Trichoscopic Differentiation in Alopecia: Retrospective Case Series Comparing Lichen Planopilaris, Discoid Lupus Erythematosus, and Alopecia Areata
Gökhan Kaya

TL;DR
This study compares trichoscopic features of three types of alopecia to help distinguish scarring from nonscarring hair loss.
Contribution
It identifies distinct trichoscopic markers for alopecia areata versus scarring alopecias like lichen planopilaris and discoid lupus.
Findings
Exclamation-mark hairs and yellow dots are specific to alopecia areata.
Follicular ostia loss and white scarring are seen in lichen planopilaris and discoid lupus.
These markers allow practical differentiation between nonscarring and scarring alopecias.
Abstract
This single-center retrospective case series included 28 patients with alopecia (7 with lichen planopilaris, 7 with discoid lupus erythematosus, and 14 with alopecia areata). Trichoscopic markers were systematically compared across groups. Exclamation-mark hairs and yellow dots were characteristic of alopecia areata, whereas follicular ostia loss and white scarring were confined to lichen planopilaris/discoid lupus erythematosus, providing a simple and practical distinction between nonscarring and scarring alopecias in routine practice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
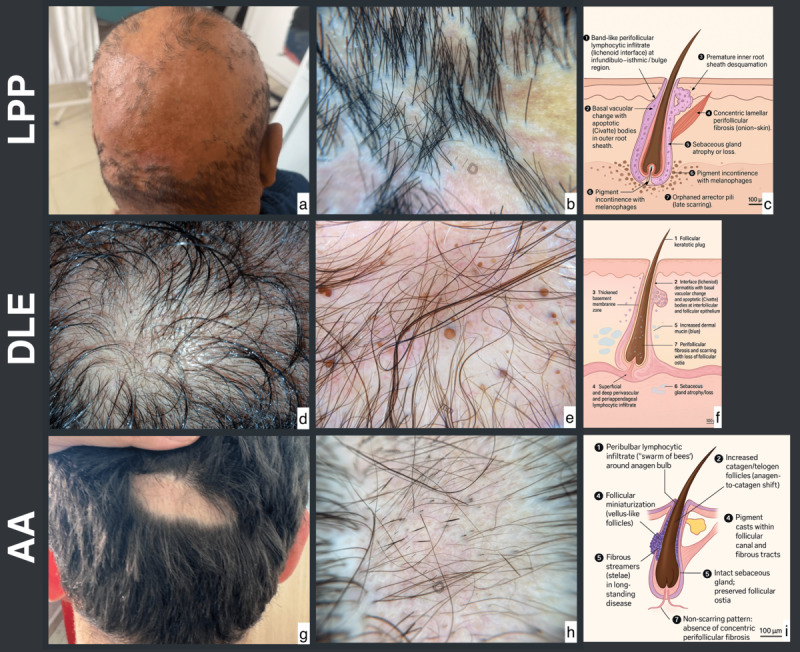 Figure 1
Figure 1| Variable | LPP | DLE | AA (n=14) | OR (AA vs scarring | |
|---|---|---|---|---|---|
| Age (years), mean (SD) | 34.4 (10.3) | 40.3 (6.6) | 37.7 (6.4) | – | – |
| Female participant, n (%) | 3 (43) | 2 (29) | 5 (36) | – | – |
| White scarring or atrophy, n (%) | 7 (100) | 7 (100) | 0 (0) | <0.01 | <.001 |
| Follicular ostia loss, n (%) | 7 (100) | 7 (100) | 0 (0) | <0.01 | <.001 |
| Exclamation-mark hairs, n (%) | 0 (0) | 0 (0) | 11 (79) | 95.29 | <.001 |
| Yellow dots, n (%) | 0 (0) | 2 (29) | 10 (71) | 15.00 | .006 |
| Black dots, n (%) | 0 (0) | 3 (43) | 7 (50) | 3.67 | .237 |
| Broken hairs, n (%) | 4 (57) | 2 (29) | 8 (57) | 1.78 | .706 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHair Growth and Disorders · Dermatology and Skin Diseases · Systemic Sclerosis and Related Diseases
Introduction
Trichoscopy is now integral to alopecia assessment, enabling the recognition of hair‐shaft changes, peri or interfollicular alterations, and follicular opening loss to quickly separate nonscarring from scarring disease [1]. In scarring alopecias, lichen planopilaris (LPP) typically shows perifollicular scales or erythema and target-pattern blue-gray dots, whereas discoid lupus erythematosus (DLE) more often displays follicular keratotic plugs with telangiectatic or arborizing vessels; patterns can vary by phototype, underscoring the need for pragmatic rules that generalize across populations [23]. The misclassification between LPP and DLE is well documented, emphasizing the value of simple bedside discriminators that complement histopathology [4].
This study, therefore, aimed to compare key trichoscopic markers among LPP, DLE, and AA and to propose a concise, rule-in/rule-out approach for routine clinical care.
Methods
Setting and Participants
This single-center, retrospective case series was conducted at the Department of Dermatology, Nizip State Hospital, Gaziantep, Türkiye, including consecutive patients with alopecia who underwent trichoscopic evaluation: LPP (n=7), DLE (n=7), and AA (n=14). The diagnosis of AA was made based on clinical and trichoscopic criteria, whereas all LPP and DLE cases were histopathologically confirmed. Age and sex were retrieved from medical records.
Trichoscopic Evaluation
Routine polarized dermoscopy images were reviewed using a prespecified 16-item checklist (present=1/absent=0), including perifollicular scale, erythema, and casts; blue-gray target dots; follicular ostia loss or plugs; yellow and black dots; white scar or atrophy; background erythema; arborizing vessels; interfollicular scales; exclamation-mark, broken, and lonely hairs; and tufting.
Arborizing vessels were graded by caliber (0=absent, 1=thin <50% of adjacent hair-shaft caliber, 2=thick ≥50% of adjacent hair-shaft caliber).
Statistical Analysis
Categorical variables were summarized as n (%) and continuous variables as mean (SD). Prespecified contrasts used two-sided Fisher exact tests (α=.05): AA versus scarring alopecias (LPP+DLE) for exclamation-mark hairs, yellow dots, white scarring or atrophy, and follicular ostia loss (plus exploratory black or broken hairs), and DLE versus LPP for follicular plug, arborizing vessels (any/thick), interfollicular scale, and peripilar casts.
Odds ratios were estimated with a Haldane–Anscombe 0.5 correction when zero cells occurred. Analyses were performed using Python and SciPy.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was granted by the Scientific Research Ethics Committee of Bezmialem Vakıf University, Istanbul, Türkiye (Approval No: E-54022451-050.04-122609; September 6, 2023). The protocol originally focused on AA; additional LPP and DLE cases collected under the same protocol were analyzed here as a secondary evaluation, with notification to the ethics committee. All participant data were anonymized and deidentified before analysis. Owing to the retrospective design and use of anonymized data, informed consent was not required. No compensation was offered to study participants.
Results
Twenty-eight patients were included (7 each with LPP and DLE, and 14 with AA); age and sex distributions were comparable. Scarring signs (white scar or atrophy and follicular ostia loss) occurred exclusively in LPP/DLE and were absent in AA. Trichoscopic markers clustered in AA, most prominently exclamation-mark hairs, followed by yellow dots, whereas black dots and broken hairs were not discriminatory. Within scarring alopecias, DLE showed more follicular plugs and occasional thick arborizing vessels, while LPP showed universal perifollicular scale with more perifollicular erythema; these trends were not statistically significant given the sample size. Representative clinical, trichoscopic, and histopathological findings for each entity are illustrated in Figure 1. All estimates and exact P values are provided in Table 1.
Clinical, trichoscopic, and histopathological features of LPP, DLE, and AA. (A–C) LPP: Patchy scarring alopecia with perifollicular scales or erythema and blue-gray dots; histology illustration (C) Perifollicular lichenoid infiltrate, lamellar fibrosis, sebaceous loss, and pigment incontinence. (D–F) DLE: Scarring alopecia with keratotic plugs, erythema, and arborizing vessels; schematic drawing (F) Follicular plugging, thickened basement membrane zone, dermal mucin, and perifollicular fibrosis with ostial loss. (G–I) AA: Nonscarring alopecia with yellow or black dots and exclamation-mark hairs; histopathologic illustration (I) Peribulbar “swarm of bees” infiltrate, follicular miniaturization, preserved sebaceous glands, and absence of concentric fibrosis. All clinical and trichoscopic images are original and de-identified; schematic histologic illustrations (C, F, I) were created by the authors for this figure to depict key diagnostic features. AA: alopecia areata; DLE: discoid lupus erythematosus; IRS: inner root sheath; LPP: lichen planopilaris.
Discussion
Principal Findings
This study identified key trichoscopic patterns that reliably distinguish nonscarring from scarring alopecias. In this cohort, white scarring or atrophy and follicular ostia loss occurred exclusively in LPP or DLE and were absent in AA, reinforcing that the loss of follicular openings is a practical hallmark of cicatricial disease [5]. Conversely, AA showed clusters of exclamation-mark hairs and, secondarily, yellow dots; these markers also track AA activity and severity in structured trichoscopic scoring systems such as STRIAA (Severity Trichoscopy Index Alopecia Areata) and support their use as practical rule-in signs [6].
Among scarring alopecias, the findings of this study were consistent with those in previous reports [378]: DLE showed more follicular plugs and occasional thick arborizing vessels, whereas LPP consistently demonstrated perifollicular scale, frequent erythema, and characteristic target-pattern blue-gray dots [378]. Notably, lonely hair is not disease-specific and should be interpreted in context, particularly when differentiating LPP from frontal fibrosing alopecia [7].
Clinically, a succinct rule emerges: AA is favored by one or more of exclamation-mark hairs or yellow dots, whereas the combination of ostia loss and white scarring favors LPP or DLE. This aligns with stepwise diagnostic algorithms that first classify distribution, then scarring status by the presence or absence of ostia, and finally apply a short list of trichoscopic clues [9]. Comparative clinicopathologic studies also demonstrate systematic differences between DLE and LPP at the population level, providing additional context for our observations [10].
Key limitations include the small, single-center sample and limited power for LPP–DLE contrasts. Nevertheless, the direction and magnitude of the observed effects and the identified high-yield markers are consistent with contemporary systematic reviews [3] and support the external validity of the findings of this study.
Conclusions
A minimalist trichoscopic rule effectively differentiates AA from scarring alopecias: exclamation-mark hairs or yellow dots favor AA, whereas the combination of follicular ostia loss and white scarring favors LPP or DLE. These easily recognizable cues can assist clinicians in biopsy site selection and treatment planning. Larger multicenter studies are warranted to validate these findings and refine diagnostic criteria for distinguishing LPP from DLE.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pirmez R The dermatoscope in the hair clinic: trichoscopy of scarring and nonscarring alopecia J Am Acad Dermatol Aug 2023892 SS 9S 15doi 10.1016/j.jaad.2023.04.033Medline 37591567 · doi ↗ · pubmed ↗
- 2Khare S Behera B Ding DD et al Dermoscopy of hair and scalp disorders (trichoscopy) in skin of color - a systematic review by the International Dermoscopy Society “Imaging in Skin of Color” Task Force Dermatol Pract Concept Oct 12023134 S 1e 2023310 Sdoi 10.5826/dpc.1304 S 1a 310S Medline 37874991 PMC 10824328 · doi ↗ · pubmed ↗
- 3Gowda SK Errichetti E Thakur V et al Trichoscopic features of scalp discoid lupus erythematosus versus lichen planopilaris: a systematic review Clin Cosmet Investig Dermatol 202417805827 doi 10.2147/CCID.S 460742 Medline 38616887 PMC 11015838 · doi ↗ · pubmed ↗
- 4Nambudiri VE Vleugels RA Laga AC Goldberg LJ Clinicopathologic lessons in distinguishing cicatricial alopecia: 7 cases of lichen planopilaris misdiagnosed as discoid lupus J Am Acad Dermatol Oct 2014714 e 1358 doi 10.1016/j.jaad.2014.04.052Medline 25219732 · doi ↗ · pubmed ↗
- 5Elmas O An effective and practical diagnostic clinical method in primary scarring alopecia: dermoscopy Turk J Dermatol 201913272 doi 10.4103/TJD.TJD_7_19 · doi ↗
- 6Starace M Pampaloni F Quadrelli F et al STRIAA (Severity Trichoscopy Index Alopecia Areata): validation of a novel trichoscopic tool for evaluation of alopecia areata Dermatol Ther (Heidelb)012025151223226 doi 10.1007/s 13555-024-01313-x Medline 39690381 PMC 11785833 · doi ↗ · pubmed ↗
- 7Rajan A Rudnicka L Szepietowski JC et al Differentiation of frontal fibrosing alopecia and Lichen planopilaris on trichoscopy: a comprehensive review J Cosmet Dermatol Jun 202221623242330 doi 10.1111/jocd.14457 Medline 34661965 · doi ↗ · pubmed ↗
- 8Gowda SK Errichetti E Behera B et al Trichoscopic features of lichen planopilaris versus frontal fibrosing alopecia: a systematic review Dermatol Pract Concept 013020251514481 doi 10.5826/dpc.1501 a 4481 Medline 40117622 PMC 11928120 · doi ↗ · pubmed ↗