Compliance and Satisfaction With a Protocol for Identifying Novel Targets to Support Postpartum Opioid Use Disorder Recovery: Prospective Cohort Study
Alicia M Allen, Linnea B Linde-Krieger, Jendar Deschenes, Stephanie Mallahan, Alexandra Harris, Mariana Felix, Arushi Chalke, Alma Anderson, Priyanka Sharma, Katherine M King, Maddy T Grant, James Baurley, Lela Rankin, Stacey Tecot

TL;DR
This study tracks individuals with opioid use disorder during pregnancy and postpartum to identify new ways to prevent relapse, and finds that participants were generally satisfied with the study despite challenges.
Contribution
The study introduces a protocol to identify novel predictors of postpartum opioid misuse through hormones and caregiving approaches.
Findings
Participants showed high completion rates for postpartum clinic visits and follow-up.
Compliance with study procedures was generally high, though lower among those with opioid use disorder.
Participants reported high satisfaction with the study procedures.
Abstract
Although treatment for opioid use disorder (OUD) often yields high adherence during pregnancy, the risk of returning to opioid misuse during postpartum is high. There are currently no relapse prevention programs tailored to this unique time period. Using a prospective cohort study, we seek to preliminarily identify hormones or infant caregiving approaches as novel predictors of postpartum opioid misuse. As a first step in dissemination of results, this report contains a detailed account of the protocol, as well as recruitment, retention, compliance, and participant satisfaction. Participants were individuals with OUD (OUD+) and those without (OUD–) who were followed from late pregnancy (≥36 gestational wk) to postpartum month 5. From childbirth to postpartum week 12, participants completed daily surveys (capturing use, craving, interactions with infant) and weekly face-to-face visits…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
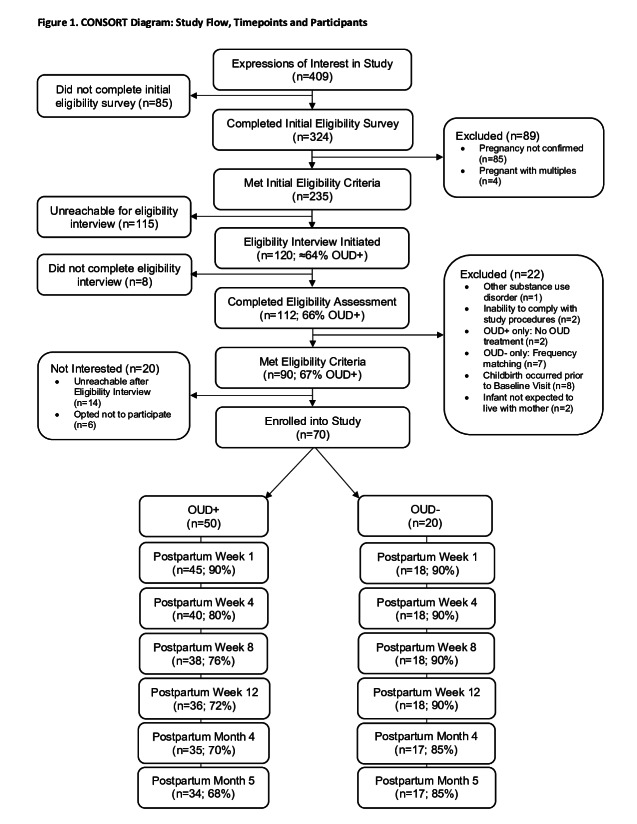 Figure 1
Figure 1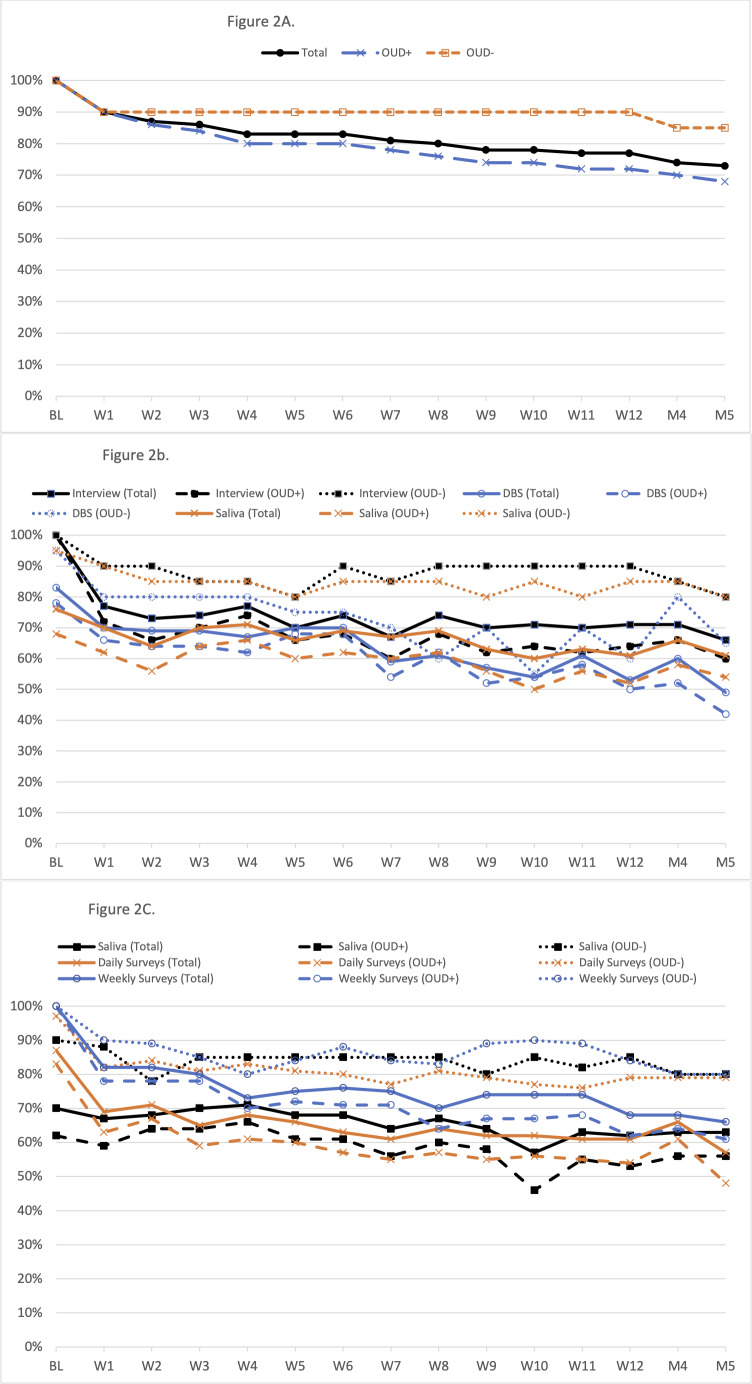 Figure 2
Figure 2| Total | OUD+ (n=50) | OUD– (n=20) | Test statistic | |
|---|---|---|---|---|
| Sociodemographic variables | ||||
| Age (y), mean (SD) | 29.3 (5.0) | 30.0 (4.9) | 27.8 (5.1) | 1.63 (.11) |
| Race and ethnicity, n (%) | 3.18 (.53) | |||
| Hispanic | 33 (47) | 21 (42) | 12 (60) | |
| NH | 28 (40) | 21 (42) | 7 (35) | |
| NH, NA/AN | 4 (6) | 3 (6) | 1 (5) | |
| NH, NH/PI | 0 (0) | 0 (0) | 0 (0) | |
| NH, Asian | 1 (1) | 1 (2) | 0 (0) | |
| NH, B/AA | 4 (6) | 4 (8) | 0 (0) | |
| Highest level of education completed, n (%) | 9.11 (0.10) | |||
| ≤8th grade | 2 (3) | 2 (4) | 0 (0) | |
| Some HS | 8 (11) | 6 (12) | 2 (10) | |
| HS or equivalent | 25 (36) | 19 (38) | 6 (30) | |
| Some college or 2-year degree | 30 (43) | 22 (44) | 8 (40) | |
| College graduate or 4-year degree | 3 (4) | 0 (0) | 3 (15) | |
| Graduate or professional degree | 2 (3) | 1 (2) | 1 (5) | |
| Insurance status, n (%) | 2.85 (.09) | |||
| Private | 6 (9) | 2 (4) | 4 (20) | |
| Public or none | 64 (91) | 48 (96) | 16 (80) | |
| Missing | 0 (0) | 0 (0) | 0 (0) | |
| Number of children living in home, mean (SD) | 1.1 (1.4) | 1.2 (1.6) | 1.0 (0.9) | 0.42 (.68) |
| Gestational week prenatal care initiated, mean (SD) | 9.1 (5.0) | 9.8 (5.2) | 7.1 (3.8) | 2.38 (.02) |
| Parity, n (%) | 0.002 (.97) | |||
| Primiparous | 19 (27) | 13 (26) | 6 (30) | |
| Multiparous | 51 (73) | 37 (74) | 14 (70) | |
| Gestational week at baseline visit, mean (SD) | 36.8 (0.8) | 36.9 (0.9) | 36.8 (0.6) | 0.32 (.75) |
| Substance use history | ||||
| Lifetime history of use of substances with abuse potential | — | |||
| Opioid-containing prescription | 58 (83) | 48 (96) | 10 (50) | |
| Heroin | 30 (43) | 30 (60) | 0 (0) | |
| Narcotics | 47 (67) | 47 (94) | 0 (0) | |
| Fentanyl | 6 (9) | 6 (12) | 0 (0) | |
| Caffeine | 68 (97) | 48 (96) | 20 (100) | |
| Alcohol | 60 (86) | 43 (86) | 17 (85) | |
| Cigarettes or nicotine | 56 (80) | 43 (86) | 13 (65) | |
| Cannabis | 56 (80) | 45 (90) | 11 (55) | |
| Cocaine | 44 (63) | 41 (82) | 3 (15) | |
| Use in 3 months prior to pregnancy of substances with abuse potential | — | |||
| Opioid-containing prescription | 18 (26) | 18 (36) | 0 (0) | |
| Heroin | 3 (4) | 3 (6) | 0 (0) | |
| Narcotics | 29 (41) | 29 (58) | 0 (0) | |
| Fentanyl | 4 (6) | 4 (8) | 0 (0) | |
| Caffeine | 66 (94) | 46 (92) | 20 (10) | |
| Alcohol | 27 (39) | 12 (24) | 15 (75) | |
| Cigarettes or nicotine | 44 (63) | 34 (68) | 10 (50) | |
| Cannabis | 38 (54) | 31 (62) | 7 (35) | |
| Cocaine | 9 (13) | 7 (14) | 2 (10) | |
| Use in last 3 months of pregnancy of substances with abuse potential | — | |||
| Opioid-containing prescription | 10 (1) | 10 (20) | 0 (0) | |
| Heroin | 0 (0) | 0 (0) | 0 (0) | |
| Narcotics | 41 (59) | 41 (82) | 0 (0) | |
| Fentanyl | 2 (3) | 2 (4) | 0 (0) | |
| Caffeine | 63 (90) | 44 (88) | 19 (95) | |
| Alcohol | 2 (3) | 2 (4) | 0 (0) | |
| Cigarettes or nicotine | 32 (46) | 28 (56) | 4 (20) | |
| Cannabis | 16 (23) | 15 (30) | 1 (5) | |
| Cocaine | 1 (1) | 1 (2) | 0 (0) | |
| Drug of choice (top 5), n (%) | — | |||
| Other opioid-containing prescription | — | 18 (36) | — | |
| Heroin | — | 11 (22) | — | |
| Fentanyl | — | 6 (12) | — | |
| Cannabis | — | 5 (10) | — | |
| Caffeine | — | 4 (8) | — | |
| Age of first opioid-containing prescription use, mean (SD) | — | 17.3 (5.7) (n=47) | — | — |
| Age of first heroin use, mean (SD) | — | 22.4 (5.7) (n=30) | — | — |
| Lifetime history treatment type, n (%) | — | |||
| Inpatient | — | 30 (60) | — | |
| Outpatient | — | 33 (66) | — | |
| Intensive outpatient | — | 27 (54) | — | |
| Current treatment type, n (%) | — | |||
| Inpatient | — | 2 (4) | — | |
| Outpatient | — | 30 (60) | — | |
| Intensive outpatient | — | 5 (10) | — | |
| Current treatment components, n (%) | — | |||
| Medications | — | 34 (68) | — | |
| Counseling/support groups | — | 24 (48) | — | |
| Other | — | 3 (6) | — | |
| Recovery length, n (%) | — | |||
| >1 year | — | 21 (42) | — | |
| Before this pregnancy but <1 year | — | 9 (18) | — | |
| First trimester of this pregnancy | — | 6 (12) | — | |
| Second trimester of this pregnancy | — | 10 (20) | — | |
| Third trimester of this pregnancy | — | 4 (8) | — | |
| Total | OUD+ | OUD– | ||
|---|---|---|---|---|
| Sample size by time point | ||||
| W1 | 20 | 17 | 3 | — |
| W12 | 31 | 25 | 6 | — |
| M5 | 45 | 32 | 13 | — |
| Based on your experience, how willing would you be to participate in a study like this again? Mean (SD) | ||||
| W1 | 2.6 (0.8) | 2.6 (0.9) | 2.7 (0.6) | .60 |
| W12 | 2.9 (0.4) | 2.8 (0.5) | 3.0 (0.0) | >.99 |
| M5 | 2.7 (0.8) | 2.7 (0.8) | 2.7 (0.6) | .56 |
| Overall, how much of a burden has it been to participate in this study? Mean (SD) | ||||
| W1 | 0.6 (0.8) | 0.6 (0.9) | 0.3 (0.6) | >.99 |
| W12 | 0.5 (0.8) | 0.6 (0.9) | 0.3 (0.5) | >.99 |
| M5 | 0.4 (0.7) | 0.4 (0.8) | 0.4 (0.6) | >.99 |
| How much of a burden was it to participate in this study before your baby was born? Mean (SD) | ||||
| W12 | 0.2 (0.6) | 0.2 (0.6) | 0.0 (0.0) | >.99 |
| How much of a burden was it to participate in this study after your baby was born? Mean (SD) | ||||
| W12 | 0.6 (0.8) | 0.6 (0.9) | 0.5 (0.5) | .51 |
| Overall, how much has participating in this study interfered with your usual activities? Mean (SD) | ||||
| W1 | 0.7 (0.8) | 0.7 (0.8) | 0.3 (0.6) | >.99 |
| W12 | 0.6 (0.8) | 0.5 (0.8) | 1.0 (1.1) | .38 |
| How much did participating before your baby was born interfere with your usual activities? Mean (SD) | ||||
| W12 | 0.2 (0.6) | 0.3 (0.7) | 0.2 (0.4) | >.99 |
| How much did participating after your baby was born interfere with your usual activities? Mean (SD) | ||||
| W12 | 0.7 (0.8 | 0.7 (0.9 | 0.7 (0.5) | .53 |
| How much difficulty did you have completing the study questionnaires? Mean (SD) | ||||
| W1 | 0.3 (0.7) | 0.4 (0.8) | 0.0 (0.0) | >.99 |
| How much difficulty did you have using a cell phone to complete the study questionnaires? Mean (SD) | ||||
| W12 | 0.1 (0.4) | 0.1 (0.4) | 0.0 (0.0) | >.99 |
| How much have you been annoyed with the number of alerts you have received in this study before your baby was born? Mean (SD) | ||||
| W12 | 0.2 (0.5 | 0.3 (0.5) | 0.0 (0.0 | .63 |
| How much have you been annoyed with the number of alerts you have received in this study after your baby was born? Mean (SD) | ||||
| W12 | 0.3 (0.7) | 0.4 (0.8) | 0.2 (0.4) | >.99 |
| How difficult was it to notify the study staff of your child’s birth? Mean (SD) | ||||
| W1 | 0.1 (0.7) | 0.2 (0.7) | 0.0 (0.0) | >.99 |
| Have you had any difficulties working with study staff? Mean (SD) | ||||
| W1 | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | — |
| W12 | 0.0 (0.0) | 0.0 (0.0) | 0.0 (0.0) | — |
| M5 | 0.0 (0.2) | 0.1 (0.2) | 0.0 (0.0) | >.99 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrenatal Substance Exposure Effects · Opioid Use Disorder Treatment · Maternal Mental Health During Pregnancy and Postpartum
Introduction
Perinatal opioid use disorder (OUD) is increasingly common with most recent estimates indicating that up to 324 per 10,000 births are impacted [1-3]. Medication for OUD (MOUD) is the gold standard treatment, improving both maternal and infant outcomes [4-6]. However, the risk for return to opioid misuse and overdose increases during postpartum [78]. In fact, opioid overdose is now a leading cause of maternal mortality [9], with additional significant adverse impacts on the birthing person, infant, family, and beyond [31011]. To address this period of high risk, the American College of Obstetricians and Gynecologists and the American Society of Addiction Medicine recommends that “Access to…relapse prevention programs should be made available” [6]. However, there are currently no evidence-based relapse prevention programs tailored to the unique postpartum circumstances [12]. Additionally, factors that contribute to the increased risk of return to use during postpartum are not well understood [9]. Ultimately, developing effective relapse prevention programs that can work adjunctive to MOUD and are tailored to postpartum-specific needs will allow parents, infants, and families enhanced opportunities to achieve positive long-term outcomes.
Ovarian hormones have been implicated as important factors for clinical treatment of substance use disorders [13-15]. For instance, in ovariectomized female rats offered intermittent access to fentanyl, those who received exogenous estradiol treatment exhibited increases in self-administration, enhanced sensitivity, and increased motivation versus placebo treatment [16]. Exogenous progesterone treatment is associated with reductions in combustible cigarette smoking during the postpartum period, as well as in nonpregnant females [17-19]. Hormonal influences on substance misuse behaviors may be amplified during the perinatal period, as hormones change by up to 300-fold during pregnancy, followed by a dramatic decline in the early postpartum and additional variation with lactation [20]. Interestingly, some of the natural hormonal patterns that occur during the perinatal period directly mirror the risk of substance misuse. For instance, both estrogen (which facilitates drug-taking behaviors) and risk of substance misuse are low during lactation, whereas without lactation, both estrogen and risk of substance misuse increase [2021]. Further, specific infant caregiving activities can have substantial effects on hormones (eg, oxytocin increases during skin-to-skin contact), which may directly or indirectly impact postpartum substance relapse risk [22-25]. Despite the observed links between ovarian hormones and substance misuse as well as infant caregiving approaches and ovarian hormones, paired with the dramatic perinatal hormonal variations, the specific examination of postpartum hormonal patterns with OUD recovery-related outcomes has yet to be explored.
We conducted a prospective cohort study with those who did and did not have perinatal OUD to examine hormones or infant caregiving activities as modifiable risk factors that future interventions may target to enhance protection against return to opioid misuse. In order to specifically study postpartum relapse risk, we recruited participants with OUD who were stable in recovery during pregnancy, as well as comparable control group participants without OUD, and followed them across the high-risk postpartum period. As a first step in dissemination, this paper aims to (1) detail our protocols and methodologies and (2) report on recruitment, retention, compliance, and participant satisfaction. Ultimately, the goal of this paper is to enhance the understanding of perinatal OUD experience and inform the development of novel interventions and treatment options to support postpartum recovery and well-being.
Methods
Ethical Considerations
This study was approved by the University of Arizona’s Institutional Review Board (2009060851R001). Study staff met with all participants to obtain informed consent prior to their participation in the study. To maintain privacy and confidentiality, all data were stored with an alphanumeric identifier on secured platforms, only accessible by study staff. Participants were compensated up to US $725.
Recruitment
In this prospective cohort study, we sought to enroll 50 pregnant people with OUD (OUD+) and 25 pregnant people without OUD (OUD–). We opted for a prospective cohort study design with frequent measurements to allow for the assessment of numerous modifiable risk factors (eg, estradiol, skin-to-skin contact). Specifically, with a primary sample of 75 independent participants who completed daily measurements across the first 12 weeks postpartum, this longitudinal study was designed to yield approximately 70,000 data points, providing adequate statistical power for within-person analyses and robust estimation of individual trajectories. It is noted that this sample size has limited power for between-group comparisons. However, the inclusion of OUD– will allow us to explore hormonal or infant caregiving approaches that are unique to OUD+. Overall, this approach will achieve the primary goal of preliminarily identifying meaningful relationships between hormones or infant caregiving with return to opioid misuse that can be further explored in future fully powered randomized control trials.
Participants met the following inclusion criteria: (1) 18‐40 years old, (2) uncomplicated single-gestation pregnancy at gestational week 30 or beyond, (3) a self-reported expectation of residing with the infant after birth, (4) English fluency, and (5) willing and able to comply with procedures. Additionally, OUD+ had to (6) report use of opioids during pregnancy, (7) report current OUD treatment with plans to continue treatment after childbirth, and (8) allow us access to their OUD treatment records. All participants were excluded for preterm birth (<36 gestational wk), planned long-distance moves, or extended travel through 6 months postpartum. Additional OUD– exclusion criteria included the use of opioids during pregnancy or a history of opioid use disorder. Finally, upon enrollment, we utilized frequency matching at the group level with a goal of ensuring the groups were comparable on proportion with no health insurance or public insurance versus private insurance, as well as on average age (ie,±5 y).
We recruited participants in the metro areas of Tucson and Phoenix, Arizona, from August 2021 to March 2024 via flyers or tabling at local health care provider clinics, community resources, community events, and social media. Individuals expressed their interest via a survey on REDCap [26], and this was followed by a telephone-based eligibility interview with staff. If eligibility criteria were met, potential participants were invited to a face-to-face baseline visit to commence participation.
Data Collection Procedures
We implemented a data collection protocol similar to one we previously used with success in a pilot study focused on postpartum cigarette smoking relapse prevention [17]. Participants completed 15 visits either in-person (at our clinic or the participant’s home) or remotely via Health Insurance Portability and Accountability Act–compliant Zoom for Health, with all data entered on REDCap [26]. Visits were scheduled to begin between 7 AM and 11 AM given the known diurnal patterns in hormones and other variables of interest [2728]. For those who attended remotely, study supplies were mailed in advance. All visits included the collection of biological samples, with all participants provided 1.8 mL of saliva via passive drool. Remote participants self-collected 12 drops of blood for dried blood spots using our previously developed protocol [29]. In-person participants provided 8 mL of venous blood, which was then processed to yield 12 drops of dried blood spots plus plasma samples. For remote participants, dried blood spots were mailed to staff weekly, and frozen saliva samples were picked up in batches by staff. All samples were subsequently stored at ≤−20 °C.
Baseline
At gestational week 36 or beyond, participants completed a baseline visit. After providing informed consent, participants completed an interview with staff to obtain their medical history, followed by completion of surveys and biological sample collection. Next, participants completed a semistructured audio-recorded interview with staff on lifetime trauma and resilience (Multimedia Appendix 1). At the end of the visit, participants were trained on how to complete daily surveys and at-home saliva samples, followed by receipt of compensation.
Daily Surveys
Beginning the day after baseline through postpartum week 12, participants completed daily surveys on their own or study-supplied smartphones. This was replicated the week preceding follow-up visits. Participants received a daily text message or email at 8 PM containing a link to surveys. Surveys remained open until 11:59 PM, with reminders every 30 minutes until completed. Surveys took approximately 10‐15 minutes to complete and documented use of and craving for substances, interactions, and connectedness with the infant and others, and other validated measures to capture return to use risk factors.
Fourth Trimester (Postpartum Weeks 1‐12)
Participants notified staff of childbirth via the daily surveys, then commenced weekly visits. At each visit, participants completed surveys and provided in-visit biological samples. Additionally, at-home saliva samples were collected at 8 PM the day before and 30 minutes after waking on the day of the visit. Participants were also interviewed to capture substance use, changes in health or medication, and time spent with the infant. At postpartum week 1, participants completed a semistructured audio-recorded interview with staff to capture birth and initial breastfeeding experiences (Multimedia Appendix 2). Approximately 1 year into study recruitment, we added a study satisfaction survey to postpartum weeks 1 and 12. Upon completion of each visit, the next visit was confirmed, and participants were compensated.
Follow-Up Visits (Postpartum Months 4 and 5)
Procedures were identical to the fourth trimester data collection. In addition, at postpartum month 5, participants completed a semistructured audio-recorded interview with staff to capture their breastfeeding experiences and a final satisfaction survey.
Study Measures
Overall, participants completed a series of instruments on a daily, weekly, and monthly basis, as well as at follow-up (MultimediaAppendices 34).
Background Variables
During the enrollment interview and at the baseline visit, standardized questionnaires and interviews were used to capture sociodemographics (eg, age, race, ethnicity), medical history (eg, parity, diagnosis of hormone-influencing conditions), and history of substance use (eg, lifetime use of 16 different substances, drug of choice, OUD treatment experiences). The baseline interview incorporated Stressful Life Events [30], Adverse Childhood Experiences [31], Early Trauma Inventory [3233], and Resilience Scale [34].
Maternal Factors
These variables included (1) known or suspected risk factors for postpartum substance misuse, (2) known or suspected association with hormones of interest, and (3) infant caregiving and parental experiences [35-51]. In brief, participants reported on lactation and breastfeeding (daily first 4 weeks, weekly thereafter), pain (daily first 4 weeks), and vaginal bleeding (daily after postpartum week 4), with additional assessments on a weekly or monthly basis.
Caregiving Factors
Variables included those that may contribute to risk of postpartum return to misuse or influence hormone levels. Daily, participants reported on their perceptions of parenting challenge, parenting reward, and connections with infant and with others using a 100-point visual analog scale ranging from “not at all” to “extremely.” Relative time spent with infant each day was reported using an investigator-created instrument with 100-point visual analog scale ranging from “a lot less than usual” to “a lot more than usual” to report on the amount of time spent: (1) in skin-to-skin contact with infant, (2) in other physical contact with infant, (3) caring for infant but not in physical contact, (4) with someone else while they cared for infant, and (5) time away from infant. Weekly staff interviewed participants to capture the average absolute time spent on each of these activities during the preceding week, ensuring that total time reported equated to 24 hours per day. Additional validated items were completed regularly throughout follow-up.
Hormones
We measured a total of 19 hormones at each time point. Cortisol and oxytocin assays were completed by the Laboratory for the Evolutionary Endocrinology of Primates at the University of Arizona. Saliva samples were stored at −80 °C, thawed to room temperature before analysis, and cleaned by centrifuging for 30 minutes at 3000 rpm with the supernatant retained. Saliva was aliquoted into microcentrifuge tubes at volumes of 500 µL for oxytocin and 150 µL for cortisol, then frozen at −80 °C until lyophilization. Samples were lyophilized at −80 °C and 0.3 mbar until completely dry, then resuspended in 250 µL and 150 µL of assay buffer (Arbor Assays, Ann Arbor, MI, USA), respectively. This resulted in 2x concentration for oxytocin and 1x concentration for cortisol. Samples were assayed according to protocols included with DetectX ELISA oxytocin (K048-H5; cross-reactivity with isotocin 94.3%, mesotocin 88.4%, other analytes <0.15%; sensitivity 17.0 pg/mL; limit of detection 22.9 pg/mL) and DetectX ELISA cortisol kits (K003-H5; cross-reactivity with dexamethasone 18.8%, prednisolone [1-dehydrocortisol] 7.8%, corticosterone and cortisone 1.2%, other analytes <0.1%; sensitivity 27.6 pg/mL; limit of detection 45.4 pg/mL). Plates were read at 450 nm on a BioTek Multi-Mode plate reader. The Laboratory for the Evolutionary Endocrinology of Primates conducted analytical validations of methods for adult female human saliva using tests of parallelism and accuracy for each analyte. Parallelism was done by serially diluting a sample pool, correcting the resulting concentrations at each dilution, and calculating the coefficient of variation [52]. The coefficient of variation of corrected concentrations from serially diluted saliva was 11.65% for oxytocin (n=5 dilutions) and 8.34% for cortisol (n=10 dilutions). For accuracy, sample pools were spiked with 10% synthetic oxytocin or cortisol in assay buffer, at different concentrations along the standard curve. Recovery for salivary oxytocin was 119.99%±0.05, and recovery for salivary cortisol was 102.18%±2.31. All samples were assayed in duplicate, and all plates included high and low pool controls to assess inter- and intra-assay variation. Any samples with concentrations that were outside of the standard curve range were diluted or concentrated and reassayed. Data were processed using the BioTek Gen5 software (version 3.08; Aligent Technologies) to calculate analyte concentrations.
Using dried blood spots, ZRT Laboratory (Beaverton, OR) measured cortisol, estrone, estradiol, estriol, testosterone, progesterone, DHEAS, cortisone, estrone-1-sulfate, pregnenolone sulfate, 17-hydroxyprogesterone, androstenedione, 7-keto DHEA, corticosterone, 11-deoxycortisol, ethinyl estradiol, anastrozole, and letrozole as previously described with some modifications [53]. Three 6-mm diameter punches were taken from each dried blood spot specimen and rehydrated. Steroids were extracted with organic solvent in the presence of internal standard, purified by solid-phase extraction, derivatized (estrogens only), and then analyzed by liquid chromatography-mass spectrometry. Liquid chromatography-mass spectrometry analysis was performed using ultra-fast liquid chromatography system (Shimadzu Nexera XR) coupled to a triple quadrupole mass spectrometer (AB Sciez 5500) equipped with an electrospray ionization source. Separations were conducted by reversed-phase chromatography, and the mass spectrometer was operated in multiple reaction monitoring mode. Data were processed using the Sciex OS software (version 1.7.2; AB Scienx) to determine analyte concentrations. All samples were run with dried blood spot controls, generated in-house by spiking stripped serum with various analyte concentrations, mixing washed red blood cells, and then spotting onto filter paper.
Factors Related to Substance Use
To assess postpartum risk for opioid misuse, we included 3 outcomes. First, daily self-reports of opioid cravings (separately for opioid-containing prescription medications, heroin, and MOUD medications) and coping with cravings. Both cravings and coping with craving were reported with a 100-point visual analog scale ranging from “not at all” to “severe” or “very well,” respectively. Second, daily self-reports of opioid use were captured via daily surveys and staff-administered TimeLine FollowBack [54] interviews at each visit. These approaches were also used to capture craving and use of 15 other substances. Finally, we reviewed toxicology results and treatment adherence via treatment program medical records.
Statistical Analyses
Study sample descriptors (eg, sociodemographics, substance use) and outcomes were summarized with descriptive statistics. Group differences (ie, OUD+ vs OUD–) were compared using Welch t tests, χ^2^ tests, and Fisher exact tests. For the latter, although some cells contained relatively large counts (up to 45), exact P values were computed without the need for permutations. Group differences in compliance over time were also examined with binomial logistic regression models. All analyses were completed using open-source Python (3.10.11) libraries, Pandas 2.0.1 (NumFOCUS, Inc.), SciPy 1.13.0, and R Studio (2024.09.1, Build 394).
Results
Study Sample
A total of 70 participants enrolled in the study and completed the baseline assessment to form the final sample (Figure 1; note that these numbers exclude 1 participant who enrolled into the OUD– and later requested her data be removed). The final enrolled sample included 50 (71%) OUD+ and 20 (29%) OUD– (Table 1). Study groups were exchangeable on all sociodemographic variables except for gestational week prenatal care was initiated (OUD+: 9.8 [SD 5.2] vs OUD–: 7.1 [SD 3.8]; P value=.02). There was little evidence of selection bias from phone screening or enrollment to the postpartum data collection period (MultimediaAppendices 56). For example, the average age at enrollment was 28.6 (SD 5.2; n=112) compared to 29.4 (SD 5.1) among those who completed at least 1 postpartum visit (n=61). Additionally, 52% (n=58) of participants who completed the phone screening identified as Hispanic and 37% (n=41) reported education of some college compared to 51% (n=31) and 41% (n=25), respectively, at postpartum data collection. Among OUD+, at enrollment, 58% (n=50) reported being in recovery for less than a year compared to 56% (n=43) at postpartum data collection, with an age of first use of heroin reported as 17.3 (SD 5.7) years old (n=47) versus 17.5 (SD 5.9) years old (n=41), respectively.
Consolidated Standards of Reporting Trials (CONSORT) diagram: study flow, time points, and participants. OUD: opioid use disorder.
Table 1.: Description of final study sample (n=70).
<table><thead><tr><th rowspan="1" colspan="1"/><th rowspan="1" colspan="1">Total<break/>(n=70)</th><th rowspan="1" colspan="1">OUD+ (n=50)</th><th rowspan="1" colspan="1">OUD– (n=20)</th><th rowspan="1" colspan="1">Test statistic<xref><sup>a</sup></xref> (<italic>P</italic> value)</th></tr></thead><tbody><tr><td rowspan="1" colspan="1">Sociodemographic variables</td></tr><tr><td rowspan="1" colspan="1"> Age (y), mean (SD)</td><td align="left" rowspan="1" colspan="1">29.3 (5.0)</td><td align="left" rowspan="1" colspan="1">30.0 (4.9)</td><td align="left" rowspan="1" colspan="1">27.8 (5.1)</td><td align="left" rowspan="1" colspan="1">1.63 (.11)</td></tr><tr><td rowspan="1" colspan="1">Race and ethnicity, n (%)</td><td rowspan="1" colspan="1">3.18 (.53)</td></tr><tr><td rowspan="1" colspan="1"> Hispanic</td><td rowspan="1" colspan="1">33 (47)</td><td rowspan="1" colspan="1">21 (42)</td><td rowspan="1" colspan="1">12 (60)</td></tr><tr><td rowspan="1" colspan="1"> NH<xref><sup>b</sup></xref>, White</td><td rowspan="1" colspan="1">28 (40)</td><td rowspan="1" colspan="1">21 (42)</td><td rowspan="1" colspan="1">7 (35)</td></tr><tr><td rowspan="1" colspan="1"> NH, NA/AN<xref><sup>c</sup></xref></td><td rowspan="1" colspan="1">4 (6)</td><td rowspan="1" colspan="1">3 (6)</td><td rowspan="1" colspan="1">1 (5)</td></tr><tr><td rowspan="1" colspan="1"> NH, NH/PI<xref><sup>d</sup></xref></td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> NH, Asian</td><td rowspan="1" colspan="1">1 (1)</td><td rowspan="1" colspan="1">1 (2)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> NH, B/AA<xref><sup>e</sup></xref></td><td rowspan="1" colspan="1">4 (6)</td><td rowspan="1" colspan="1">4 (8)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td colspan="4" rowspan="1">Highest level of education completed, n (%)<break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">9.11 (0.10)</td></tr><tr><td rowspan="1" colspan="1"> ≤8th grade</td><td rowspan="1" colspan="1">2 (3)</td><td rowspan="1" colspan="1">2 (4)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Some HS<xref><sup>f</sup></xref></td><td rowspan="1" colspan="1">8 (11)</td><td rowspan="1" colspan="1">6 (12)</td><td rowspan="1" colspan="1">2 (10)</td></tr><tr><td rowspan="1" colspan="1"> HS or equivalent</td><td rowspan="1" colspan="1">25 (36)</td><td rowspan="1" colspan="1">19 (38)</td><td rowspan="1" colspan="1">6 (30)</td></tr><tr><td rowspan="1" colspan="1"> Some college or 2-year degree</td><td rowspan="1" colspan="1">30 (43)</td><td rowspan="1" colspan="1">22 (44)</td><td rowspan="1" colspan="1">8 (40)</td></tr><tr><td rowspan="1" colspan="1"> College graduate or 4-year degree</td><td rowspan="1" colspan="1">3 (4)</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">3 (15)</td></tr><tr><td rowspan="1" colspan="1"> Graduate or professional degree</td><td rowspan="1" colspan="1">2 (3)</td><td rowspan="1" colspan="1">1 (2)</td><td rowspan="1" colspan="1">1 (5)</td></tr><tr><td rowspan="1" colspan="1">Insurance status, n (%)<break/><break/><break/><break/><break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">2.85 (.09)</td></tr><tr><td rowspan="1" colspan="1"> Private</td><td rowspan="1" colspan="1">6 (9)</td><td rowspan="1" colspan="1">2 (4)</td><td rowspan="1" colspan="1">4 (20)</td></tr><tr><td rowspan="1" colspan="1"> Public or none</td><td rowspan="1" colspan="1">64 (91)</td><td rowspan="1" colspan="1">48 (96)</td><td rowspan="1" colspan="1">16 (80)</td></tr><tr><td rowspan="1" colspan="1"> Missing</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1">Number of children living in home, mean (SD)</td><td align="left" rowspan="1" colspan="1">1.1 (1.4)</td><td align="left" rowspan="1" colspan="1">1.2 (1.6)</td><td align="left" rowspan="1" colspan="1">1.0 (0.9)</td><td align="left" rowspan="1" colspan="1">0.42 (.68)</td></tr><tr><td rowspan="1" colspan="1">Gestational week prenatal care initiated, mean (SD)</td><td align="left" rowspan="1" colspan="1">9.1 (5.0)</td><td align="left" rowspan="1" colspan="1">9.8 (5.2)</td><td align="left" rowspan="1" colspan="1">7.1 (3.8)</td><td align="left" rowspan="1" colspan="1">2.38 (.02)</td></tr><tr><td rowspan="1" colspan="1">Parity, n (%)<break/><break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">0.002 (.97)</td></tr><tr><td rowspan="1" colspan="1"> Primiparous</td><td rowspan="1" colspan="1">19 (27)</td><td rowspan="1" colspan="1">13 (26)</td><td rowspan="1" colspan="1">6 (30)</td></tr><tr><td rowspan="1" colspan="1"> Multiparous</td><td rowspan="1" colspan="1">51 (73)</td><td rowspan="1" colspan="1">37 (74)</td><td rowspan="1" colspan="1">14 (70)</td></tr><tr><td rowspan="1" colspan="1">Gestational week at baseline visit, mean (SD)</td><td align="left" rowspan="1" colspan="1">36.8 (0.8)</td><td align="left" rowspan="1" colspan="1">36.9 (0.9)</td><td align="left" rowspan="1" colspan="1">36.8 (0.6)</td><td align="left" rowspan="1" colspan="1">0.32 (.75)</td></tr><tr><td rowspan="1" colspan="1">Substance use history</td></tr><tr><td rowspan="1" colspan="1"> Lifetime history of use of substances with abuse potential<xref><sup>g</sup></xref>, n (%)<break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—<xref><sup>h</sup></xref></td></tr><tr><td rowspan="1" colspan="1"> Opioid-containing prescription</td><td rowspan="1" colspan="1">58 (83)</td><td rowspan="1" colspan="1">48 (96)</td><td rowspan="1" colspan="1">10 (50)</td></tr><tr><td rowspan="1" colspan="1"> Heroin</td><td rowspan="1" colspan="1">30 (43)</td><td rowspan="1" colspan="1">30 (60)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Narcotics</td><td rowspan="1" colspan="1">47 (67)</td><td rowspan="1" colspan="1">47 (94)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Fentanyl</td><td rowspan="1" colspan="1">6 (9)</td><td rowspan="1" colspan="1">6 (12)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Caffeine</td><td rowspan="1" colspan="1">68 (97)</td><td rowspan="1" colspan="1">48 (96)</td><td rowspan="1" colspan="1">20 (100)</td></tr><tr><td rowspan="1" colspan="1"> Alcohol</td><td rowspan="1" colspan="1">60 (86)</td><td rowspan="1" colspan="1">43 (86)</td><td rowspan="1" colspan="1">17 (85)</td></tr><tr><td rowspan="1" colspan="1"> Cigarettes or nicotine</td><td rowspan="1" colspan="1">56 (80)</td><td rowspan="1" colspan="1">43 (86)</td><td rowspan="1" colspan="1">13 (65)</td></tr><tr><td rowspan="1" colspan="1"> Cannabis</td><td rowspan="1" colspan="1">56 (80)</td><td rowspan="1" colspan="1">45 (90)</td><td rowspan="1" colspan="1">11 (55)</td></tr><tr><td rowspan="1" colspan="1"> Cocaine</td><td rowspan="1" colspan="1">44 (63)</td><td rowspan="1" colspan="1">41 (82)</td><td rowspan="1" colspan="1">3 (15)</td></tr><tr><td rowspan="1" colspan="1">Use in 3 months prior to pregnancy of substances with abuse potential<xref><sup>g</sup></xref>, n (%)<break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Opioid-containing prescription</td><td rowspan="1" colspan="1">18 (26)</td><td rowspan="1" colspan="1">18 (36)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Heroin</td><td rowspan="1" colspan="1">3 (4)</td><td rowspan="1" colspan="1">3 (6)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Narcotics</td><td rowspan="1" colspan="1">29 (41)</td><td rowspan="1" colspan="1">29 (58)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Fentanyl</td><td rowspan="1" colspan="1">4 (6)</td><td rowspan="1" colspan="1">4 (8)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Caffeine</td><td rowspan="1" colspan="1">66 (94)</td><td rowspan="1" colspan="1">46 (92)</td><td rowspan="1" colspan="1">20 (10)</td></tr><tr><td rowspan="1" colspan="1"> Alcohol</td><td rowspan="1" colspan="1">27 (39)</td><td rowspan="1" colspan="1">12 (24)</td><td rowspan="1" colspan="1">15 (75)</td></tr><tr><td rowspan="1" colspan="1"> Cigarettes or nicotine</td><td rowspan="1" colspan="1">44 (63)</td><td rowspan="1" colspan="1">34 (68)</td><td rowspan="1" colspan="1">10 (50)</td></tr><tr><td rowspan="1" colspan="1"> Cannabis</td><td rowspan="1" colspan="1">38 (54)</td><td rowspan="1" colspan="1">31 (62)</td><td rowspan="1" colspan="1">7 (35)</td></tr><tr><td rowspan="1" colspan="1"> Cocaine</td><td rowspan="1" colspan="1">9 (13)</td><td rowspan="1" colspan="1">7 (14)</td><td rowspan="1" colspan="1">2 (10)</td></tr><tr><td rowspan="1" colspan="1">Use in last 3 months of pregnancy of substances with abuse potential<xref><sup>g</sup></xref>, n (%)<break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Opioid-containing prescription</td><td rowspan="1" colspan="1">10 (1)</td><td rowspan="1" colspan="1">10 (20)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Heroin</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Narcotics</td><td rowspan="1" colspan="1">41 (59)</td><td rowspan="1" colspan="1">41 (82)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Fentanyl</td><td rowspan="1" colspan="1">2 (3)</td><td rowspan="1" colspan="1">2 (4)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Caffeine</td><td rowspan="1" colspan="1">63 (90)</td><td rowspan="1" colspan="1">44 (88)</td><td rowspan="1" colspan="1">19 (95)</td></tr><tr><td rowspan="1" colspan="1"> Alcohol</td><td rowspan="1" colspan="1">2 (3)</td><td rowspan="1" colspan="1">2 (4)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1"> Cigarettes or nicotine</td><td rowspan="1" colspan="1">32 (46)</td><td rowspan="1" colspan="1">28 (56)</td><td rowspan="1" colspan="1">4 (20)</td></tr><tr><td rowspan="1" colspan="1"> Cannabis</td><td rowspan="1" colspan="1">16 (23)</td><td rowspan="1" colspan="1">15 (30)</td><td rowspan="1" colspan="1">1 (5)</td></tr><tr><td rowspan="1" colspan="1"> Cocaine</td><td rowspan="1" colspan="1">1 (1)</td><td rowspan="1" colspan="1">1 (2)</td><td rowspan="1" colspan="1">0 (0)</td></tr><tr><td rowspan="1" colspan="1">Drug of choice (top 5), n (%)<break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Other opioid-containing prescription</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">18 (36)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Heroin</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">11 (22)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Fentanyl</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">6 (12)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Cannabis</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">5 (10)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Caffeine</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">4 (8)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Age of first opioid-containing prescription use, mean (SD)</td><td align="left" rowspan="1" colspan="1">—</td><td align="left" rowspan="1" colspan="1">17.3 (5.7) (n=47)</td><td align="left" rowspan="1" colspan="1">—</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Age of first heroin use, mean (SD)</td><td align="left" rowspan="1" colspan="1">—</td><td align="left" rowspan="1" colspan="1">22.4 (5.7) (n=30)</td><td align="left" rowspan="1" colspan="1">—</td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Lifetime history treatment type, n (%)<break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Inpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">30 (60)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Outpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">33 (66)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Intensive outpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">27 (54)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Current treatment type, n (%)<break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Inpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">2 (4)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Outpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">30 (60)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Intensive outpatient</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">5 (10)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Current treatment components, n (%)<break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Medications</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">34 (68)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Counseling/support groups</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">24 (48)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Other</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">3 (6)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1">Recovery length, n (%)<break/><break/><break/><break/></td><td align="left" rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> >1 year</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">21 (42)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Before this pregnancy but <1 year</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">9 (18)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> First trimester of this pregnancy</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">6 (12)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Second trimester of this pregnancy</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">10 (20)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> Third trimester of this pregnancy</td><td rowspan="1" colspan="1">—</td><td rowspan="1" colspan="1">4 (8)</td><td rowspan="1" colspan="1">—</td></tr></tbody></table>Protocol Compliance
Nearly all participants (n=65, 93%) reported childbirth to staff (OUD+: 92%, OUD–: 95%), and 62 (87%) completed at least 1 study visit post-childbirth (OUD+: 86%, OUD–: 90%). Visit completion rates post-baseline ranged from 90% at postpartum week 1% to 73% at postpartum month 5 (Figure 2; Multimedia Appendix 7), with lower rates in the OUD+ group and at later time points. Compliance with procedures followed similar patterns (lower in OUD+ and at later time points), with the highest overall compliance, on average, with the weekly surveys (81%), followed by interviews (74%), saliva samples (66%), daily surveys (66%), and dried blood spots (63%). While there were no differences in the decline in compliance over time by group by procedure (interviews [β=.04, P=.40], dried blood spots [β=.04, P=.22], saliva samples [in visit: β=.01, P=.89; outside of visit: β=−.01, P=.82], nor surveys [daily: β=−.01, P=.80; weekly: β=−.04, P=.10]), OUD+ visit attendance declined more rapidly over time compared to OUD– (β=−.06, P=.03).
Completion rates by study group, time point, and procedure: (a) visit completion by study group, (b) compliance with in-visit procedure over time by modality and group, and (c) compliance with out-of-visit procedure over time by modality and group. OUD: opioid use disorder.
Study Satisfaction
Among the subgroup of participants who completed the study satisfaction surveys, results indicate that the study was well tolerated over time with no significant differences by study groups (Table 2).
Table 2.: Study satisfaction by study group and time pointa.
<table><thead><tr><th rowspan="1" colspan="1"/><th rowspan="1" colspan="1">Total</th><th rowspan="1" colspan="1">OUD+<break/><break/></th><th rowspan="1" colspan="1">OUD–<break/><break/></th><th rowspan="1" colspan="1"><italic>P</italic> value<xref><sup>b</sup></xref></th></tr></thead><tbody><tr><td colspan="5" rowspan="1">Sample size by time point<xref><sup>c</sup></xref><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1<xref><sup>d</sup></xref></td><td rowspan="1" colspan="1">20</td><td rowspan="1" colspan="1">17</td><td rowspan="1" colspan="1">3</td><td rowspan="1" colspan="1">—<xref><sup>e</sup></xref></td></tr><tr><td rowspan="1" colspan="1"> W12<xref><sup>f</sup></xref></td><td rowspan="1" colspan="1">31</td><td rowspan="1" colspan="1">25</td><td rowspan="1" colspan="1">6</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> M5<xref><sup>g</sup></xref></td><td rowspan="1" colspan="1">45</td><td rowspan="1" colspan="1">32</td><td rowspan="1" colspan="1">13</td><td rowspan="1" colspan="1">—</td></tr><tr><td colspan="5" rowspan="1">Based on your experience, how willing would you be to participate in a study like this again? Mean (SD)<break/><break/><break/><break/><break/><break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">2.6 (0.8)</td><td rowspan="1" colspan="1">2.6 (0.9)</td><td rowspan="1" colspan="1">2.7 (0.6)</td><td rowspan="1" colspan="1">.60</td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">2.9 (0.4)</td><td rowspan="1" colspan="1">2.8 (0.5)</td><td rowspan="1" colspan="1">3.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td rowspan="1" colspan="1"> M5</td><td rowspan="1" colspan="1">2.7 (0.8)</td><td rowspan="1" colspan="1">2.7 (0.8)</td><td rowspan="1" colspan="1">2.7 (0.6)</td><td rowspan="1" colspan="1">.56</td></tr><tr><td colspan="5" rowspan="1">Overall, how much of a burden has it been to participate in this study? Mean (SD)<break/><break/><break/><break/><break/><break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">0.6 (0.8)</td><td rowspan="1" colspan="1">0.6 (0.9)</td><td rowspan="1" colspan="1">0.3 (0.6)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.5 (0.8)</td><td rowspan="1" colspan="1">0.6 (0.9)</td><td rowspan="1" colspan="1">0.3 (0.5)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td rowspan="1" colspan="1"> M5</td><td rowspan="1" colspan="1">0.4 (0.7)</td><td rowspan="1" colspan="1">0.4 (0.8)</td><td rowspan="1" colspan="1">0.4 (0.6)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How much of a burden was it to participate in this study before your baby was born? Mean (SD)<break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.2 (0.6)</td><td rowspan="1" colspan="1">0.2 (0.6)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How much of a burden was it to participate in this study after your baby was born? Mean (SD)<break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.6 (0.8)</td><td rowspan="1" colspan="1">0.6 (0.9)</td><td rowspan="1" colspan="1">0.5 (0.5)</td><td rowspan="1" colspan="1">.51</td></tr><tr><td colspan="5" rowspan="1">Overall, how much has participating in this study interfered with your usual activities? Mean (SD)<break/><break/><break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">0.7 (0.8)</td><td rowspan="1" colspan="1">0.7 (0.8)</td><td rowspan="1" colspan="1">0.3 (0.6)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.6 (0.8)</td><td rowspan="1" colspan="1">0.5 (0.8)</td><td rowspan="1" colspan="1">1.0 (1.1)</td><td rowspan="1" colspan="1">.38</td></tr><tr><td colspan="5" rowspan="1">How much did participating before your baby was born interfere with your usual activities? Mean (SD)<break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.2 (0.6)</td><td rowspan="1" colspan="1">0.3 (0.7)</td><td rowspan="1" colspan="1">0.2 (0.4)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How much did participating after your baby was born interfere with your usual activities? Mean (SD)<break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.7 (0.8<xref><sup>h</sup></xref>)</td><td rowspan="1" colspan="1">0.7 (0.9<xref><sup>h</sup></xref>)</td><td rowspan="1" colspan="1">0.7 (0.5)</td><td rowspan="1" colspan="1">.53</td></tr><tr><td colspan="5" rowspan="1">How much difficulty did you have completing the study questionnaires? Mean (SD)<break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">0.3 (0.7)</td><td rowspan="1" colspan="1">0.4 (0.8)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How much difficulty did you have using a cell phone to complete the study questionnaires? Mean (SD)<break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.1 (0.4)</td><td rowspan="1" colspan="1">0.1 (0.4)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How much have you been annoyed with the number of alerts you have received in this study before your baby was born? Mean (SD)<break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.2 (0.5<xref><sup>h</sup></xref>)</td><td rowspan="1" colspan="1">0.3 (0.5)</td><td rowspan="1" colspan="1">0.0 (0.0<xref><sup>h</sup></xref>)</td><td rowspan="1" colspan="1">.63</td></tr><tr><td colspan="5" rowspan="1">How much have you been annoyed with the number of alerts you have received in this study after your baby was born? Mean (SD)<break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.3 (0.7)</td><td rowspan="1" colspan="1">0.4 (0.8)</td><td rowspan="1" colspan="1">0.2 (0.4)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">How difficult was it to notify the study staff of your child’s birth? Mean (SD)<break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">0.1 (0.7)</td><td rowspan="1" colspan="1">0.2 (0.7)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr><tr><td colspan="5" rowspan="1">Have you had any difficulties working with study staff? Mean (SD)<break/><break/><break/><break/><break/><break/><break/><break/></td></tr><tr><td rowspan="1" colspan="1"> W1</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> W12</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">—</td></tr><tr><td rowspan="1" colspan="1"> M5</td><td rowspan="1" colspan="1">0.0 (0.2)</td><td rowspan="1" colspan="1">0.1 (0.2)</td><td rowspan="1" colspan="1">0.0 (0.0)</td><td rowspan="1" colspan="1">>.99</td></tr></tbody></table>Discussion
Principal Results
We completed a prospective cohort study with individuals who did and did not have perinatal OUD, following them with robust data collection procedures. This included daily surveys and weekly face-to-face visits with collection of biological samples during the first 12 weeks postpartum with additional follow-up through postpartum month 5. We enrolled 70 participants during late pregnancy, and 51 (73%) completed the follow-up through postpartum month 5. Notably, more participants in the OUD– group completed follow-up compared to the OUD+ group (85% vs 68%, respectively). Additionally, despite the challenges faced in caring for a newborn paired with our robust data collection protocol, compliance with specific data collection modalities was moderately high in both groups (63%‐81%). Indeed, the daily survey compliance of approximately 80% during the follow-up period among OUD– is directly in line with the, on average, 80% compliance rates (range: 63%‐96%) observed in 27 studies using similar procedures during the perinatal period [55]. The OUD+ group had lower compliance overall, throughout the follow-up period for the data collection procedures, as well as a faster drop in compliance over time with regard to visit attendance. This is to be expected given the additional demands on the OUD+ participants (eg, caring for a high-needs infant, daily MOUD clinic visits). Moreover, during the first year of data collection, all participants faced additional challenges with the ongoing COVID-19 pandemic. Despite this, among a subset of participants, high levels of satisfaction were reported in both groups consistently across time. While this data collection protocol was burdensome with daily surveys plus weekly meetings and hormonal measurements and, thus, likely includes some selection bias due to the nature of individuals who are able to participate in this research (eg, those with more support at home, those more stable in recovery), it does provide an opportunity to inform future research on relapse prevention development.
The primary goal of this prospective cohort study is to examine the potential utility of hormones or infant caregiving activities to support postpartum OUD recovery (publications forthcoming). While there is growing evidence that hormones (eg, progesterone, estrogen, oxytocin) influence drug-taking behaviors, nearly all research has examined the effect of a single hormone in isolation at 1 or 2 time points [13-15]. Emerging research demonstrates that relative levels and temporal patterns of hormones may be more important than a single hormone value at an isolated time point. For example, changes in the ratio of progesterone to estradiol across two time points are more predictive of smoking behavior than either hormone alone at a single time point [56]. Given that hormones (1) are continuously in flux, especially during the perinatal period, and variations occur as a result of many factors, including specific infant caregiving activities, and (2) have a significant effect on several aspects of neurobiology, including drug reward and stress responses, assessing the effects of 1 or 2 hormones at 1 or 2 time points is insufficient.
With the daily surveys and weekly hormonal measurements, we will be able to examine the role of hormones and infant caregiving practices on OUD recovery-related outcomes with novel analytical approaches to model complex variable interactions both concurrently and across time. Forthcoming analyses addressing this goal will follow recommendations to handle missing data in longitudinal datasets, including the use of multilevel modeling frameworks that use all available data across repeated measures and maximum likelihood and imputation methods for relatively small sample sizes (eg, full information maximum likelihood, joint multiple imputation) [57-59]. Further, we will employ sensitivity analyses to assess potential selection bias and mitigate error [60-63] to further approximate observations to the target population.
While this study may not produce generalizable results, it can provide direction for future research. For example, if our observations suggest that higher levels of progesterone are protective against relapse risk, exogenous progesterone may be used to favorably modify progesterone during the postpartum period to reduce relapse risk, as was recently done to reduce postpartum cigarette smoking relapse risk [17]. Another scenario may include our observations suggesting that more close contact with infants is protective against postpartum opioid craving, in line with our prior work demonstrating that babywearing is linked to reduced urges to use substances [56]. Consequently, a follow-up study may examine the results of maternal babywearing on postpartum recovery outcomes similar to recent studies with nurses and mothers caring for infants with neonatal abstinence syndrome [6465]. A third example may be heightened estradiol or testosterone during postpartum may be linked to more cue-induced cravings. While the exogenous delivery of these hormones is not compatible with pregnancy or breastfeeding [6667], future research may instead use innovative approaches to monitor hormone pattern(s) or level(s) remotely [68] to proactively identify periods of heightened risk leading to the deployment of additional supports. This approach could also be applied to remotely monitor infant caregiving via smart baby carriers [68]. In sum, the data resulting from the study protocol described here, while limited, will yield informative preliminary results that can be further examined via a priori hypothesis testing approaches (eg, randomized control trials) with fully powered and diverse study samples to yield generalizable results and inform the development of additional postpartum OUD recovery support.
Beyond our primary goals, these data provide ample opportunities to explore novel topics in perinatal substance misuse and beyond. For example, we conducted comprehensive interviews of lifetime trauma exposure and resilience, as well as birth and breastfeeding experiences. This allows for mixed-method approaches to expand the understanding of these experiences prospectively during the perinatal period. Additionally, daily our participants reported on their mood, affect, and stress, as well as their craving for and use of other substances (eg, alcohol, cannabis, nicotine, or tobacco). Thus, we can explore the relationships between these variables, as well as in relation to baseline characteristics (eg, ethnicity, parity) and concurrent behaviors and activities (eg, sleep, involvement of others). Indeed, we are currently exploring the role of loneliness, isolation, and social support in OUD-related outcomes within this dataset (R21DA058364; Allen and Linde-Krieger). Overall, these data offer substantial opportunities to uncover novel relationships, increase our understanding of risk or protective factors of maladaptive behaviors during the sensitive perinatal period, and ultimately inform new approaches to enhance the health and well-being of mothers, infants, and families.
Limitations
Like every study, there are limitations. First, generalizability is limited given that these data were collected in a single US state, and the robust protocol may have been too burdensome for some individuals. Similarly, our eligibility criteria restricted our OUD+ group to those who were in treatment for recovery and expected to live with their infant. It is also possible that those who had lower cravings or better coping were less likely to discontinue their study participation. We also have a fair amount of missing data, as is common in prospective studies during the postpartum period with daily measurements [55]. These data may not be missing at random (eg, those with a high-needs newborn or those at higher risk for return to opioid misuse may be less likely to complete data collection; retention may have changed across the study due to the COVID-19 pandemic or protocol adjustments). It is possible that this will introduce bias and error into our observations. Finally, this study is underpowered to test hypotheses using traditional analytical approaches for causal modeling. However, our goal here is to generate new preliminary observations that will lead to fully powered trials that can adequately assess these relationships with diverse study samples and that utilize novel approaches to prevent opioid misuse. Despite these limitations, there are also substantial strengths, including an ability to temporally evaluate relationships; assessment of substance use with multiple sources (eg, prospective surveys, retrospective interviews); and numerous validated measures with rigorous, gold-standard approaches.
Conclusions
Overall, this prospective cohort study of those with and without OUD during the perinatal period resulted in moderately high retention and compliance, as well as high participant-reported study satisfaction, among a subgroup of participants. Consequently, these multidimensional data have high potential to inform future research on the challenges and opportunities of the perinatal period to support OUD recovery during the traditionally high-risk postpartum period.
Supplementary material
10.2196/77899Multimedia Appendix 1Lifetime trauma and resilience interview.
10.2196/77899Multimedia Appendix 2Investigator-created birth and breastfeeding interview.
10.2196/77899Multimedia Appendix 3Protocol completion by time point, modality, and group.
10.2196/77899Multimedia Appendix 4Investigator-created and modified versions of validated instruments.
10.2196/77899Multimedia Appendix 5Overview of study measures.
10.2196/77899Multimedia Appendix 6Description of study sample—completed phone screening interview (n=112).
10.2196/77899Multimedia Appendix 7Description of study sample—completed at least 1 postpartum visit (n=61).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Haight SC Ko JY Tong VT Bohm MK Callaghan WM Opioid use disorder documented at delivery hospitalization—United States, 1999-2014 MMWR Morb Mortal Wkly Rep Aug 1020186731845849 doi 10.15585/mmwr.mm 6731 a 1Medline 30091969 PMC 6089335 · doi ↗ · pubmed ↗
- 2Hirai AH Ko JY Owens PL Stocks C Patrick SW Neonatal abstinence syndrome and maternal opioid-related diagnoses in the US, 2010-2017 JAMA 011220213252146155 doi 10.1001/jama.2020.24991 Medline 33433576 PMC 7804920 · doi ↗ · pubmed ↗
- 3Auty SG Frakt AB Shafer PR Stein MD Gordon SH Severe maternal morbidity among pregnant people with opioid use disorder enrolled in Medicaid JAMA Netw Open 012202581 e 2453303 doi 10.1001/jamanetworkopen.2024.53303 Medline 39777443 PMC 11707626 · doi ↗ · pubmed ↗
- 4Terplan M Martin CE Premkumar A Krans EE Caring for pregnant and parenting women with opioid use disorder Wakeman SE Rich JD Treat Opioid Use Disord Gen Med Settings Springer International Publishing 2021203221 doi 10.1007/978-3-030-80818-1_14ISBN 978-3-030-80818-1 · doi ↗
- 5Winstanley EL Stover AN The impact of the opioid epidemic on children and adolescents Clin Ther Sep 201941916551662 doi 10.1016/j.clinthera.2019.06.003Medline 31303278 PMC 7017799 · doi ↗ · pubmed ↗
- 6Opioid Use and Opioid Use Disorder in Pregnancy UR Lhttps://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/08/opioid-use-and-opioid-use-disorder-in-pregnancy Accessed 23-11-2024
- 7Schiff DM Nielsen T Terplan M et al Fatal and nonfatal overdose among pregnant and postpartum women in Massachusetts Obstet Gynecol Aug 20181322466474 doi 10.1097/AOG.0000000000002734 Medline 29995730 PMC 6060005 · doi ↗ · pubmed ↗
- 8Correlates of treatment retention and opioid misuse among postpartum women in methadone treatment UR Lhttps://oce-ovid-com.ezproxy 1.library.arizona.edu/article/01271255-201904000-00012/HTML Accessed 23-11-202410.1097/ADM.000000000000046730418335 · doi ↗ · pubmed ↗