Strategies to Improve Adherence to Eye Care Referrals for Children following Vision Screening: A Scoping Review
Afua O. Asare, Amy Amoah, Patrice M. Hicks, Allison M. Howard, Teasha Luu, Aurora Rodriguez

TL;DR
This review explores strategies to help children follow up on eye care referrals after vision screenings, finding that communication and logistical support are most commonly used.
Contribution
The study synthesizes strategies to improve adherence to eye care referrals for children, highlighting gaps in evaluating their effectiveness in low-income countries.
Findings
Enhanced direct communication like phone calls and mailed notifications was the most frequently reported strategy.
Logistical support, such as transportation and pre-scheduled appointments, was also commonly used.
Effectiveness of these strategies remains under-evaluated, particularly in low-income countries.
Abstract
Vision screening plays a critical role in identifying potential vision disorders; however, its effectiveness is compromised when follow-up with eye care professionals is not completed. Up to 60% of children with abnormal vision screenings do not attend recommended appointments with eye care providers. This study aims to identify and synthesize the strategies to improve adherence to eye care referrals following abnormal vision screening tests. The Joanna Briggs Institute methodology was followed to conduct the scoping review. This review is part of a broader study exploring adherence to pediatric eye care referrals. A companion scoping review focusing on social risk factors of non-adherence has been submitted separately. Searches for relevant literature were performed across bibliographic databases and gray literature from their inception to July 2023, with an updated search in November…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
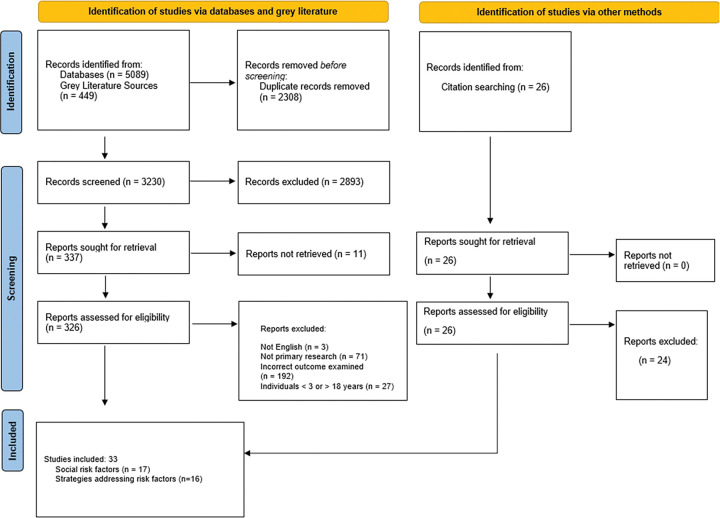 Figure 1
Figure 1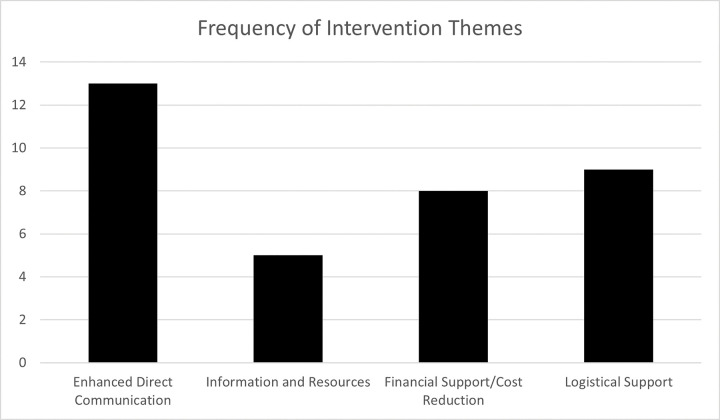 Figure 2
Figure 2- —National Institutes of Health Core Grant
- —National Eye Institute
- —National Institute of General Medical Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies
Introduction
To prevent long-term visual impairment, the early detection and treatment of vision disorders during childhood is essential.(1–3) Vision screening enables the early identification of vision disorders through referrals to eye care professionals for a comprehensive eye examination.(4) However, the effectiveness of vision screening programs is compromised when referrals to eye care professionals are not completed, preventing timely treatment for identified vision disorders. Vision screening is conducted in elementary schools, pediatric primary care, and/or other community-based settings in most countries.(1, 5)
In spite of the widespread use and established benefits of vision screening and comprehensive eye examinations, ensuring follow-up eye care after abnormal screening results remains a significant challenge. Studies show that as many as 60% of children do not attend recommended appointments with eye care providers following abnormal vision screening tests.(2, 3, 6, 7) Lower adherence to eye care appointments disproportionally affects children from socially disadvantaged populations, including racial and ethnic minorities, underserved rural communities, people with low socioeconomic status, and sexual and gender minorities.(4, 8–11)
Efforts to address low adherence to eye care appointments include developing evidence-based strategies and interventions. A previous study reviewed strategies to improve adherence to eye care professionals for adult populations.(12) Strategies reported in the study included patient navigation and prescheduled appointments. It is however unknown if these strategies have been used in pediatric populations and their impact on referral adherence for children.(12) These gaps highlight the need for a comprehensive synthesis of strategies for improving referral nonadherence in children. The objective of this study is to identify strategies from the existing literature to improve referral adherence for comprehensive eye exams by eye care professionals following abnormal vision screening tests for children.
Methods
Protocol and registration
This scoping review followed the methodology outlined by the Joanna Briggs Institute (JBI) (6) for scoping reviews and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.(7) This review is part of a broader study exploring adherence to pediatric eye care referrals. A companion scoping review focusing on social risk factors of non-adherence has been submitted separately, with adaptations to address a distinct research objective focused on intervention strategies. Searches were conducted across bibliographic databases (PubMed, Embase, CINAHL, PsycINFO, Scopus, and Web of Science) and gray literature were searched from their inception to July 2023, with an updated search performed in November 2024. The protocol for this review was registered with the Open Science Framework. As this study involved analysis of previously published sources with de-identified data and did not involve interaction with human participants, ethical approval and informed consent were not required and was exempt from the University of Utah Institutional Review Board.
Search Strategy
The review team met with a librarian (AMH) in June 2023 to develop a comprehensive search strategy for PubMed. The strategy was subsequently adapted for use across additional electronic databases. The initial literature search was conducted in July 2023 covering studies available from the inception of the respective databases up to July 2023. An updated search was conducted in early November 2024. The search aimed to identify relevant studies that examined social risk factors of and strategies to improve referral adherence following abnormal vision screenings in children. Search terms included keyword and controlled vocabulary, where applicable, and their synonyms for the following concepts: child, vision screening, referral adherence, and eye care professional. The complete search strategy used for PubMed can be found in Appendix I.
Eligibility criteria
Studies were selected based on specific characteristics including the type of target population, outcomes and study design. Screening for eligibility criteria was conducted in two phases: an initial review of the title/abstract followed by a full-text assessment, as detailed in Table 1. Eligible studies included vision screening conducted in any setting, e.g., school, pediatric primary care, or another community-based setting. There were no limitations on date of publication or country of publication; however, studies not published in English were excluded (Table 1).
Information sources
Searches were conducted across multiple electronic databases, including PubMed (NLM), Embase (Elsevier), CINAHL (EBSCO), PsycINFO (EBSCO), Scopus (Elsevier), and Web of Science (Clarivate). Sources of grey literature were OAIster, NIH RePORTER, Trials Register of Promoting Health Interventions (TRoPHI), National Center for Children’s Vision and Eye Health website, American Association for Pediatric Ophthalmology and Strabismus website, Conference Proceedings Citation Index, and Cochrane CENTRAL Register of Controlled Trials. Additionally, a review of citations in included studies and relevant reviews was performed.
Evidence selection
Search results were initially collected in EndNote for deduplication and then uploaded into the Rayyan-Intelligent Systematic Review program (Rayyan Systems Inc., Cambridge, MA) to review retrieved articles. The article selection process followed a two-step approach: a review of titles and abstracts, followed by a review of full-text articles. Eligibility was assessed according to the criteria described earlier. All reviewers (AOA, PMH, AA, and AR) were involved in a pilot test on a random 10% of full-text articles retrieved from the initial search to ensure inter-rater reliability (IRR). The reviewer team screened the articles using the initial eligibility criteria outlined in our protocol and made minor changes to the inclusion criteria, such as the addition of studies involving caregivers of children, and clarity on the type of vision screening programs. Screening began once at least 75% agreement had occurred between all four reviewers on the pilot test. Each study was independently assessed at both stages by two reviewers at each level (title, abstract, and full-article review). Discrepancies were resolved through discussion or by a third reviewer (AOA or PMH).
Study selection and data collection process
Data from studies that were included in the review were extracted using a pilot-tested form. Key variables collected included author, year of publication, geographical context (i.e., city/state, country), World Health Organization income level, target population, screening setting, age range, and sex/gender, race, and ethnicity distributions (Appendix II)
Synthesis of findings
Data extracted from full-text studies selected for inclusion were synthesized following a three-stage process: inductive coding, theme generation, and theme mapping. Inductive coding was conducted using descriptive coding labels created inductively by one reviewer (AA) to allow patterns and preliminary subthemes related to social risk factors and strategies to emerge from existing published knowledge. The codes were reviewed and confirmed by a second reviewer (AOA) to ensure accuracy.
Theme generation involved the identification, analysis, and interpretation of patterns within the data set (‘thematic synthesis’). Coded data was organized in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) by one reviewer (AA) into thematic groups, which were subsequently reviewed by another reviewer (AOA) to confirm consistency. The approach of theme generation facilitated the synthesis of findings to extend beyond the original studies, offering analytic insights. During the generation of themes, the reviewers consistently considered the study’s overarching research question and objectives.
Results
The initial search identified 5,538 studies through databases and grey literature, with 26 additional records identified through citation searching. After 2,308 duplicates were excluded, 3,230 studies were screened at the level of the abstract and title. An additional 2,893 citations were removed in the title and abstract screening as not relevant. During the full-text screening stage, 337 articles were required for retrieval, of which 11 were not available for retrieval. Of the 326 full-text articles assessed for eligibility, 31 studies met the inclusion criteria and were included in the review. Citations of included studies were searched to identify any additional studies, and two were subsequently included, making a total of 33 included studies. Overall, 16 studies assessed strategies to improve rates of referral adherence (Fig. 1). Seventeen studies assessed social risk factors following an abnormal vision screening test and have been reported in a separate manuscript.
Of the included studies that assessed strategies to overcome referral nonadherence, 14 (88%) studies targeted vision screening programs conducted in schools (15–28), and two (13%) studies targeted programs in health care settings. (29, 30)
Vision screening programs in two studies (13%) targeted preschool-aged children (2 to 5 years) [16]; four studies (25%) targeted school-aged children (6 to 19 years) [22, 23, 25, 26]; and nine studies (56%) targeted both preschool- and school-aged children (2 to 19 years).(15, 17, 20, 21, 24, 27, 28, 30, 31). Race was reported in three (19%) studies, (22, 26, 30) and ethnicity was reported in four (25%) studies.(16, 17, 22, 24) Nine studies targeted underserved or socially disadvantaged populations.(15, 16, 18, 22, 24, 25, 28, 29, 31) Study designs varied with 10 included studies being intervention (63%) (15, 16, 18, 20–22, 24, 25, 30, 31) compared to three descriptive (19%) (17, 23, 28) designs to assess strategies to improve referral adherence. Retrospective design was used in two (13%) studies (32, 33), and one (6%) study implemented a cluster-randomized controlled trial. (27) In total, 12 studies (75%) were conducted in high income countries [United States (US) (15–18, 21, 22, 24–26, 29–31)], and four (25%) studies were conducted in an upper middle-income country [(Peru, (20) Brazil, (23) China (27, 28)]. The most frequently reported strategy for improving referral adherence was enhanced direct communication reported in 13 studies (81%) (Fig. 2).(16, 17, 21–31). This was followed by logistical support (15, 17, 18, 20, 24, 27–29, 31) in nine (56%) studies and financial support (15, 16, 18, 20, 21, 28, 31, 33) in eight studies (50%). The least reported strategy was related to information and resources (16, 20, 21, 25, 27) in five studies (31%).
Direct Communication
Enhanced direct communication was implemented in vision screening programs reported by 13 studies (81%), (16, 17, 21–31) that were conducted in upper-middle [Brazil, (23) China (27, 28)] and high-income countries [United States (US), (16, 17, 21, 22, 24, 25, 30–33)]. Particularly, organizers of vision screening programs in nine studies reported the placement of phone calls to caregivers to notify them of referrals after a vision screening test and encourage adherence. Another popular strategy reported in five studies was helping caregivers to schedule referral appointments (e.g., answering caregivers’ questions about covering the cost of the follow-up appointment, type of eye care provider to see, and where to find these providers), and coordinating these appointments. In some cases, pre-arranged appointments with eye care professionals were provided. (Table 3)
Information and Resources
Five studies (31%) conducted in high [US (16, 21, 25)], and upper-middle income [Peru,(20) China (27)] countries reported the provision of additional information and resources to motivate caregivers to adhere to referrals, and simplify the process of referral adherence. The resources and information included lists of pediatric eye care professionals, the insurance the provider accepted, and contact information to facilitate appointment scheduling. (16, 21) Suchoff et al. created opportunities for optometrists to meet one-on-one with caregivers of children identified with severe vision impairment to amplify the importance of adhering to the referral. (25) A vision screening program in China offered comprehensive eye examinations for referred children, delivered by local nurses, ocular technicians, and ophthalmologists. These providers were trained by specialists from the Zhongshan Ophthalmic Center, a renowned eye clinic affiliated with Sun Yat-sen University. To promote caregiver adherence to referrals, program organizers emphasized the training received by these providers from Zhongshan experts, who would also be present at the referral clinic to oversee the management of any diagnosed eye conditions.(27) (Table 3)
Financial Support
Vision screening programs reported in eight studies (50%) provided financial support (15, 16, 18, 20, 21, 28, 31, 33) to improve adherence to referral eye exams. The vision screening programs were conducted in high-income (US) (15, 16, 18, 21, 31, 33) and upper-middle-income [China, (27) Peru (20)] countries. To overcome the financial constraints related to referral eye exams for families, the most popular strategy of financial support was free comprehensive eye exams in the same location or within proximity to the vision screening. (15, 18, 28) A study conducted in rural Peru trained teachers to perform basic vision screening of students. (20) Children with abnormal vision screening tests were examined onsite by an optometrist at school. Adherence rates were not reported, but a high follow-up rate with onsite eye exams was implied. (20) Other strategies to provide financial support include the use of social workers to assist families in enrolling in affordable health insurance programs, (20, 33) vouchers for transportation to referral appointments, (20, 33) and financial subsidies for glasses and treatment of eye disorders. (20) A novel approach by Hark et al. was to provide two free movie tickets to caregivers who adhered to referral appointments with eye care professionals for their children. (31) (Table 3)
Logistical Support
Logistical support was used to improve adherence in nine studies (56%) from upper-middle [China, (27, 28) Peru (20)] and high-income countries [US, (15, 17, 18, 24, 31, 33)]. The most frequently used method was assistance with scheduling and coordinating referral eye appointments to include providing pre-arranged appointments with eye care professionals. (17, 24, 27, 31, 33) Also mentioned in five studies was the provision of comprehensive eye exams on the same site as (or within close proximity to) the vision screening to encourage adherence to referral eye appointments. (17, 24, 27, 31, 33) In addition to this, support for transportation (vouchers and covering cost of transportation), (20, 33) and reserved slots at eye clinics to expedite referral appointments had been strategies employed in prior studies. (31)
Rates of Referral Adherence
In total, 10 studies (63%) reported rates of adherence pre- and post-strategy intervention, (18, 20–24, 27, 28, 30, 33) while four studies reported rates of adherence post-intervention only. (16, 25, 26, 31) The highest rates of adherence were 96% (an increase from 67% pre-intervention) in the US-based study by Rodriguez et al., followed by 92% (an increase from 82% pre-intervention) in the Peru-based study by Latorre-Arteaga et al, and 91% in the study by Yawn et al. (26) The lowest rate of adherence of 43% in a study by Zhang et al. conducted in China. (28) Rodriguez et al. and Latorre-Arteaga et al. used multiple strategies to improve rates of referral adherence. Specifically, Rodriguez et al. used direct communication (i.e., phone calls to notify and encourage adherence to follow-up appointments) and logistical support (i.e., assistance with scheduling and coordinating follow-up appointments) strategies. (24) Latorre-Arteaga used information and resources (i.e., written health education materials for caregivers), and financial/logistical support (i.e., social workers’ assistance with enrolling in health insurance, transport vouchers, and subsidies for treatment and glasses). (20) Yawn et al., on the other hand, used one communication strategy, i.e. phone calls to notify and encourage adherence to follow-up appointments. (26) In the screening program conducted in China reported by Zhang et al., the lowest rate of referral adherence (43%) was reported despite the use of multiple strategies to improve referral adherence, specifically, financial/logistical support (i.e., free comprehensive eye exams and prescription glasses within proximity of vision screening) and communication strategies (i.e., phone calls to notify and encourage follow-up eye exams).
The highest increase in the rates of adherence to referrals post-intervention was 57% reported in the study by Dotan et al., (33) followed by a 40% increase in adherence in the study by Kripke et al., (30) and a 37% increase in the study by Neville et al. (22) The vision screening programs described in these studies employed different strategies to improve rates of referral non-adherence. (22, 30, 33) For instance, in the study by Dotan et al., they used communication, financial, and logistical support strategies, specifically, social workers, transportation vouchers, and the collection of multiple contact numbers for the caregivers of children who were referred. (33) In the study by Kripke et al., they used a single communication strategy, specifically, sending letters to parents and family physicians to inform them of the referral and need for a comprehensive eye exam. (30) The program in the study by Neville et al. also used two communication strategies; specifically, follow-up phone calls to caregivers and a detailed informative letter (separate from the standard referral notification). (22)
Discussion
This scoping review synthesized published evidence on strategies designed to increase adherence to pediatric eye care referrals following abnormal vision screening results. Across the 16 included studies, (13–28) direct communication with caregivers emerged as the most frequently implemented approach to improve referral adherence, (14, 15, 18, 19, 21, 22, 24–30) often combined with logistical or financial supports to address common barriers.
Gaps in the Literature
None of the included studies reported strategies to improve referral adherence in lower-middle and low-income countries. This lack of studies highlights a significant gap in our understanding of the availability and types of strategies in settings where resources may be limited despite the high burden of vision impairment. (31) The limited research in eye care topics in lower-middle and low-income countries. (32–34) may reflect the overall lower investment in global health research. (35–37)
Free Comprehensive Eye Exams
Free comprehensive eye exams were frequently offered as a means of financial and logistical support to improve referral adherence. However, the impact of free comprehensive eye exams on referral adherence was mixed. In the study by Chu et al., which provided on-site free comprehensive eye exams in low-income schools by an optometrist, only 52% of children returned consent forms, and adherence rates were reported as similar to traditional referrals. (13) The Wills on Wheels Mobile Eye Unit provided follow-up eye exams by pediatric ophthalmologists at school for children referred by an optometrist with positive feedback from school nurses. (16) The presence of the mobile eye unit led to a statistically significant improvement in follow-up rate from a historical rate of 53% to an improved rate of 62%. However, in rural China, vision centers established to offer free eye exams and a pair of glasses for children while increasing access to comprehensive eye exams, resulted in only 43% of referred students visiting vision centers.(16)
Impact of Strategies on Referral Adherence
Strategies implemented had varying impact on adherence to referrals for children with the rates of adherence ranging from 43–96%. The highest increase in adherence pre and post implementation of a new strategy was 57%. The rate of adherence did not appear to be additive based on the number of strategies employed. That is, employing more than one strategy did not translate to higher rates of adherence. While communication strategies were the most frequently used, it remains unclear whether it had greater impact on rates of adherence compared to other strategies. Improvements in the rates of adherence may depend on the target population and confounding factors such as race and ethnicity, geography, and socioeconomic status. Causal inferences of the effect of strategies on adherence to referrals cannot be drawn using scoping review methodology. To draw inferences and therefore assess the effectiveness of strategies on referral adherence, alternative methodologies such as systematic reviews, meta-analyses or randomized controlled trials are needed.
Comparisons to Prior Studies
Our companion study indicated that the most common social risk factor for referral nonadherence is a lack of affordability and awareness. Therefore, the results of this current study reflect that of the prior, given that communication, financial, and logistical support were the most frequently reported strategies. The study results also closely reflect that of Zeng et al. who reported health interventions to increase follow-up rates for ophthalmology eye exams following vision screening in the community. (12) The study population in the study by Zeng et al. was adult patients with diabetic retinopathy, glaucoma, refractive error, or cataract, and the most frequently reported interventions were free or subsidized follow-up eye exams (financial support), and reminder phone calls (logistical support). Other interventions identified in the Zeng et al., study included prescheduled ophthalmology appointments (logistical support), transportation assistance (logistical/financial support), patient education (communication), and patient navigators (logistical support). Rates of adherence ranged between 38 and 83%. The highest follow-up rate of 83% was reported in a study by Hark et al., who used patient navigators (logistical support) to improve follow-up to ophthalmology appointments.(38) Patient navigators have been used widely in various medical specialties, including ophthalmology in adult populations (38–42) with no evidence of their effectiveness for vision screening programs in pediatric populations. Future studies should explore the effectiveness of the abundance of health interventions, including patient navigators, to improve referral adherence in vision screening programs targeted specifically to children.
Strengths and Limitations
Strengths of this study include its novelty, and its robust and systematic approach. To the best of our knowledge, it is the first study to identify strategies to improve referral adherence for children following abnormal vision screening tests, regardless of the screening setting or disease focus. Despite its strengths, the limitations of this study are consistent with JBI methodology and need to be considered. First, the quality of included studies was not assessed. Consequently, the risk of bias within individual studies cannot be commented on, which may affect the strength of the evidence synthesized. Also, had an assessment of the quality of included studies been conducted, additional gaps in knowledge may have been elucidated. Similarly, we cannot assess the effectiveness of strategies identified in prior studies without employing a systematic review or meta-analysis. Also, the heterogeneity of included studies, combined with the exclusion of non-English literature, may have led to gaps in the evidence captured. Finally, despite using a robust and systematic approach to search the literature, it is possible that some relevant studies may not have been selected for inclusion.
Conclusion
Many strategies—most commonly direct caregiver communication—have been implemented to enhance referral adherence among children flagged by vision screening programs. Future work should rigorously evaluate the effectiveness of these strategies using randomized controlled trials or in systematic reviews and meta-analysis. This knowledge will inform the development of scalable, evidence-based solutions that can prevent avoidable childhood vision loss.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mema SC, Mc Intyre L, Musto R. Childhood vision screening in Canada: public health evidence and practice. Can J public health = Revue canadienne de sante publique. 2011;103(1):40–5.
- 2Schuster AK, Elflein HM, Diefenbach C, Gräf C, König J, Schmidt MF, Recommendation for ophthalmic care in German preschool health examination and its adherence: Results of the prospective cohort study ikid S. P Lo S ONE. 2018;13(12):e 0208164.30507974 10.1371/journal.pone.0208164 PMC 6277132 · doi ↗ · pubmed ↗
- 3Uwemedimo OT, Arpadi SM, Chhagan MK, Kauchali S, Craib MH, Bah F, Compliance with referrals for non-acute child health conditions: evidence from the longitudinal ASENZE study in Kwa Zulu Natal, South Africa. BMC Health Serv Res. 2014;14:242.24888212 10.1186/1472-6963-14-242PMC 4067123 · doi ↗ · pubmed ↗
- 4World Health Organization. Closing the Gap: Policy into Practice on Social Determinants of Health: Discussion paper for the World Conference on Social eterminants of Health. Rio De Janeiro, Brazil; 2011.
- 5Asare AO, Malvankar-Mehta MS, Makar I. Community vision screening in preschoolers: Initial experience using the Plusoptix S 12C automated photoscreening camera. Can J Ophthalmol. 2017;23.
- 6Aromataris ELC, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis 2024 [.
- 7Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, PRISMA Extension for Scoping Reviews (PRISMA-Sc R): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.30178033 10.7326/M 18-0850 · doi ↗ · pubmed ↗
- 8National Institute on Minority Health and Health Disparities. Minority Health and Health Disparities Definitions: U.S. Department of Health & Human Services, National Institute of Health; [Available from: https://www.nimhd.nih.gov/resources/understanding-health-disparities/minority-health-and-health-disparities-definitions.html#:~:text=NIH%2Ddesignated%20populations%20that%20experience,Underserved%20rural%20communities