Electroencephalography in the Intensive Care Unit: Experience of the Department of Functional Neurosensory Explorations at Gonesse Hospital, France
Idrissa Doumbouya, Karinka Diawara, Elian Hapca, Djénabou Négué Barry, Mohamed Traoré, Gabriela Carelli, Oumar Sylla, Andreea Stanciulescu, Fodé Abass Cissé

TL;DR
This study evaluates how EEG is used in ICU settings to assess neurological conditions and predict patient outcomes.
Contribution
The study provides insights into the clinical utility and prognostic value of EEG in ICU patients.
Findings
EEG was primarily used for neuroprognostic evaluation and seizure assessment in ICU patients.
Epileptic abnormalities were common and correlated with conditions like status epilepticus and ischemic stroke.
Poor prognosis was linked to EEG features like absence of reactivity and burst suppression.
Abstract
Introduction: The aim of this study was to evaluate the indications and outcomes of electroencephalography (EEG) in the intensive care unit (ICU), as well as to assess their prognostic values in adults. Materials and methods: We conducted a two-year retrospective study from November 2022 to October 2024 in the Department of Functional Neurosensory Explorations at Gonesse Hospital, involving patients hospitalized in the ICU. Sociodemographic, clinical, electroencephalographic, and prognostic variables were collected. During data analysis, we investigated EEG patterns associated with poor prognosis and epileptic abnormalities. Results: A total of 76 participants met our selection criteria, with a mean age of 61 ± 18.8 years and a predominance of men (sex ratio: 1.92). The main indications for EEG were neuroprognostic evaluation in 53 patients (68.5%), seizure assessment in 32 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
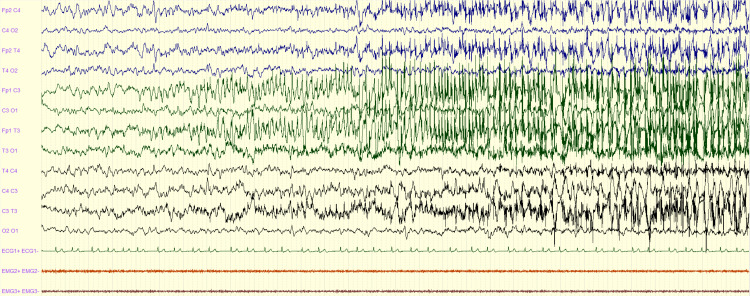 Figure 1
Figure 1 Figure 2
Figure 2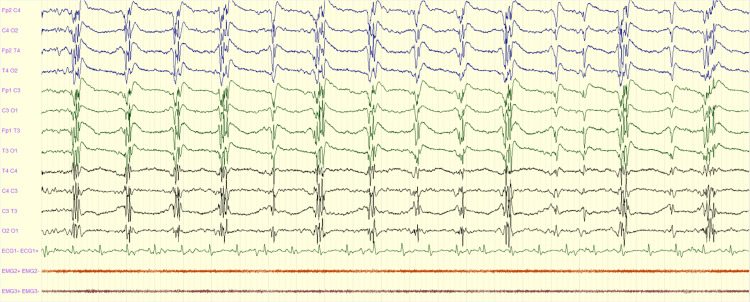 Figure 3
Figure 3 Figure 4
Figure 4| Variables | Number (n = 76) | Proportion (%) | |
| Reasons for performing an EEG | |||
| Search for epileptic seizures | 32 | 40.8 | |
| Neuroprognosis assessment | 53 | 68.5 | |
| Unexplained neurological deterioration | 4 | 5.3 | |
| Reasons for admission to the ICU | |||
| Cardiorespiratory arrest | 29 | 38.2 | |
| Ischemic stroke | 13 | 17.1 | |
| Status epilepticus | 11 | 14.5 | |
| Septic shock | 10 | 13.2 | |
| Confusion | 9 | 11.8 | |
| Cerebral hemorrhage | 4 | 5.3 | |
| Comorbidities | |||
| Hypertension | 33 | 43.4 | |
| Heart disease | 22 | 28.9 | |
| Diabetes | 19 | 25 | |
| Dyslipidemia | 13 | 17.1 | |
| Stroke | 8 | 10.5 | |
| Psychiatric disorders | 7 | 9.2 | |
| None | 6 | 7.9 | |
| Epilepsia | 6 | 7.9 | |
| Neoplasia | 5 | 6.6 | |
| Alcoholism | 4 | 5.3 | |
| Renal insufficiency | 4 | 5.3 | |
| Smoking | 3 | 3.9 | |
| HIV | 3 | 3.9 | |
| Others | 3 | 3.9 | |
| Variables | Number | Proportion (%) |
| Generalized slow waves | 63 | 82.9 |
| Focal slow waves | 27 | 35.5 |
| Generalized periodic activities | 15 | 19.7 |
| Burst suppression | 11 | 14.5 |
| Epileptic activity | 43 | 56.6 |
| Electrographic seizures | 18 | 23.7 |
| Non-specific interictal activity | 10 | 13.2 |
| NCSE | 8 | 10.5 |
| LPDs | 7 | 9.2 |
| Absence of cerebral activity | 7 | 9.2 |
| Normal | 2 | 2.6 |
| Coma alpha pattern | 1 | 1.3 |
| Variables | Epileptic abnormalities (%) | Total | χ2 | P-value | |
| Yes | No | ||||
| Cardiorespiratory arrest | 11 (37.9) | 18 (62.1) | 29 | 0.7725 | 0.3794 |
| Status epilepticus | 11 (100) | 0 | 11 | 12.6344 | 0.0003 |
| Ischemic stroke | 10 (76.9) | 3 (23.1) | 13 | 4.6100 | 0.0317 |
| Septic shock | 2 (20) | 8 (80) | 10 | 0.8448 | 0.3580 |
| Confusion | 6 (66.7) | 3 (33.3) | 9 | 0.9318 | 0.3343 |
| Abnormal brain imaging | 30 (56.6) | 23 (43.5) | 46 | 4.1289 | 0.0421 |
| Variables | Death, n (%) | Total | χ2 | P-value | |
| Yes | No | ||||
| Sedation | 13 (48.2) | 14 (51.8) | 27 | 0.8159 | 0.3663 |
| Number of anti-seizure medications | |||||
| 1-2 | 9 (37.5) | 15 (62.5) | 24 | 5.8442 | 0.01562 |
| 3-5 | 9 (90) | 1 (10) | 10 | ||
| Abnormal brain imaging | 23 (47.9) | 25 (52.1) | 48 | 4.6361 | 0.0175 |
| Nonreactive EEG | 25 (58.1) | 18 (41.9) | 43 | 17.2538 | 0.0001 |
| Epileptic abnormalities | 14 (40) | 21 (60) | 27 | 0.0834 | 0.7727 |
| Burst suppression | 9 (90.9) | 1 (9.1) | 11 | 13.5553 | 0.0002 |
| Absence of cerebral activity | 6 (85.7) | 1 (14.3) | 7 | 5.7700 | 0.0163 |
| Generalized slow waves | 21 (53.9) | 42 (46.1) | 63 | 1.1669 | 0.2800 |
| Focal slow waves | 12 (44.4) | 15 (55.6) | 27 | 0.5951 | 0.4404 |
| Generalized periodic activities | 5 (30.8) | 10 (69.2) | 15 | 0.0334 | 0.7571 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpilepsy research and treatment · Intensive Care Unit Cognitive Disorders · Traumatic Brain Injury and Neurovascular Disturbances
Introduction
Electroencephalography (EEG) visualizes brain activity by detecting differences in electrical potential between electrodes placed on the scalp over time, to aid in the diagnosis, management, and prognosis of brain pathologies [1]. EEG analysis, which traditionally relies on visual reading and clinically oriented interpretation by qualified physicians, plays an important role, from the quality control of the recording to advanced EEG interpretation [1]. In intensive care, EEG monitoring is an effective surveillance tool for detecting and characterizing epileptic seizures, assessing the severity of encephalopathy, evaluating sedation levels, and aiding prognosis [2]. It also plays a role in the detection and management of non-convulsive seizures (NCS) and non-convulsive status epilepticus (NCSE) [3], monitoring of neurosurgical patients, and classification of paroxysmal clinical events [4-6]. Recognizing epileptic seizures in the intensive care unit (ICU) is essential due to their impact on morbidity and mortality, as well as the risk of developing epilepsy following acute symptomatic events [7]. However, the use of EEG in the ICU presents challenges, particularly regarding the interpretation of results, which can be affected by patient sedation and artifacts inherent to the intensive care environment. While there is a growing body of literature describing EEG practices in academic hospital ICUs, little is known about EGG utilization patterns, diagnostic yield, and clinical impact in non-academic centers where resource limitations and staffing models may differ substantially [8]. Addressing this knowledge gap is essential to guide the rational implementation of EEG monitoring and improve timely seizure detection and the accessibility of neurodiagnostic care. Therefore, the aim of this study was to evaluate the indications and outcomes of EEG in the ICU at a general hospital in the suburb of Paris, as well as to assess their prognostic value in adults.
Materials and methods
We conducted a two-year retrospective study from November 2022 to October 2024 in the Department of Functional Neurosensory Explorations at Gonesse Hospital. The department operates from Monday to Friday during standard working hours (50 hours/week) and is equipped to perform EEG recordings at night when necessary. EEG recordings were performed using a BRAIN QUICK system (Natus Medical Incorporated, Middleton, WI) equipped with analysis and reporting software and an SD PLUS amplifier, both of which were used throughout this study. Recordings were carried out by qualified nurses in accordance with the international 10-20 electrode placement system and in compliance with French national EEG guidelines [9]. EEGs were examined and pre-analyzed by a trained neurologist and then reinterpreted and validated by a neurophysiologist to ensure consistent and rigorous interpretation.
We included all EEGs conducted on comatose patients admitted to the ICU. Patients under 18 years of age, as well as those with missing critical data, particularly regarding EEGs or essential clinical variables, were excluded. For each patient, the following data were collected.
Sociodemographic data included patient age and sex. Clinical data encompassed the reason for ICU admission, associated comorbidities, and the indication for EEG. Patients were classified based on whether or not they had experienced seizures, and the type of seizure was recorded.
EEG recordings were performed intermittently on all patients by the same technical team. EEG findings were categorized as either epileptic or non-epileptic. Seizure diagnosis during EEG was based on the criteria established by Chong and Hirsch [10]. Rhythmic and periodic patterns, including lateralized periodic discharges (LPDs) and generalized periodic discharges (GPDs), were defined according to the American Clinical Neurophysiology Society (ACNS) Standardized Critical Care EEG Terminology: 2021 version [11]. Non-convulsive status epilepticus (NCSE) was defined using the Salzburg criteria [12]. Other EEG patterns were classified as normal, slowed, or inactive. EEG duration was calculated by summing the total recording time for each patient. The use of anti-seizure medications was also documented.
Brain imaging findings were classified as either normal or abnormal, and patient outcomes, including mortality, were recorded.
The data were extracted from the electronic medical records of comatose patients admitted to the ICU, including clinical records and EEG results obtained during their hospitalization. Cases of missing data were systematically noted. To ensure the quality of the data collected, regular checks were performed on a random sample of medical records, and audits were conducted to detect any inconsistencies or missing important data.
All data were anonymized to protect confidentiality in accordance with the principles of the Declaration of Helsinki. The study has been approved by the local ethics committee.
Data analysis was performed using Epi Info™ version 7.1, a database and statistical software developed by the Centers for Disease Control and Prevention (CDC, Atlanta, GA). Quantitative variables were expressed as means, and qualitative variables were presented as frequencies and numbers. Comparisons between qualitative variables were made using the chi-square test (a nonparametric test), while comparisons between quantitative variables were performed using Student’s t-test (a parametric test). A p-value of less than 0.05 was considered statistically significant.
Results
Out of a total of 3,900 patients who underwent EEG in the department, 77 patients were from the intensive care unit. One patient was under 18 years of age and was therefore excluded, resulting in a final sample of 76 participants, representing 1.9% of all EEGs performed.
The overall mean age was 61 ± 18.8 years, with a median of 63 years and extremes of 18 and 100 years. The mean age was 62 for women and 60 for men. There was a predominance of men, with a sex ratio of 1.92 (50 men versus 26 women). There was no statistically significant difference between age and sex (p = 0.7382).
The main indications for EEG were neuroprognostic assessment in 53 patients (68.5%), search for seizures in 32 patients (40.8%), and unexplained neurological deterioration in four patients (5.3%).
Reasons for admission to the intensive care unit were cardiorespiratory arrest in 29 patients (38.2%), ischemic stroke in 13 patients (17.1%), status epilepticus in 11 patients (14.5%), septic shock in 10 patients (13.2%), confusion in nine patients (11.8%), and cerebral hemorrhage in four patients (5.3%). Hypertension was the most common comorbidity, found in 33 patients (43.4%); other comorbidities were dominated by heart disease in 22 patients (28.9%), diabetes in 19 patients (25%), dyslipidemia in 13 patients (17.1%), stroke in eight patients (10.5%), and psychiatric disorders in seven patients (9.2%) (Table 1).
Clinically, 17 patients (22.4%) experienced seizures. Among them, six patients (7.9%) had generalized seizures, five patients (6.6%) had focal seizures with secondary bilateralization, three patients (3.9%) had focal seizures without bilateralization, and three patients (3.9%) had seizures of unknown onset.
In total, 34 patients (44.7%) had received at least one anti-seizure medication prior to EEG recording.
The mean EEG duration was 50 minutes, with a range from 20 to 1,420 minutes. In terms of electroencephalographic findings (Table 2), epileptic abnormalities were observed in 43 patients (56.6%). These included electrographic seizures in 18 patients (23.7%), non-specific interictal activity in 10 patients (13.2%), NCSE in eight patients (10.5%), and LPDs in seven patients (9.2%). These findings accounted for 41.9%, 23.3%, 18.6%, and 16.3% of the epileptic abnormalities, respectively.
Among non-epileptic abnormalities, the most frequent patterns were generalized slow waves in 63 patients (82.9%), focal slow waves in 27 patients (35.5%), generalized periodic discharges in 15 patients (19.7%), and burst-suppression patterns in 11 patients (14.5%) (Figures 1-4).
Left focal seizure with bilateralization: EEG showing left frontal rhythmic spikes with secondary bilateralizationEEG: electroencephalography
NCSE: generalized rhythmic epileptiform discharges after non-status epilepticusNCSE: non-convulsive status epilepticus
Generalized periodic activity: EEG showing periodic polyspikes in a patient with post-anoxic coma following cardiac arrestEEG: electroencephalography
EEG showing a burst-suppression pattern in a patient after post-anoxic encephalopathyEEG: electroencephalography
Fifty-three patients (69.7%) had abnormal brain imaging findings, with anoxic-ischemic lesions accounting for 19 patients (25%). Other brain abnormalities were infarctions in 13 patients (17.1%), cerebral edema in 12 patients (15.8%), and intracranial hemorrhage in nine patients (11.8%).
A statistically significant correlation was found between epileptic EEG abnormalities and the status epilepticus (p = 0.0003), ischemic stroke (p = 0.0317), and abnormal brain imaging (p = 0.0421) (Table 3).
A total of 28 patients (36.8%) died during the study period. Several factors were significantly associated with poor prognosis, including the use of more than two anti-seizure medications (p = 0.0156), the absence of EEG reactivity (p = 0.0001), burst-suppression pattern on EEG (p = 0.0002), and the absence of cerebral activity (p = 0.0163) (Table 4).
Discussion
The use of EEG in the ICU represents a significant advancement in the management of comatose or neurologically unstable patients, allowing for the early detection of seizures that may go clinically unnoticed. We conducted a 24-month retrospective study of EEG monitoring in the ICU setting. However, this study has several limitations. These include its retrospective design, a relatively small sample size that may limit statistical power, and the generalizability of the findings to other institutions. Additionally, the lack of systematic long-term EEG monitoring may have led to the underdetection of delayed or intermittent abnormalities.
There is a substantial body of literature on EEG monitoring in the ICU. However, in non-academic hospitals such as ours, where resources may be more limited and expertise in neurophysiology less readily available, the implementation of EEG monitoring in the ICU remains a challenge.
The prevalence of clinical seizures (22.4%) found in our study is consistent with the literature, where the reported prevalence of seizures in ICU patients varies widely, ranging from 7% to 47% depending on the study population and center [13,14]. Reported rates of non-convulsive status epilepticus (NCSE) also vary considerably, from 1% to 32% [13]. Claassen et al. demonstrated that nearly 90% of seizures in comatose ICU patients are non-convulsive and therefore would not be detected without EEG monitoring, highlighting the essential role of EEG in this setting [14]. The seizure frequency observed in our study may be partly explained by the relatively short duration of EEG recordings, which averaged 50 minutes, and by the use of anti-seizure medications. In practice, treatment decisions regarding anti-seizure medications are often made in real time, based on clinical suspicion, and do not necessarily wait for EEG confirmation. This practice could account for the relatively high proportion of patients (44.7%) who received at least one anti-seizure medication prior to EEG.
Epileptic abnormalities were identified in 43 patients (56.6%). Among them, electrographic seizures were observed in 18 patients (41.9%), followed by non-specific interictal activity in 10 patients (23.3%), LPDs in seven patients (16.3%), and non-convulsive status epilepticus (NCSE) in eight patients (18.6%). Claassen et al. reported an 18% frequency of electrographic seizures, and periodic epileptiform discharges were recorded in 19% of patients (LPDs, 13%; GPDs, 6%) [15]. In many patients with convulsive status epilepticus (CSE), electrographic seizures may persist even after convulsive activity has ceased [16]. In the Veterans Affairs Cooperative Study, Treiman et al. reported that patients who developed NCSE following convulsive status epilepticus (CSE) had more than twice the mortality compared to those whose seizures had completely ceased [17]. Similarly, in a prospective study, DeLorenzo et al. found that 48% of patients monitored by EEG for 24 hours after the resolution of CSE experienced non-convulsive seizures, and 14% developed NCSE [18].
Another common indication for EEG monitoring was neuroprognostic evaluation. Standard EEG, continuous EEG, and evoked potentials (particularly somatosensory evoked potentials) are frequently used to assess prognosis in cases of suspected irreversible neuronal damage [5]. In our study, non-epileptic EEG abnormalities were predominantly characterized by generalized slow waves, followed by focal slow waves, generalized periodic discharges, and burst-suppression patterns. Young and Mantia described a series of EEG changes correlated with various markers of multi-organ failure [19]. The initial abnormalities involved slowing in the theta range (>4 but <8 Hz), followed by delta activity (≤4 Hz), which progressed from intermittent and rhythmic to continuous and arrhythmic patterns. These were followed by the appearance of triphasic waves and, ultimately, a burst-suppression pattern. As in our study, their findings demonstrated a strong and nearly linear correlation between EEG deterioration and increased mortality.
Poor prognostic EEG factors were the lack of reactivity (p = 0.0001), burst-suppression patterns (p = 0.0002), anti-seizure medications exceeding two (p = 0.0156), and the lack of brain activity (p = 0.0163). In another study, Young et al. reported that in anoxic-ischemic encephalopathy, certain EEG patterns are strongly predictive of poor outcomes, with patients failing to regain consciousness and either remaining in a vegetative state or dying without recovery [20]. These patterns include the absence of cerebral activity, burst suppression with generalized epileptiform activity in bursts, and periodic generalized epileptiform discharges on a background of cerebral inactivity [20]. The severe outcomes correlated with burst suppression and complete electrocerebral inactivity in our study emphasize the necessity of EEG evaluation for accurate prognostication in such patients. In addition, other authors have reported that the absence of EEG reactivity to stimulation (defined as a lack of change in amplitude or frequency following a stimulus) also holds significant prognostic value and is associated with increased mortality or severe disability in most cases [21,22].
Conclusions
EEG monitoring in the intensive care setting provides valuable insights into both the epileptic nature of coma and patient prognosis. In our study, a significant number of electrographic seizures went undetected clinically, which strongly supports the need for implementing continuous EEG monitoring even in peripheral or non-academic centers. Such monitoring can improve seizure detection, guide treatment decisions, and potentially improve patient outcomes. However, our study had limitations, including its retrospective design and relatively short EEG recording durations. Future studies should incorporate additional factors such as the degree of sedation, anti-seizure medication dosages, and extending continuous EEG monitoring beyond 24 hours. These investigations would offer a more comprehensive understanding of continuous EEG utility in the ICU setting, tailored to the specific constraints and resources of centers similar to ours.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Electroencephalogram in the intensive care unit: a focused look at acute brain injury Intensive Care Med Alkhachroum A Appavu B Egawa S 144314624820223599779210.1007/s 00134-022-06854-3PMC 10008537 · doi ↗ · pubmed ↗
- 2Continuous EEG monitoring in the intensive care unit Curr Neurol Neurosci Rep Kennedy JD Gerard EE 4194281220122265363910.1007/s 11910-012-0289-0 · doi ↗ · pubmed ↗
- 3Prevalence of nonconvulsive status epilepticus in comatose patients Neurology Towne AR Waterhouse EJ Boggs JG Garnett LK Brown AJ Smith JR Jr De Lorenzo RJ 3403455420001066869310.1212/wnl.54.2.340 · doi ↗ · pubmed ↗
- 4Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring J Neurosurg Vespa PM Nuwer MR Nenov V 7507609119991054123110.3171/jns.1999.91.5.0750 PMC 4347935 · doi ↗ · pubmed ↗
- 5Early prediction of delayed cerebral ischemia in subarachnoid hemorrhage based on quantitative EEG: a prospective study in adults Clin Neurophysiol Gollwitzer S Groemer T Rampp S 1514152312620152550019310.1016/j.clinph.2014.10.215 · doi ↗ · pubmed ↗
- 6Nonconvulsive seizures after subarachnoid hemorrhage: multimodal detection and outcomes Ann Neurol Claassen J Perotte A Albers D 53647420132381394510.1002/ana.23859 PMC 3775941 · doi ↗ · pubmed ↗
- 7Continuous electroencephalography in the critically ill: clinical and continuous electroencephalography markers for targeted monitoring J Clin Neurophysiol Newey CR Kinzy TG Punia V Hantus S 3253313520182967701410.1097/WNP.0000000000000475 · doi ↗ · pubmed ↗
- 8Analysis of routine EEG usage in a general adult ICU Ir J Med Sci Mc Hugh JC Downey T Murphy RP Connolly S 26326617820091929614510.1007/s 11845-009-0317-5 · doi ↗ · pubmed ↗