Non-surgical Management of Post-traumatic Elbow Stiffness Following a Distal Humerus Fracture: A Case Report
Rohit Gulati, Jyotsna Agarwal, Parveen Kaur

TL;DR
A 25-year-old man with elbow stiffness after a fracture improved significantly with a non-surgical hydro-dissection treatment.
Contribution
Demonstrates hydro-dissection as a minimally invasive alternative to surgery for post-traumatic elbow stiffness.
Findings
Pain-free elbow flexion improved from 50° to 90° within three days of treatment.
Patient reported better quality of life and increased independence in daily activities.
Hydro-dissection effectively addressed synovial thickening without surgery.
Abstract
This case study examines the non-surgical treatment of post-traumatic elbow stiffness following a distal humerus fracture. A 25-year-old male patient presented with significant pain and a severe restriction in elbow flexion nine months after his injury. The patient had a delayed presentation to the specialist, having previously undergone an unsuccessful closed reduction and manipulation by a local health care provider. The patient received a hydro-dissection procedure using a mixture of corticosteroids, hyaluronidase, and local anesthesia. Within three days of the treatment, he experienced improvement, with his pain-free elbow flexion increasing from 50° to 90°. The patient also reported a better quality of life and improved independence in daily activities. This case highlights hydro-dissection as a potential, minimally invasive, and effective alternative for treating synovial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
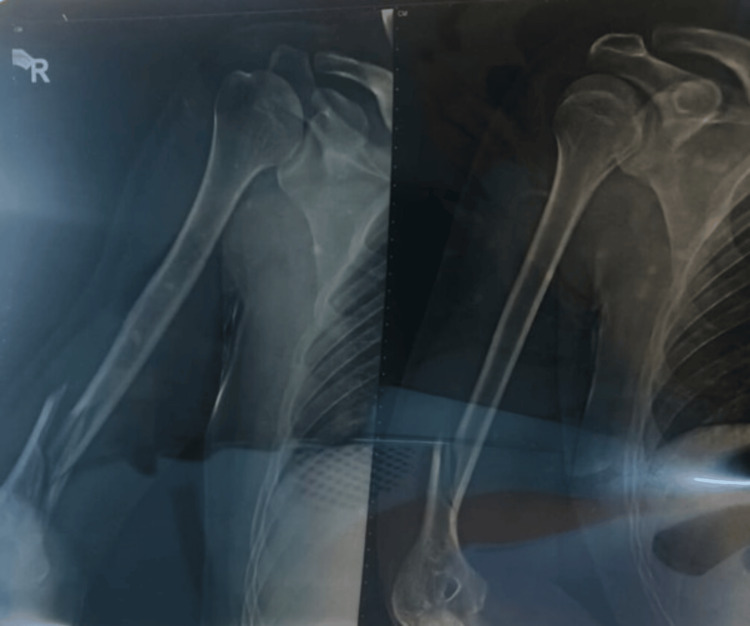 Figure 1
Figure 1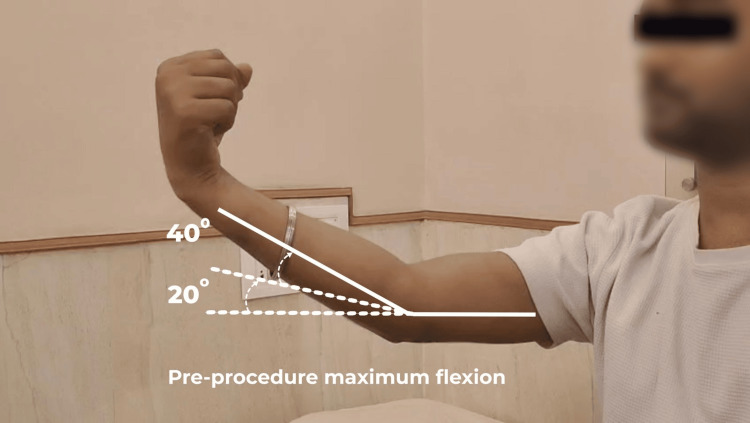 Figure 2
Figure 2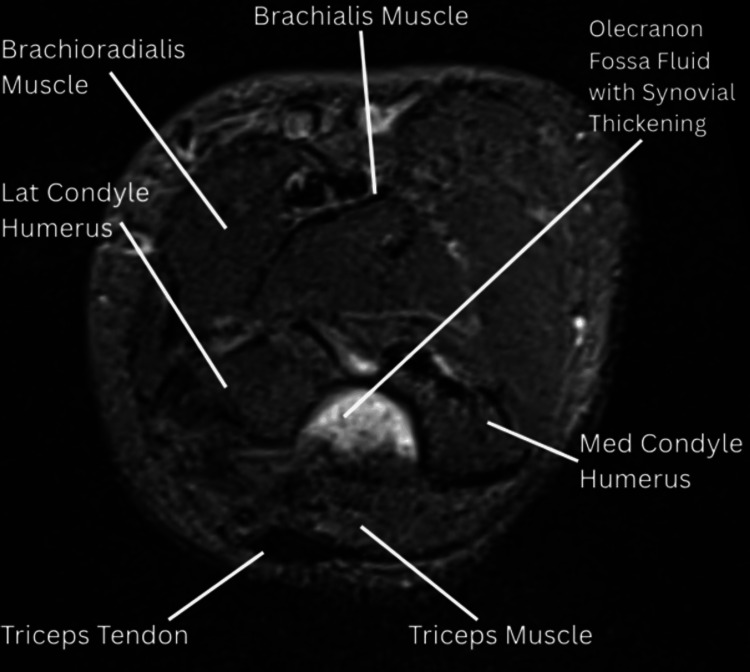 Figure 3
Figure 3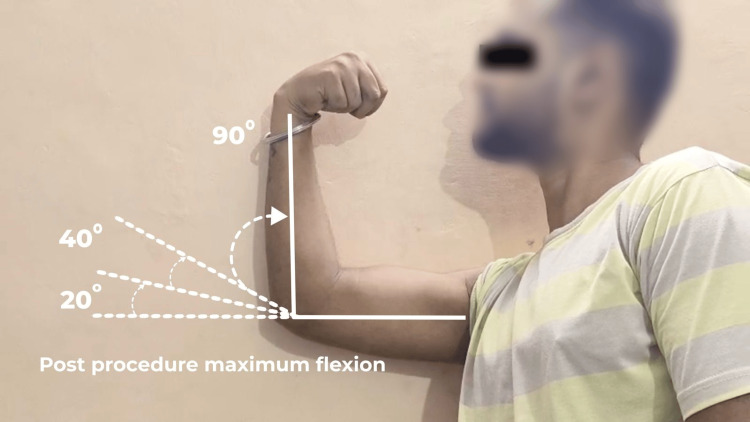 Figure 4
Figure 4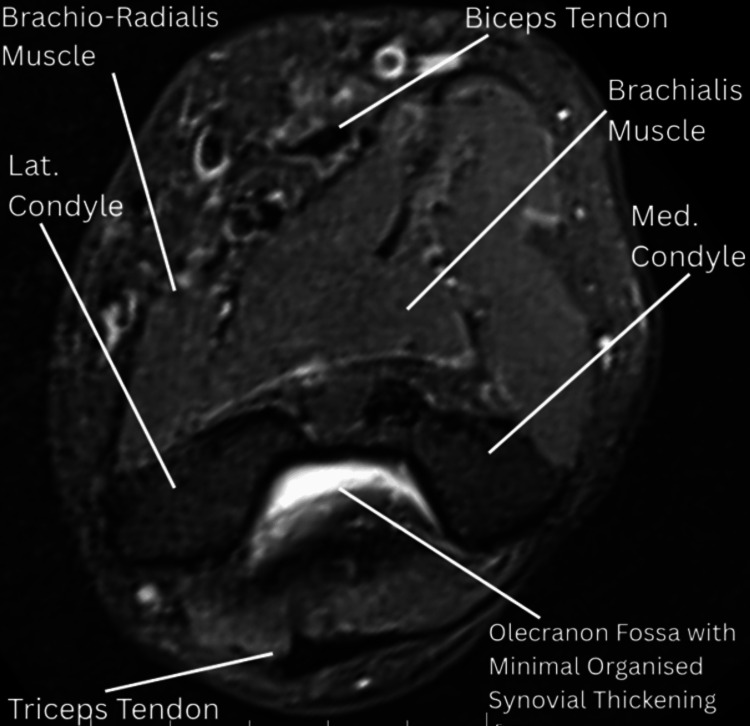 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
Synovial thickening and capsular fibrosis are common pathological responses after joint trauma and frequently contribute to elbow stiffness with resultant functional impairment [1,2]. Current clinical management of post-traumatic elbow stiffness is dominated by mechanical or structural approaches such as surgical capsulectomy and arthrolysis (open or arthroscopic), together with intensive physiotherapy and structured rehabilitation programs [1,2]. Several experimental approaches targeting inflammatory or fibrotic pathways have been explored in preclinical models or in inflammatory arthritides. Examples include the use of mast-cell stabilizers such as ketotifen, which has shown reduction in joint capsule fibrosis in rabbit models of post-traumatic contracture [3]; intra-articular relaxin-2, demonstrated to alleviate shoulder arthrofibrosis and reverse established fibrosis when delivered via sustained-release microparticles [4,5]; RNA interference-based strategies aimed at downregulating fibrotic or inflammatory gene expression in arthritic models [6]; and anti-TNF biologics, which have been shown to reduce synovial inflammation and remodeling in spondyloarthropathy [7].
These therapies, while promising in their respective experimental or disease-specific contexts, remain investigational for post-traumatic synovial fibrosis and are not established, routine treatments for elbow arthrofibrosis [1,2].
We describe a case where the patient with post-traumatic elbow stiffness having synovial thickening and joint effusion was managed with hydro-dissection of the joint nine months after the injury. The patient showed marked improvement in pain-free range of motion and resting pain within three days. To our knowledge, limited literature supports such delayed non-surgical management of post-traumatic elbow stiffness in humans.
The etiology of post-traumatic elbow stiffness is multifactorial, involving both soft tissue contractures and bony abnormalities. Capsular thickening, disorganized collagen, cytokine and enzyme changes, and early myofibroblast proliferation driven by the transforming growth factor-beta pathway are central to soft tissue contracture, particularly in the early post-injury phase [8]. Heterotopic ossification, characterized by the formation of mature lamellar bone in non-osseous tissue, creates a mechanical block to motion and is commonly triggered by trauma, burns, or surgery [8]. Extra-articular malunions, especially of the distal humerus, alter the anterior translation necessary for elbow flexion, while intra-articular malunions distort joint congruity and can cause periarticular fibrosis and ulnar nerve dysfunction [8]. Non-unions, whether intra- or extra-articular, contribute to stiffness through articular distortion, adhesions, and instability. Lastly, posttraumatic loss of articular cartilage may lead to arthrosis, with distal humerus fractures being particularly associated with long-term degenerative changes [8]
In this context, our successful use of hydro-dissection with corticosteroid, hyaluronidase, and local anesthetic suggests that such an approach may serve as a viable, less invasive, non-surgical alternative for patients with post-traumatic elbow stiffness.
Case presentation
A 25-year-old male presented with post-traumatic restriction of right elbow flexion. The patient had a road traffic accident nine months back, leading to a fracture of the lower one-third of the right humerus (Figure 1).
Radiographic image depicting a fracture of the right humerus.
The patient, being in a remote location, could not undergo any surgical intervention. He received closed reduction and elbow immobilization for up to 12 weeks. Following this, he started physiotherapy for the right upper limb, and the patient also used to do self-massage of the right elbow region. On examination, the right elbow showed an active range of motion from 20° to 40° and a passive range of motion from 20° to 50°. The patient was unable to perform routine activities requiring hand-to-face movement, such as brushing teeth, eating, or combing hair, and due to pain on elbow flexion, he was also unable to lift his baby in his lap (Figure 2).
Pre-procedure maximum flexion
Any attempt to flex beyond 40° was accompanied by severe pain, Visual Analogue Scale (VAS) 8-9 out of 10. The patient also had resting pain of VAS 3 out of 10. Muscular atrophy of the right biceps and triceps was noticed, with the right arm showing 4 cm less mid-arm circumference as compared to the left. The patient was previously a regular gym-goer and had no comorbidities or any relevant past history.
MRI imaging of the right elbow, done on the current OPD visit, demonstrated moderate intra- and periarticular fluid accumulation across all joint compartments, with associated synovial thickening and patchy marrow edema, suggestive of moderate synovitis (Figure 3). The injection was administered using the blind technique without USG/CT/MRI guidance.
MRI (pre-treatment): axial proton density fat-suppressed (PDFS) image demonstrating mild joint effusion in the olecranon fossa and mild synovial thickening.
The patient denied surgical intervention but agreed to a trial of hydro-dissection of the joint. Pre-procedure written informed consent was taken, and lignocaine sensitivity testing was done. Vitals monitoring and aseptic precautions were observed during the procedure. Under local anesthesia, hydro-dissection of the elbow joint and intra-articular and peri-articular soft tissues was done, using 30 ml of drug solution. Hyaluronidase was used as an adjuvant in the hydro-dissection mixture to enzymatically reduce hyaluronic-acid-mediated viscosity and to improve dispersion of the injectate, thereby facilitating mechanical separation of adhesions and enhanced delivery of corticosteroid and local anaesthetic. While this mechanism is biologically plausible and supported by studies of peri-articular hydro-dissection and adjunctive injections, high-quality evidence specifically demonstrating reversal of post-traumatic synovial thickening in the elbow is currently lacking; therefore, we present this as a less-invasive, investigational alternative to surgery in selected patients.
The drug solution consisted of injection methylprednisolone acetate 80 mg, 1% lignocaine, and 3000 IU hyaluronidase, with normal saline. Within 15 minutes post-procedure, the patient experienced a reduction in elbow stiffness and a reduction in pain on movement. Intermittent cold fomentation was done on the site for two days. Functional improvement was assessed on day three. Significant improvement in range of motion was noted, with pain-free passive flexion-extension from 20° to 90°. Pronation and supination were full and painless (Figure 4).
Post-procedure maximum flexion
There was no resting pain at this time. Fifteen days later, a repeat hydro-dissection procedure was done, similar to the first procedure. The dosing was adjusted between the two sittings. In the first procedure, the patient received 80 mg of Depo-Medrol, and in the second sitting (after three weeks) 40 mg of Depo-Medrol was administered. The total dose administered (120 mg) was well within the recommended annual safety limit of 3 mg/kg body weight (≈225 mg for this 75-kg patient). A three-week interval was maintained between the procedures to allow for excretion of the first dose (reported elimination time 12-16 days), thereby ensuring safety.
Minimal improvement was observed after the second procedure. The patient was advised to do gentle physiotherapy exercises. Following the intervention, a comprehensive physiotherapy regimen was initiated under supervision. The detailed physiotherapy protocol is attached in Appendix 1 for reference. At eight weeks post-procedure, the pain-free flexion up to 90° was maintained, and a 20% increase in muscle bulk in the right arm was noted. Restoration of function for daily activities was achieved, as reflected by the patient’s regained ability to perform routine tasks such as brushing, eating, and combing hair. The improvement in elbow flexion also enabled him to comfortably lift and hold his baby, resulting in significant functional and emotional satisfaction.
A follow-up (post-treatment) MRI done at eight weeks after the first procedure revealed a reduction in synovial thickening (Figure 5).
MRI (post-treatment): axial proton density fat-suppressed (PDFS) image demonstrating a marked reduction in diffuse synovial thickening, with only minimal organized residual synovial tissue remaining.
Discussion
This case highlights the potential value of a minimally invasive, non-surgical approach for managing post-traumatic synovial thickening. Ring et al. in 2006 evaluated 46 adults undergoing open elbow capsulectomy and demonstrated a mean improvement of 53° in ulna-humeral motion, with outcomes closely tied to pain and ulnar neuropathy [9]. Their study reinforces surgical release as the standard for refractory elbow stiffness. Similarly, Adithyaa et al. in 2025 reported successful open arthrolysis in a patient with severe post-traumatic stiffness and a flexion arc limited to 30°, secondary to malunion and heterotopic ossification [10].
Hydrodissection (or hydrodilatation) has been reported in other joints and entrapment syndromes with encouraging outcomes. In adhesive capsulitis (frozen shoulder), ultrasound-guided hydrodistention has produced sustained improvements in pain and shoulder range of motion [11-14]. In peripheral nerve entrapment syndromes such as carpal tunnel syndrome, hydrodissection with or without steroid or hyaluronidase adjuncts under ultrasound guidance has been used to release perineural adhesions; randomized controlled trials and systematic reviews suggest it is safe and can improve symptom scores and function over several months [15-17]. These examples support the potential generalizability of hydrodissection approaches to other anatomical sites, while emphasizing that application in post-traumatic elbow stiffness remains exploratory.
The authors emphasize that intra-articular deformities and bony blocks often necessitate open surgical access to restore function. In our case, despite similar mechanical restriction, the absence of major bony obstruction and patient preference enabled a non-surgical approach that offers a promising alternative, potentially disrupting adhesions, reducing inflammation, and enhancing joint mobility. Our patient received two sessions of hydrodissection. Repetitions of the procedure can be individualized as per the patient's presentation and improvement per session. While most clinical literature focuses on surgical management, preclinical models have also explored non-surgical mechanisms of contracture.
Adhesiolysis has been well-documented in the management of post-traumatic stiff elbow, predominantly through surgical or arthroscopic techniques. Open arthrolysis involving adhesiolysis of the capsule and periarticular soft tissues remains an established treatment modality for post-traumatic elbow contracture, enabling substantial restoration of joint mobility [18]. Arthroscopic arthrolysis has also demonstrated favorable outcomes, providing a minimally invasive approach for releasing intra-articular and capsular adhesions while minimizing soft tissue trauma [19]. Additionally, adjunctive strategies such as the intra-articular application of hyaluronan-based anti-adhesion gels during arthroscopic arthrolysis have been explored to mitigate postoperative adhesion recurrence and enhance long-term functional recovery [20]. Complementing these clinical insights, Dunham et al. developed a non-surgical rat model of post-traumatic elbow stiffness, wherein soft tissue injury followed by 42 days of immobilization without pharmacologic intervention led to persistent contracture characterized by capsular fibrosis and myofibroblast proliferation, underscoring the biological basis of post-injury joint stiffness. Our case employed targeted hydro-dissection using corticosteroids, hyaluronidase, and local anesthetic, resulting in rapid and sustained improvement in range of motion within three days. The hydrodissection mixture was intentionally formulated for complementary pharmacologic effects. The corticosteroid (Depo-Medrol) provides potent anti-inflammatory activity, attenuating synovial inflammation and capsular fibrosis; however, repeated use has been associated with potential adverse effects such as local tissue atrophy and systemic absorption-related complications [21]. Hyaluronidase enzymatically reduces hyaluronic acid-mediated viscosity, enhances tissue permeability and drug dispersion, and facilitates adhesiolysis-although its role in post-traumatic elbow stiffness remains investigational, and rare hypersensitivity reactions have been reported [22,23]. The local anesthetic component ensures immediate analgesia, enables comfortable hydrodissection, and supports early mobilization, though its duration of action is short and systemic toxicity can occur if inadvertently administered intravascularly or in excessive doses. Collectively, these agents act synergistically to release adhesions, reduce pain, and promote functional recovery, while emphasizing the need for further studies to validate their combined use in this context.
An increase in flexion from 50° to 90° might appear to be a moderate improvement of 40° flexion; however, it translates into meaningful enhancement in daily activities. An increase in flexion from 50° to 90° might appear to be a moderate improvement of 40° in range of motion; however, it translated into meaningful enhancement in daily activities. The ability to use his right hand, particularly to hold his baby in his lap, gave the patient great satisfaction and joy. This moderate improvement in elbow flexion has led to a remarkable improvement in the patient’s quality of life. There has been no improvement in the minimal restriction in elbow extension (fixed flexion deformity at 20°), and it also appears that further improvement in extension and flexion beyond 90° is not possible non-surgically in this patient. Strengths of this case report include the rapid clinical response, procedural safety, and technical simplicity.
Conclusions
This case demonstrates that in carefully selected patients of post-traumatic elbow stiffness, with synovial thickening and no bony obstruction, hydro-dissection of the elbow joint may offer an effective, minimally invasive management technique. In this case, hydro-dissection was performed using a combination of steroid, hyaluronidase, and local anesthetic. Further research in larger cohorts is needed to establish its long-term efficacy, and studies should also explore the feasibility of hydro-dissection as a first-line intervention in such cases, with surgical management reserved for non-responders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Post-traumatic elbow stiffness: pathogenesis and current treatments Shoulder Elbow Zhang D Nazarian A Rodriguez EK 3845122020 https://doi.org/10.1177/17585732187939033201023210.1177/1758573218793903 PMC 6974890 · doi ↗ · pubmed ↗
- 2The post-traumatic stiff elbow: a review J Clin Orthop Trauma Akhtar A Hughes B Watts AC 125131192021 https://doi.org/10.1016/j.jcot.2021.05.0063427733910.1016/j.jcot.2021.05.006PMC 8261251 · doi ↗ · pubmed ↗
- 3The mast cell stabilizer ketotifen reduces joint capsule fibrosis in a rabbit model of post-traumatic joint contractures Inflamm Res Monument MJ Hart DA Befus AD Salo PT Zhang M Hildebrand KA 285292612012 https://doi.org/10.1007/s 00011-011-0409-32217327910.1007/s 00011-011-0409-3PMC 3710138 · doi ↗ · pubmed ↗
- 4Intraarticular injection of relaxin-2 alleviates shoulder arthrofibrosis Proc Natl Acad Sci U S A Blessing WA Okajima SM Cubria MB 12183121921162019 https://doi.org/10.1073/pnas.19003551163116044110.1073/pnas.1900355116 PMC 6589647 · doi ↗ · pubmed ↗
- 5Minimally invasive, sustained-release relaxin-2 microparticles reverse arthrofibrosis Sci Transl Med Kirsch JR Williamson AK Yeritsyan D 0142022 https://doi.org/10.1126/scitranslmed.abo 335710.1126/scitranslmed.abo 3357 PMC 994876636223449 · doi ↗ · pubmed ↗
- 6Effects of infliximab treatment on rheumatoid synovial tissue J Rheumatol Suppl Tak PP 3134742005 https://www.jrheum.org/content/jrheumsupp/74/31.full.pdf 15742462 · pubmed ↗
- 7Anti-TNF (adalimumab) injection for the treatment of adults with frozen shoulder during the pain predominant stage protocol for a multi-centre, randomised, double blind, parallel group, feasibility trial NIHR Open Res Hopewell S Kenealy N Knight R 28220223788130710.3310/nihropenres.13275.2PMC 10593336 · doi ↗ · pubmed ↗
- 8Operative treatment of type C intercondylar fractures of the distal humerus: results after a mean follow-up of 2 years in a series of 18 patients J Shoulder Elbow Surg Pajarinen J Björkenheim JM 48521120021184514910.1067/mse.2002.119390 · doi ↗ · pubmed ↗