRC, 2018. This study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) and STROBE-RECORD statements for cohort studies.
Results
Demographics
A total of 774 patients from eight hospitals were included in the study. Participant demographics are demonstrated in Table 1; most participants were male (n = 617, 79.7%) with a mean age of 27.1 years (SD 9.1). Men were slightly older than women at the time of surgery (27.3 vs 26.2 years). Body weight ranged from 32 to 210 kg, with men heavier on average than women (89.9 vs 80.5 kg). Mean height was 177.6 cm for men and 165.7 cm for women. The overall mean body mass index (BMI) was 28.6 (SD 6.2), consistent with the overweight range. More than one-third of the cohort was classified as obese (37.1%), and over half were current smokers (50.9%). The majority did not have diabetes (90.3%) and were not hirsute (73.6%) (Table 1).
Table 1: Participant demographics per SPD surgery typesValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s exact test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a SPD: Sacrococcygeal pilonidal sinus diseaseb BMI: Body mass index*
Surgical procedure types
Nine distinct procedures were identified and recategorised for analysis. These included the Karydakis flap (KF, 39.0%), modified Karydakis flap (MKF, 31.3%), modified Limberg flap (MLF, 11.9%), laying open with marsupialisation as a secondary intention technique (SIT, 11.6%), and a group of less common procedures such as Bascom’s cleft lift, gluteus maximus myocutaneous flap, Z-plasty and V-Y advancement, which were grouped as other flap techniques (OFT, 6.2%). Most participants were considered public patients (93.2%), and almost half of the procedures were undertaken within the South Metropolitan region (49.1%). The hospitals contributing the largest volumes were A, B and E, together accounting for more than 60% of cases (Table 1).
Across the decade of data collection, KF and MKF were the most frequently performed procedures (Table 2). From 2013 onwards, MKF and MLF became more common, with a corresponding reduction in KF. Most operations were definitive index procedures (85.0%), with redo surgery accounting for 15.0%. SIT and OFT were more likely to be performed as secondary procedures, whereas KF, MKF and MLF were predominantly index procedures.
Table 2: Initial surgery details per SPD surgery type – categorical variablesValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s exact test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a SPD: Sacrococcygeal pilonidal sinus disease, b IVABs: Intravenous antibiotics*
Post-operative complications
The overall SSI rate was 28.8% (n = 223). OFT recorded the highest SSI rate (47.9%), while MKF had the lowest (21.9%). SIT was also strongly associated with infection. The overall WD rate was 28.4% (n = 220). OFT (39.6%) and KF (37.1%) had the highest WD rates, whereas MKF was associated with the lowest (25.2%). As SIT heals by secondary intention, these cases were excluded from the WD sub-analysis. Haematoma occurred in 8.4% (n = 65), with SIT showing the highest rate (12.2%) and MLF the lowest (2.2%). Seroma was rare, affecting only 1.4% (n = 11). A summary of post-operative complications is provided in Table 3, with additional wound-related events outlined in Table 4.
Table 3: Post-operative surgery complication details per SPD surgery typeValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s exact test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a SPD: Sacrococcygeal pilonidal sinus diseaseb Margins - n= 653, not all specimens were sent for histopathology*
Risk factors for surgical site infection
Univariate analysis demonstrated significant associations between SSI and several factors, including OFT procedures, absence of methylene blue staining, use of chlorhexidine skin preparation, operations performed in areas suspected of infection, diabetes, smoking, hirsutism and positive surgical margins. Univariate analysis, with the likelihood of SSI as the dependent variable, is presented in Table 5. However, and surprisingly, there was no significant association of SSI with obesity or re-do procedures, but they were trending towards significance (p=0.055; p=0.056), respectively (Table 5). Multivariate logistic regression confirmed that SIT and OFT independently increased SSI risk, with SIT patients six times more likely [OR 6.0, 95% CI 2.7-13.4; p < 0.001] and OFT patients three times more likely (OR 3.1, 95% CI 1.1-8.4; p = 0.027) to develop infection. Additional independent predictors included wound dehiscence [OR 50.6, 95% CI 28.7-89.5; p < 0.001], being overweight [OR 2.0, 95% CI 1.0-3.5; p=0.037] and undergoing surgery in the North Metropolitan region (OR 2.6, 95% CI 1.3-4.9; p = 0.003). Clear surgical margins were protective, reducing the risk of SSI by 60% (p = 0.002) (Figure 2).
Table 5: Univariate analysis – with the likelihood of surgical site infection (SSI) as the dependent variableValues are the number of participants (%) unless otherwise indicated.Pearson Chi-Square analysis, and Fisher’s Exact Test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a BMI: Body mass index; b IVABs: Intravenous antibiotics; c SPD: Sacrococcygeal pilonidal sinus disease
Multivariate logistic regression (N=774)Graphic logarithmic representation with the likelihood of surgical site infection as the dependent variableSIT: Secondary Intention Techniques; OFT: Other Flap Techniques
Risk factors for wound dehiscence
The overall rate of WD rate was 28.4% (n = 220). Age was significantly associated with WD, with patients aged 20-29 years (34.6%) and those over 30 years exhibiting higher rates (both 34.6%) than patients aged 15-19 years (22.9%, p = 0.030). BMI demonstrated a strong association with WD, with obese patients experiencing the highest rates (42.2%) compared to overweight (28.9%) and healthy weight individuals (24.0%, p < 0.001). Use of drains was associated with increased WD (36.8% vs 26.8%, p = 0.005), as was surgery in areas of suspected infection (60.9% vs 31.2%, p = 0.003). Chlorhexidine skin preparation was also linked with higher rates of WD than povidone-iodine (45.5% vs 29.3%, p < 0.001).
Procedure type was significant, with KF (37.1%) and OFT (39.6%) associated with higher rates than MKF (25.2%) and MLF (30.4%, p = 0.018). Comorbidities were strongly associated with WD: diabetes (62.3% vs 29.2%, p < 0.001), smoking (38.3% vs 25.7%, p < 0.001), and hirsutism (54.1% vs 24.8%, p < 0.001). Use of methylene blue was associated with lower rates of WD (26.5% vs 34.3%, p = 0.048). WD was strongly associated with SSI (85.1% vs 11.2%, p < 0.001) and with involved surgical margins (60.0% vs 26.6%, p < 0.001). Other variables, including region, gender, intravenous antibiotics, strict bed rest, wound classification, haematoma, and seroma, were not significantly associated with WD. Univariate analysis, with likelihood of WD as the dependent variable, is presented in Table 6.
Table 6: Univariate analysis – with likelihood of wound dehiscence (WD) as dependent variableValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s Exact Test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a BMI = Body Mass Index, b IVABs - Intravenous Antibiotics, c SPD - Sacrococcygeal pilonidal sinus disease*
Cox regression demonstrated that procedure type and smoking status were significant predictors of WD (Table 7; Figure 3). Compared with OFT, KF was associated with a hazard ratio (HR) of 1.78 (95% CI 1.04-3.05, p = 0.037), and MLF with a HR of 1.99 (95% CI 1.06-3.73, p = 0.031). Smoking was also independently associated with WD (HR 1.37, 95% CI 1.02-1.85, p = 0.040). Other covariates, including age, sex, BMI, diabetes, hirsutism, drain use, methylene blue use, redo procedures, and inpatient SSI, were not statistically significant in the Cox model. Hazard plots are shown in Figure 3, with regression results summarised in Table 7.
Table 7: Model covariates for wound dehiscence risk factors post definitive SPD procedure * Bolded denotes significance at p<0.05Age and BMI are continuous variables† This parameter is compared to the OFT surgical procedures which is set to zero‡ This parameter is compared to female sex which is set to zero§ This parameter is compared to “no” response which is set to zero|| This parameter is compared to NMHS region which is set to zero¶ This parameter is compared to “yes” response which is set to zeroSPD: Sacrococcygeal pilonidal sinus disease; BMI: Body Mass Index; KF: Karydakis Flap; MKF: Modified Karydakis Flap; MLF: Modified Limberg’s Rotational Flap. Due to the low frequency of Bascom’s Cleft Lift procedure (BCL), Gluteus Maximus Myocutaneous Rotational Flap (GRF), Z-plasty Flap (ZP), V-Y Advancement Flap (VY), they were grouped as Other Flap Techniques (OFT)
30-day wound dehiscence hazard function curves by SPD flap procedure groupsKF: Karydakis flap; MKF: Modified Karydakis flap; MLF: Modified Limberg Flap; OFT: Other flap TechniquesPanel A = Hazard Function for Wound Dehiscence at the mean of covariatesPanel B = Hazard Function for Wound Dehiscence for SPD Flap Procedures
Thirty-day representation and readmission
Within 30 days, 209 patients (27.0%) represented to the hospital, half of whom presented to the emergency department. KF accounted for nearly half of all re-presentations, while OFT had the highest proportional representation rate (45.0%). The most frequent reason for re-presentation was SSI, present in 49.8% of cases, most of which were superficial. Post SPD procedure 30-day re-presentation, destination and reason details are provided in Table 8.
Table 8: Post SPD procedure 30-day re-presentation, destination and reasonValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s Exact Test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a SPD - Sacrococcygeal pilonidal sinus disease, b ED = Emergency department, c GP = General Practitioner, d SSI = Surgical site infection, e WD = Wound dehiscence*
Thirty-day readmission occurred in 58 patients (7.5%). KF and MKF together accounted for nearly three-quarters of these readmissions. SSI (34.5%) and WD (31.0%) were the leading causes, while refashioning of wounds was rare. Vacuum-assisted devices used in SIT procedures also contributed to readmission, mainly due to persistently high drainage outputs. No deaths occurred during the follow-up period (Table 9).
Table 9: Post SPD Procedure SPD 30-day readmission and reasonValues are the number of participants (%) unless otherwise indicated. Pearson Chi-Square analysis, and Fisher’s Exact Test (for cell values <5), and * denotes significance at p<0.05 (indicated in bold)a SPD: Sacrococcygeal pilonidal sinus disease, b SSI: Surgical site infection, c WD: Wound dehiscence, d Vac: Negative pressure wound dressing system*
Discussion
This multi-centre cohort study is the first in Australia to evaluate surgical site complications after definitive surgery for sacrococcygeal pilonidal sinus disease incorporating both flap-based and secondary intention techniques. The study focused on SSI and WD, the most common and clinically significant complications of pilonidal surgery [12-14,16,22]. Together they account for the bulk of postoperative morbidity, contribute to hospital re-presentations and readmissions, and impose substantial demands on outpatient wound care services [10,16,18,20,21,23-26]. Their prevention therefore represents a critical benchmark for surgical quality in this field, particularly given the variability in elective surgical approaches for SPD, resulting in significantly different patient outcomes [27,28].
The overall SSI rate of 28.8% and WD rate of 28.4% observed in this cohort are striking, even when compared with the wide ranges reported internationally [10,11,16]. These complication rates are not trivial; both SSI and WD can delay healing by weeks or months, prolonging the requirement for dressings and hospital-in-the-home services, and significantly impact patient wellbeing and productivity. In the context of SPD, where the disease predominantly affects young working adults, the socioeconomic burden of prolonged recovery is considerable. The strong correlation between SSI and WD demonstrated in this study further underscores their clinical importance, as infection and breakdown often coexist, compounding morbidity.
This analysis identified both patient-level and procedural determinants of SSI and WD. On multivariate modelling, secondary intention and other complex flap techniques were independently associated with higher SSI rates, with SIT conferring a six-fold risk and OFT a three-fold risk compared with MKF. WD, meanwhile, was most strongly associated with KF and MLF procedures, as confirmed by Cox regression (Table 7; Figure 3). Patient-related factors also exerted a significant influence. Obesity, diabetes, smoking and hirsutism emerged as consistent predictors of both SSI and WD, highlighting the contribution of systemic and local host factors to wound healing. The interplay between infection, involved surgical margins and dehiscence further reinforces the concept that meticulous operative technique and patient optimisation are crucial in reducing surgical site occurrences.
The importance of surgical margins warrants particular attention. Incomplete excision was associated with higher rates of both SSI and WD, while clear margins were protective. This finding aligns with surgical principles but is particularly relevant in SPD, where disease extent is sometimes difficult to define intraoperatively. Ensuring wide and complete resection may be as important as the choice of closure technique in preventing complications. Similarly, the protective association observed with methylene blue staining suggests that adjunctive measures to aid visualisation of sinus tracts may improve surgical completeness and reduce postoperative morbidity.
Among the procedures compared, the MKF consistently demonstrated the most favourable outcomes across both SSI and WD, supporting its role as the preferred option for elective definitive surgery. However, it should be recognised that even MKF was associated with clinically significant complication rates. Conversely, secondary intention techniques were associated with unacceptably high rates of SSI and re-presentation, yet they remain a pragmatic option when infection precludes safe primary closure. These findings reinforce the principle that no single procedure is universally applicable; rather, outcomes are optimised when patient risk factors, disease complexity and intraoperative findings are integrated into a shared decision-making framework.
Readmissions and re-presentations provide an important measure of the broader healthcare impact of SPD surgery, and in this study, they were predominantly driven by wound-related complications. Within 30 days, 27% of patients re-presented, most often to the emergency department or outpatient clinics, and 7.5% required readmission. SSI accounted for more than one-third of readmissions, while WD contributed to nearly one-third, with a substantial overlap between the two. Secondary intention techniques were associated with the highest readmission rates, whereas modified flap procedures, particularly the MKF, had comparatively lower but still clinically significant representation rates. These findings underline that SSI and WD are not only immediate postoperative complications but also major drivers of hospital resource use, influencing both early re-presentations and readmissions.
This study has several limitations. Its retrospective design relied on administrative and clinical records, with potential for data entry errors and incomplete documentation. Surgical technique was heterogeneous, with variation in flap design, closure method, drain use and perioperative management not consistently captured, limiting the precision of comparisons between techniques. Some procedures, particularly those grouped as other flap techniques, were under-represented, preventing analysis of individual outcomes for Bascom cleft lift, gluteus maximus myocutaneous flap, Z-plasty and V-Y advancement. While data were collected over a prolonged period, extended follow-up was not available for all patients, and recurrence data were incomplete, with late complications possibly under-estimated if patients presented outside the study hospitals. Patient-reported outcomes such as pain, cosmesis and quality of life were not available. Finally, findings are limited to the public healthcare system, which may not reflect private practice. However, review of the complete state data linkage record, including both public and private hospitals, confirmed that more than 85% of elective SPD procedures were conducted in the public sector, suggesting that the findings are broadly representative of overall practice.
Despite these limitations, the study provides important insights. SSI and WD remain common and burdensome complications after SPD surgery, with both patient-level and procedural factors influencing risk. Modified flap procedures, particularly the MKF, offer the most balanced outcomes but do not eliminate the problem. These findings highlight the need for structured training and upskilling to improve operative consistency, optimisation of modifiable patient factors, and continued refinement of surgical techniques. Future prospective studies should place SSI and WD at the centre of outcome reporting, with longer follow-up and inclusion of patient-centred metrics to fully capture the burden of these complications.
The principal strength of this study lies in its comprehensive representation of contemporary surgical practice, combined with long-term follow-up of all patients to capture genuine long-term outcomes. Recognising that some patients may not return to their index centre for complication management, as reported in previous studies, this study employed triangulation of follow-up data across multiple sources to achieve a more accurate and complete depiction of outcomes.
Conclusions
SSI and WD are the most frequent and burdensome complications following definitive surgery for sacrococcygeal pilonidal disease. This study identified key patient-level risk factors, including obesity, diabetes, smoking and hirsutism, as well as procedural determinants such as incomplete margins and closure technique. Clear margins were protective, and the MKF demonstrated the most favourable overall risk profile, whereas secondary intention and other complex flaps were associated with higher complication rates. SSI and WD were also the predominant causes of 30-day re-presentations and readmissions, confirming their central role in hospital utilisation and patient morbidity. These findings reinforce the importance of optimising modifiable risk factors, refining operative techniques, and promoting structured training to reduce variation in practice. Future prospective studies should prioritise SSI and WD as key outcomes, with long-term follow-up to define their contribution to recurrence and the overall healthcare burden.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patient characteristics and symptoms in chronic pilonidal sinus disease Int J Colorectal Dis Søndenaa K Andersen E Nesvik I Søreide JA 3942101995774532210.1007/BF 00337585 · doi ↗ · pubmed ↗
- 2Pilonidal disease Surg Clin North Am Hull TL Wu J 116911858220021251684610.1016/s 0039-6109(02)00062-2 · doi ↗ · pubmed ↗
- 3Pilonidal disease Clin Colon Rectal Surg Khanna A Rombeau JL 46532420112237940510.1055/s-0031-1272823 PMC 3140333 · doi ↗ · pubmed ↗
- 4Incidence and aetiological factors in pilonidal sinus among Turkish soldiers Eur J Surg Akinci OF Bozer M Uzunköy A Düzgün SA Coşkun A 33934216519991036583510.1080/110241599750006875 · doi ↗ · pubmed ↗
- 5ABC of colorectal diseases. Pilonidal sinus BMJ Jones DJ 4104123051992139292610.1136/bmj.305.6850.410PMC 1883113 · doi ↗ · pubmed ↗
- 6Pilo-Nidal sinus Boston Med Surg J Hodges RM 4854861031880
- 7Pilonidal cyst: cause and treatment Dis Colon Rectum da Silva JH 114611564320001095001510.1007/BF 02236564 · doi ↗ · pubmed ↗
- 8Common surgical procedures in pilonidal sinus disease: a meta-analysis, merged data analysis, and comprehensive study on recurrence Sci Rep Stauffer VK Luedi MM Kauf P 3058820182944954810.1038/s 41598-018-20143-4PMC 5814421 · doi ↗ · pubmed ↗