Artificial Intelligence Enhanced Electrocardiogram Analysis for Age and Sex Classification in Youth
Honggen Zhang, Mohammad Zaeri-Amirani, Mojtaba Abolfazli, Narayana P. Santhanam, June Zhang, Anders Høst-Madsen, Chieko Kimata, James C. Perry, Andras Bratincsak

TL;DR
This study uses machine learning to improve ECG analysis in children and adolescents by creating age- and sex-specific standards.
Contribution
The novel use of machine learning models to derive age- and sex-specific ECG standards in youth.
Findings
Support vector machines achieved the highest accuracy in predicting age and sex from ECG data.
Key ECG features like heart rate and QRS duration were most predictive of age and sex.
Age-group classification improved significantly when allowing one-group misclassification.
Abstract
Electrocardiogram (ECG) values vary significantly across age and sex, particularly during childhood and adolescence. While age- and sex-specific ECG standards exist, they often fail to capture complex multi-dimensional relationships and have not been applied in machine learning (ML) enhanced ECG analysis. Accuracy of automated ECG analysis in clinical practice improved significantly by applying ML models, however there is a paucity of such studies in the pediatric population. Our aim was to create age- and sex-specific standards for children by ML modeling. We analyzed 29,408 curated resting 12-lead ECGs from healthy subjects aged 0–21 years using 177 digitized ECG variables combined with various ML models including regression and classification analyses and semi-supervised neural networks. Primary outcome variables were age and sex. Model performance was evaluated using F1-score,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
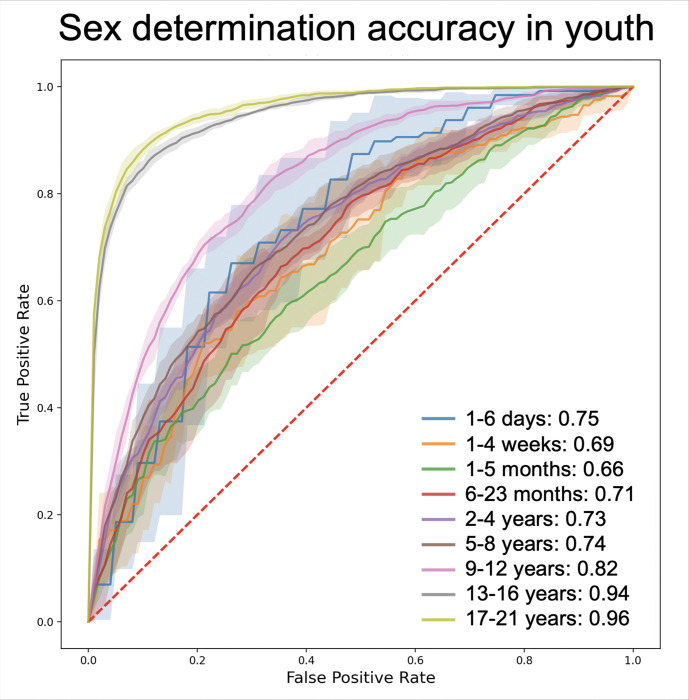 Figure 1
Figure 1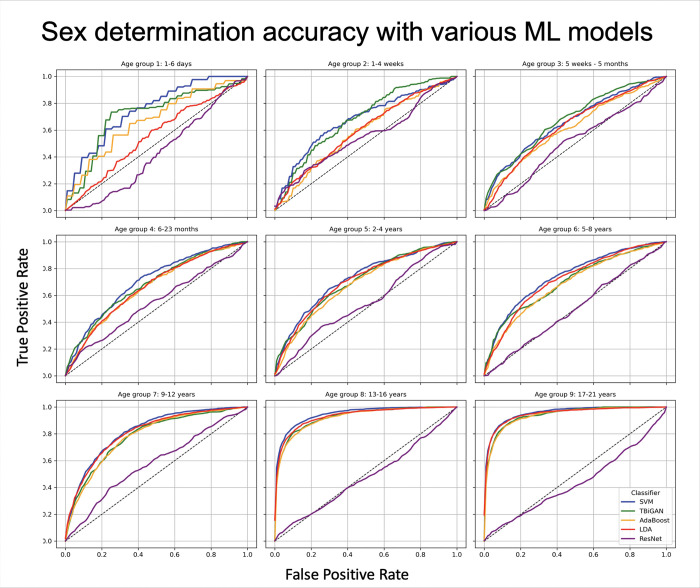 Figure 2
Figure 2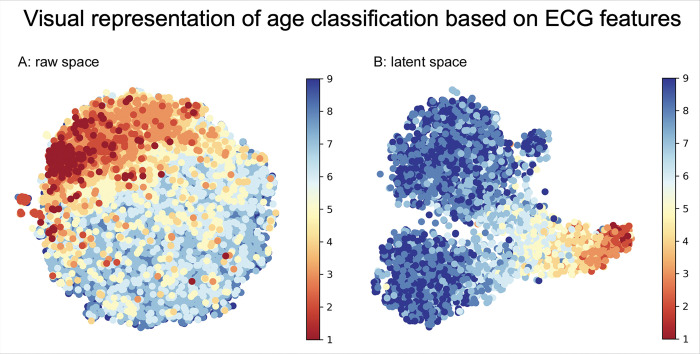 Figure 3
Figure 3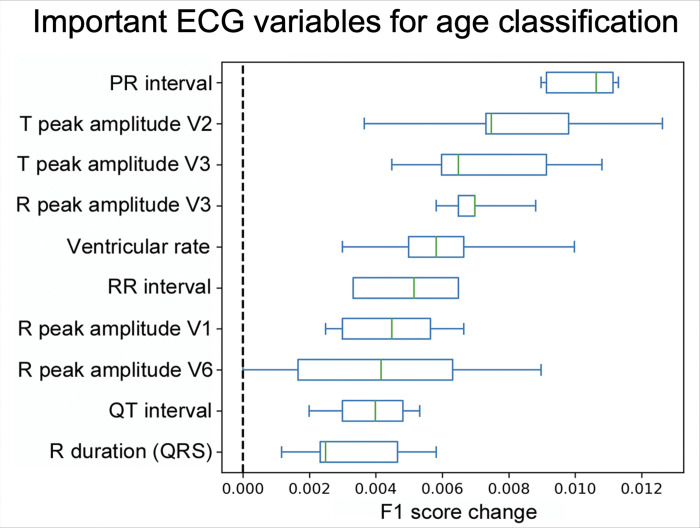 Figure 4
Figure 4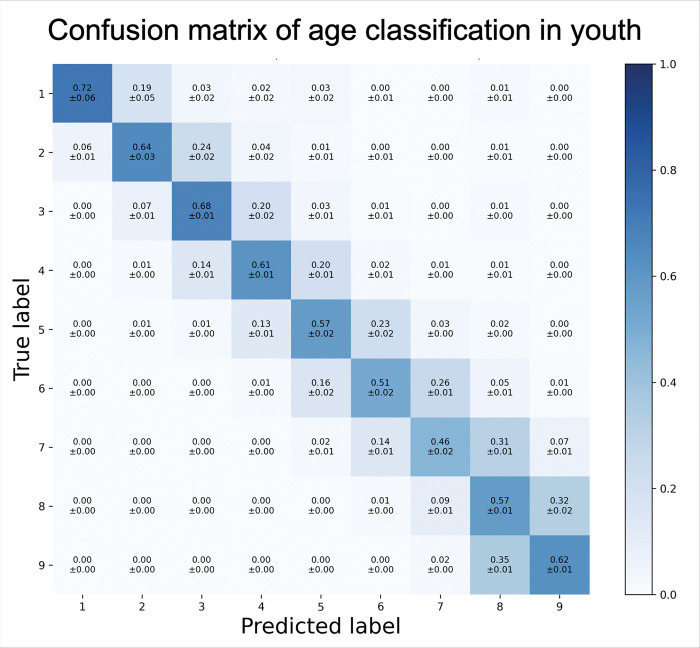 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Effects of Exercise · Cardiac electrophysiology and arrhythmias · Heart Rate Variability and Autonomic Control
Introduction
Since its invention by Einthoven in 1898, the electrocardiogram (ECG) has been one of the most important screening and diagnostic tests for heart problems [1] However, ECG analysis with the ability to indicate underlying cardiac disease states has historically relied upon the inherent biases and errors of physician interpretation based on standards derived from very few healthy subjects. In pediatric and adolescent populations, ECG interpretation is further hindered by the distinct challenges due to the rapid and profound physiological changes that occur from birth through young adulthood. These developmental changes affect ECG waveform morphology and timing, reflecting underlying alterations in heart size, autonomic tone, ion channel function, and conduction pathways. Detailed assessment of the largest historical pediatric cohort of normal ECGs recently allowed us to understand the granularity of these changes in the parameters of ECG variables across childhood [2]. Yet, these standards are primarily based on summary statistics of isolated ECG variables and do not fully capture the complex, multivariate patterns embedded within the high-dimensional ECG signal. Recognizing these dynamic and complex features is essential for accurate clinical interpretation.
Recent advances in machine learning (ML) have ignited the development of a novel field: artificial intelligence (AI) enhanced ECG analysis [3–5]. These ML models offer the potential to leverage the full complexity of data in ECGs, and can integrate numerous ECG features simultaneously, uncovering latent patterns, and improving the granularity of physiological modeling. Importantly, establishing ML models that can accurately infer age and sex based solely on ECG data is a critical step toward developing adaptive, context-aware diagnostic tools. These models can identify subtle electrophysiological signatures correlated with demographic factors, thus providing a normative framework that enhances detection of pathological deviations. AI-enhanced ECG analysis has been used for the detection of ventricular dysfunction and hypertrophic cardiomyopathy [6–8] and was also able to model the age and sex of adults and estimate a biological or cardiac age of a person [9–10]. However, these studies were performed in adults. There is a paucity of data of AI-enhanced ECG analysis in children, complicated by the profound changes in the ECG that occur between 0–21 years of age. Hypertrophic cardiomyopathy (HCM), left ventricular dysfunction and recently, congenitally corrected transposition of the great arteries have been successfully analyzed by ML models with reasonable detection rate [11–13]. However, other less common heart conditions have not been modeled by AI in children. ECG analysis in children and youth has a unique importance in screening for rare heart conditions, congenital heart defects and inherited arrhythmia syndromes [14–17], but this screening cannot be performed in an automated model, if there is no definition of age-and sex-specific normal standards. To date, AI-generated age- and sex-specific ECG standards for children and adolescents have not been developed, limiting the application of automated models for pediatric cardiac screening.
This study aims to evaluate multiple supervised and semi-supervised ML architectures to classify age groups and sex from ECG features of pediatric and young adult individuals. By developing age- and sex-classification, we aim to establish a foundation for automated AI-enhanced ECG analysis leveraging age- and sex-specific standards for children and young adults.
Methods
ECG data source and study population
This study used a large, curated cohort of ECGs from subjects with no known heart condition. The cohort, previously validated and published (Bratincsak et al, Circ AE, 2020) included ECGs collected retrospectively from patients aged 1 day to 21 years at Hawaii Pacific Health and Rady Children’s Hospital San Diego between 2012 and 2022 (n = 70,816). ECGs were obtained for a variety of clinical reasons, including evaluation of heart murmur, irregular heartbeat, syncope, dizziness, bradycardia, tachycardia, fever, screening for certain diseases, and for sports pre-participation screening. ECG from patients with congenital or acquired heart conditions, history of heart surgery, arrhythmia syndromes, pacemakers, or duplicate ECGs from the same patient within the same age-group were excluded from the study (n = 31,278). The stringent exclusion criteria created a curated cohort of ECGs from children and adolescents with no evidence of heart defect or cardiac anomaly on a more than 7-year average follow-up. All ECGs were performed in resting supine position using GE MAC 5500 HD ECG systems (General Electrics, Houston, TX) at 500 Hz sampling frequency with standardized voltage (10 mm = 1 mV) and speed (25 mm/s). Digitized ECG values were exported from the GE Muse v9 system. ECGs were excluded from the final analysis if they had technical errors, lead reversal, poor baseline, or missing lead information (n = 10,130), resulting in a final cohort of 29,408 complete ECGs. The study was approved by the Hawaii Pacific Health Research Institute and deemed exempt from further Institutional Review Board approval due to the retrospective nature of the analysis.
ECG variable selection and processing
ECG variables were pre-selected based on expert physician input and prior established standards. We included 177 ECG variables (features) in the analysis of the ECGs, such as: P, QRS, and T axes; frontal QRS-T and spatial QRS-T angles, RR interval; PR interval; QRS duration; QT interval and corrected QT interval (QTc) calculated using the Bazett and Fridericia methods; peak amplitudes of P, Q, R, S and T waves; QRS integral; and T wave integral in all leads (I, II, III, aVL, aVF, aVR, V1, V2, V3, V4, V5, V6).
Machine learning models, training and testing
Selected ML models were used on standardized digitized values of 177 ECG variables. We compared supervised and semi-supervised ML models for the determination of age and gender. Assessment with supervised ML models included Support Vector Machines (SVM) with linear and Radial Basis Function (RBF) kernels, Adaptive Boosting (AdaBoost) with decision trees, and Linear Discriminant Analysis (LDA) models. For semi-supervised ML we used Triplets Bidirectional Generative Adversarial Networks (T-BiGAN) and Residual Networks (ResNet), a deep neural network.
Traditional ML models
Analysis with SVM is usually employed to solve complex classifications with a sensitive detection of outliers by defining boundaries among data points predetermined by certain supervised inputs. We used SVM in both the original data space with a linear kernel and in a new feature space obtained by a non-linear transformation of the data using RBF kernel. with penalty C = 0.5, 1, and 1.5 analyzed and optimal penalty C = 1.5 selected for age classification, and the default C = 1 for sex classification.
AdaBoost is a popular ensemble-based method for data classification that can enhance the power of a base/weak classifiers by a weighted linear combination of original data. We used AdaBoost with a decision tree model as the base estimator with hyperparameter depth of D = 1,3,5 tested, and learning rate L = 0.1,1,2 tested. The base estimator was set at 200 with the optimal hyperparameter combination of D = 5 and L = 1 for age classification, while for sex classification the base estimator was 50, D = 1, and L = 1.
LDA is a multi-class classification model that can be used for supervised learning by maximizing class separation on a low-dimensional space. We used LDA to separate multiple classes with multiple features based on data dimensionality reduction involving the entire ellipse of data and not only data on the boundary of distinct groups.
Age classification is a multi-class classification, and we used the entire dataset to develop the model. Model performance was evaluated by ratio of predicted and true labels for the determination of age-across the 0–21 years of the cohort, Sex classification is a binary determination. Since the difference in ECG variables is more pronounced among various ages than between the two sexes, we performed binary analysis to determine the sex of the subjects within each age-group. The performance of binary classification for SVM, AdaBoost and LDA was assessed using both the F1 score and receiver operating characteristic (ROC) curves as comparison metrics. We calculated ROC with the probability of each sample being assigned to one class. For model classification accuracy we used the F1-score metric, which combines precision and recall scores.
Semi-supervised ML models
T-BiGAN is a ML model that offers improved feature representation through semi-supervised learning, employing a model based on Bidirectional Generative Adversarial Networks (BiGAN). In this approach, semi-supervised data is seamlessly integrated into the training process via an additional triplet loss term. The BiGAN structure comprises an encoder and a decoder, facilitating data transformation into a latent space, alongside a discriminator tasked with distinguishing genuine data from synthetic data within the GAN framework. In T-BiGAN, auxiliary labels within the dataset are utilized. The choice of triplet loss is deliberated: during training, the model considers a probability where the distance from a query example to a negative example (i.e. those with labels different from the query) should be greater than the distance to positive examples. This strategic use of triplet loss fosters a mapping in the latent space that encourage data with the same label to form distinct clusters, differentiating them from data with other labels. This is the underlying rationale for the application of T-BiGAN on ECG data.
In our T-BiGAN model, we incorporated sex and age groups (2 sex-groups × 9 age-groups = 18 categories) as auxiliary labels during the training process. The model uses a latent dimension of 50 z_dim = 50), and is comprised of three main components: an encoder, a generator, and a discriminator. Each of these neural components consists of two hidden layers, with each layer having a size of 1024 units followed by a leaky Rectified Linear Unit (ReLU) activation layer with a negative slope of 0.2 for non-linearity. Additionally, the layers in the generator are followed by Batch Normalization layers. The optimizer is Adam with a very small initial learning rate of 1e-8 and β_1_ = 0.5, making the training stable but very slow to start. The model is regularized using L2 weight decay (2.5e-5) and weights are initialized with a small Gaussian noise (stddev = 0.02). Training is run for 501 epochs with a batch size of 256.
Residual Networks (ResNet) is a deep neural network architecture designed to facilitate the training of exceptionally deep networks. It achieves this by introducing residual blocks, which utilize skip connections to learn the difference (residual) between input and desired output in each block. ResNet architectures often incorporate batch normalization, global average pooling, and some in various depths.
The ResNet model comprises of an initial convolutional layer that applies 32 filters, batch normalization, ReLU activation, and max-pooling. The ResNet-based classifier is built on top of ImageNet-pretrained ResNet-50, using it as a feature extractor (with all layers frozen). The output of the ResNet backbone is passed through a custom fully connected head, consisting of dense layers of sizes 512, 256, 128, and 64, each followed by ReLU activation and 50% dropout to prevent overfitting. The final layer is a Softmax classifier that outputs class probabilities. The model is compiled with the Adam optimizer, using categorical cross-entropy loss and accuracy as a metric.
Similarly to the supervised ML models, T-BiGAN and ResNet models were used to characterize the sex of the subjects in a binary classification, while the age-group classification used a multi-class model for the determination of set age-groups.
Training and testing
For all supervised (SVM, AdaBoost, LDA) and semi-supervised (T-BiGAN, ResNet) ML models 75% of data was used for training, 5% for testing and hyperparameter tuning, and 15% for final classification. To minimize overfitting and report performance variance, we used k-fold cross-validation.
Statistical analysis
For binary classification, simple descriptive statistical measures were calculated (true positive, false positive, true negative, and false negative rates). From those rates, ROC curves were generated and Area Under the ROC Curve (AUROC) was calculated. For predictive accuracy, precision rates or positive predictive values (true positive divided by the sum of true and false positive), and recall or sensitivity (true positive divided by the sum of true positive and false negative) rates were calculated, next F1 scores were generated as the harmonic mean of the precision and recall rates, being one of the most accurate measures of test predictability. For multiple group classification confusion matrices were generated to assess true and predicted positive rates.
Results
Study population
After exclusion of patients with heart conditions, duplicate and erroneous ECGs, the final study cohort contained 29,408 curated normal ECGs across ages of 1 day to 21 years (12,318 male – 41.9%, 17,090 female – 58.1%). The cohort was divided based on prior ECG age classification following the developmental stages of children and young adults, to the following 9 age-groups: 1) term newborns: 1–6 days old; 2) neonates: 1–4 weeks old; 3) young infants: 1 months to < 6 months old; 4) older infants: 6 months to < 2 years old; 5) toddlers and small children: 2 to < 5 years old; 6) children: 5 to < 9 years old; 7) preteen children: 9 to < 13 years old; 8) teenagers: 13 to < 17 years old; 9), and adolescents to young adults: 17 to < 22 years old. The number of patients in each age group ranged from 304 to 7,366 (Table 1). Although we attempted to model age with a continuous regression analysis across the entire age range, but the confidence interval and error margin of ± 1.2 years was deemed to be too large and meaningless, when we had to compare 1–6 days old and 2–4 weeks old infants. Therefore, and following previous physiological classification of infants and children into distinct age groups, we performed our age-classification analysis using 9 distinct age groups.
Modeling of sex in various ages
Sex-related differences in ECG parameters were subtle and often masked by the more pronounced age-related changes. To control for the age-related differences, sex classification models were trained and tested separately within each age group. Predictive accuracy varied by age group and the ML model used. The summated area under the ROC curve in distinguishing male and female ECGs ranged from 61% in younger children to 96% in teenagers and young adults. Consistent with the AUROC scores, F1 scores for determining sex ranged from 0.53 to 0.91, depending on the age group and the ML model used. The best sex classification performance was achieved in teenagers (13–17 years) and young adults (18–21 years) with an AUROC pf 95% and an F1 score of 0.91, compared to AUROC of 65–82% and F1 scores of 0.53–0.7 in younger children (0–12 years) (Fig. 1, Table 2). Supervised ML models, such as SVM, consistently outperformed semi-supervised deep learning models, such as ResNet, in predicting sex along all age groups, e.g. an F1 score of 0.91 by SVM vs. 0.60 by ResNet, and an AUROC of 96% by SVM vs. 73% by ResNet in the 16–21 years old group (age group 9) (Fig. 2, Table 2).
Modeling of age from infancy to young adulthood
Numerous ECG variables showed variations among different age-groups in children and young adults. The following ECG features were identified having a higher importance using the permutation importance method: heart rate, PR interval, QRS duration, QTc interval, and R and T wave amplitudes in V1, V3 and V6 (Fig. 3). These key features were explicitly utilized in the supervised ML models to develop age-group prediction, while the semi-supervised T-BiGAN model processed all features without any discrimination or weight, and transformed to latent space to develop age-group classification. Visual representation of individual data points reflects how the accuracy of age prediction improved when the data was transformed to latent space (Fig. 4).
All models successfully discriminated among the predefined 9 age-groups in the multi-class classification model, with a true positive rate (TPR) ranging from 46–72%. The highest accuracy was observed in distinguishing the youngest age groups (1–6 days, 1–4 weeks, 1–5 months old) with TPRs of 64–72%, compared to older age groups (2–21 years), with TPRs of 46–62% (Fig. 5). Traditional supervised models performed better than semi-supervised neural networks. SVM with RBF kernel showed the highest accuracy with an average TPR of 60%, outperforming AdaBoost (49%), and LDA (55%). Younger age-groups with smaller number of subjects had a higher variation of results depending on hyperparameter optimization, reflected by wider confidence intervals, nevertheless, SVM outperformed the other models in multi-class classification despite hyperparameter optimization. Among semi-supervised models, T-BiGAN had the highest average TPR (57%) in multi-class classification of various ages compared to Resnet (39%).
A confusion matrix visually represents the true positive rates using SVM with RBF kernel (Fig. 5). The matrix revealed that misclassification (false negative rate: FNR) predominantly occurred in immediate neighboring age-groups, consistent with the expected overlap in physiological changes. Allowing a single age-group deviation (± 1 age-group error margin), increased the average adjusted age-group detection accuracy (TPR) to 94% for SVM (range 91–99%), and 92% with T-BiGAN (range 88–98%), and a FNR of 1–9% with SVM, and 2–12% with T-BiGAN.
Comparison of various machine learning models
Comparison of traditional supervised ML methods (SVM, AdaBoost, LDA) compared to semi-supervised neural networks(T-BiGAN, ResNet) demonstrated that when including less than 300 ECGs, supervised methods (SVM with linear or RBF kernel) outperformed semi-supervised methods in predicting both age and sex. When the analyzed data included 1000 or more ECGs, supervised and semi-supervised methods had similar accuracy. Overall, the best results were achieved using SVM with RBF kernel in both sex-prediction with a binary classification, and age-prediction using a multi-class classification.
Discussion
Our findings demonstrate that machine learning models can accurately classify both age and sex from ECG features in children and young adults. Notably, classification of age and sex was achieved with high precision even in groups containing only a few hundred ECGs – previously not demonstrated with any other method. Our results support the concept that age- and sex-related physiological differences are encoded in the ECG waveform and can be decoded through data-driven methods. Modeling demographic-specific normal ECGs using specific ML models may facilitate the development of more precise, automated ECG interpretation frameworks.
Age and sex classification
In early childhood, physiologic differences between males and females are minimal, but become more apparent around (10–12 years). Our results demonstrate that among adolescents and young adults, when males and females differ in physiologic features, their ECG also changes, reflected by subtle sex-related differences in specific parameters, such as PR interval, QRS duration, QTc interval, and R and S wave voltages in many leads. ML models detected these changes with high accuracy in adolescents and young adults, with AUROC values of 0.94–0.95. Such a high AUROC would serve as a remarkable metric for a screening tool, supporting the idea that the ECG encodes biologically relevant sex-specific signatures.
Similar to sex, age can be determined accurately by ECG in children and young adults. Somatic and physiologic changes occur during the development of children, with the most dramatic changes observed during early childhood (0–5 years), and less pronounced differences in adolescents and young adults (15 to 21 years). Following somatic growth, ECG variables change throughout childhood, with the most dramatic changes in early childhood, detected by specific ECG parameters, such as heart rate, PR, QRS and QTc intervals, and R and T wave voltages. Despite sample size limitations and class imbalance among analyzed groups, both supervised and semi-supervised ML models classified various ages with an excellent adjusted true positive rate of 88–99% by the ECG. This is the first ML-based multi-class model to classify nine distinct pediatric age groups using ECG data alone. The proof of the concept of multi-class classification using ML-enhanced ECG analysis is foundational in the process of developing an automated system for ECG analysis and defining normal ECGs for every age and sex.
Machine learning model comparison
Supervised ML models (SVM and AdaBoost) performed more favorably in prediction modeling of datasets with less than 1000 data points (ECGs) compared to semi-supervised neural networks (T-BiGAN and ResNet). Supervised and weighted preselection of ECG variables improved the prediction accuracy of supervised ML models. When a dataset (specific age group) contained more than 1000 data points (ECGs), the difference in performance between the supervised and semi-supervised models diminished. While previous ECG-based AI models relied on datasets in excess of 5,000 subjects, our study shows that effective classification and prediction is possible with much smaller subject numbers. Developing ML algorithms for ECG analysis that can model analyzed groups with less than a 1000 subjects, and distinguish these groups with remarkable accuracy is particularly relevant for rare cardiac disorders, where large datasets are not available.
Clinical significance of sex and age classification in youth
Our results highlight that ECG signatures differ by demographic group and that ML can reliably recognize these patterns. The most significantly affected ECG variables and ML modeling features were PR, QRS and QTc intervals and the R, S and T wave amplitudes. These very same ECG parameters are used to diagnose several heart conditions, including conduction defects, long QT syndrome (LQTS), and ventricular hypertrophy or enlargement associated with cardiomyopathies. The subtle changes in ECG variables of these heart conditions are not only affected, but could be easily masked by the changes caused by different age-groups and sexes. Without age- and sex-specific reference values, such abnormalities can be overlooked or misinterpreted. For example, a mildly prolonged QT interval may be normal in a 1-week-old female, but would serve as a suspected diagnosis in a 10-year-old male, and similarly a certain QRS duration and S wave amplitude in lead V2 could be normal in an 8-year-old female, but would be associated with significant ventricular enlargement or hypertrophy in a 2-year-old female.
Establishing robust normative ECG standards is crucial for future ML-based models aimed at detecting heart conditions in children. These models can only perform accurately if trained on well-defined demographic baselines with curated normal ECGs. By modeling healthy ECG profiles across pediatric and young adult age groups and sexes, we set the stage for ML tools that can provide demographic-specific diagnosis in clinical practice. It is important to emphasize that the primary aim of our study was not to predict age or sex as diagnostic endpoints, but rather to assess and model the representation of these factors in the ECG data. This distinction is important because accurate identification of age and sex signatures is a prerequisite for developing reliable diagnostic models that avoid confounding by demographic variability. In clinical practice, age and sex are known and recorded variables, but understanding their explicit ECG correlates enhances model transparency and interpretability, will serve as the foundation for future age-and sex-specific ML models for cardiac disease prediction, and provide an important step towards creating AI-enhanced ECG screening.
Limitations and strengths
Our study had certain limitations. Sex was self-reported, which may not always align with biologic sex – potentially affecting ECG patterns. Our ML analysis was limited to selected models, and excluded certain advanced AI methods, such as deep and convolutional neural networks, however, we believe that we have chosen representative models with appropriate optimization, and the exclusion of certain models was because the input signal was not deemed complex enough to warrant them.
Strengths of our study include the use of a curated dataset containing only healthy subjects, eliminating patients with cardiac conditions, and enabling the establishment of normal ECG values for accurate ML modeling. We also compared multiple ML algorithms, rather than relying on a single model, which strengthens confidence in our results and helps mitigate bias and overfitting. Achieving consistent findings across different methods suggests robustness and reproducibility of our results.
Conclusion
In conclusion, this study provides foundational evidence that ML can uncover age- and sex-specific signatures in pediatric ECG data. By establishing reliable age- and sex-specific ECG standards, this work supports future efforts to build ML models capable of identifying conditions with subtle ECG changes affected by age- and sex-specific variations. Our findings move the field beyond static reference standards toward dynamic, ML-informed models that better capture biological variability and will provide personalized, context-aware ECG interpretation. Such AI-enhanced ECG analytic models incorporating demographic variation are poised to improve the accuracy and reliability of ECG interpretation, particularly for rare cardiac conditions in children, where sample sizes are limited and demographic variability is large.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fisch C (2000) Centennial of the string galvanometer and the electrocardiogram. J Am Coll Cardiol 36:1737–1745. 10.1016/s 0735-1097(00)00976–111092639 · doi ↗ · pubmed ↗
- 2Bratincsák A, Kimata C, Limm-Chan BN, Vincent KP, Williams MR, Perry JC (2020) Electrocardiogram standards for children and young adults using Z-scores. Circ Arrhythm Electrophysiol 13:e 008253. 10.1161/CIRCEP.119.00825332634327 · doi ↗ · pubmed ↗
- 3Feeny A, Chung MK, Madabhushi A, Attia ZI, Cikes M, Firouznia M, (2019) Artificial intelligence and machine learning in arrhythmias and electrophysiology. Circ Arrhythm Electrophysiol 12:e 007952. 10.1161/CIRCEP.119.007952 · doi ↗
- 4Ribeiro AH, Ribeiro MH, Paixão GMM, Oliveira DM, Gomes PR, Canazart JA, (2020) Automatic diagnosis of the 12-lead ECG using a deep neural network. Nat Commun 11:1760. 10.1038/s 41467-020-15656-032273514 PMC 7145824 · doi ↗ · pubmed ↗
- 5Siontis KC, Attia ZI, Friedman PA, Noseworthy PA, Kapa S, Lopez-Jimenez F, (2021) Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat Rev Cardiol 18:349–360. 10.1038/s 41569-020-00503-233340010 PMC 8127952 · doi ↗ · pubmed ↗
- 6Attia ZI, Noseworthy PA, Lopez-Jimenez F, Asirvatham SJ, Deshmukh AJ, Gersh BJ, (2019) An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm. Lancet 394:861–867. 10.1016/S 0140-6736(19)31721-031378392 · doi ↗ · pubmed ↗
- 7Attia ZI, Kapa S, Lopez-Jimenez F, Mc Kie PM, Ladewig DJ, Satam G, (2019) Screening for cardiac contractile dysfunction using an artificial intelligence-enabled electrocardiogram. Nat Med 25:70–74. 10.1038/s 41591-018-0240-230617318 · doi ↗ · pubmed ↗
- 8Ko WY, Siontis KC, Attia ZI, Carter RE, Kapa S, Ommen SR, (2020) Detection of hypertrophic cardiomyopathy using a convolutional neural network-enabled electrocardiogram. J Am Coll Cardiol 75:722–733. 10.1016/j.jacc.2019.12.03032081280 · doi ↗ · pubmed ↗