Impact of attending neonatologist presence on neonatal intubation success and adverse events: a cohort study
Kate Hodgson, Clement Trinh, Kate Hodgson, Marnie Downes, Brett Manley, Marta Thio, Michael-Andrew Assad, Katharina Bibl, Shilpi Chabra, Cassandra DeMartino, Stephen DeMeo, Kristen Glass, Heidi Herrick, Bin Huey Quek, Sabine Iben, Philipp Jung, Jae Kim, Ayman Abou Mehrem

TL;DR
This study examines whether having an experienced neonatologist present affects the success of neonatal intubation and related complications.
Contribution
The study reveals that attending neonatologist presence is linked to lower first-attempt intubation success after adjusting for confounding factors.
Findings
Univariate analysis showed higher first-attempt success with attending presence.
Multivariate analysis found lower success odds with attending presence.
Attendings were present in 66% of intubations by junior operators.
Abstract
To evaluate the effect of attending neonatologist presence on first attempt neonatal intubation success and adverse events. Retrospective review of National Emergency Airway Registry for Neonates (NEAR4NEOS) intubations October 2014 - December 2022. Univariate and multivariate analyses were performed to estimate associations between attending presence and outcomes. Among 12,652 intubation encounters, attendings were present for 8,391 (66%) intubations by more junior operators. On univariate analysis, attending presence was associated with first attempt intubation success (OR 1.11, 95% CI 1.04–1.2). However, on multivariate analysis, attending presence was associated with lower first attempt success (aOR 0.78, 95% CI 0.70–0.86) and intubation requiring ≥ 3 intubation attempts (aOR 1.39, 95% CI 1.21–1.60). After adjustment, attending presence was associated with lower odds of first…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
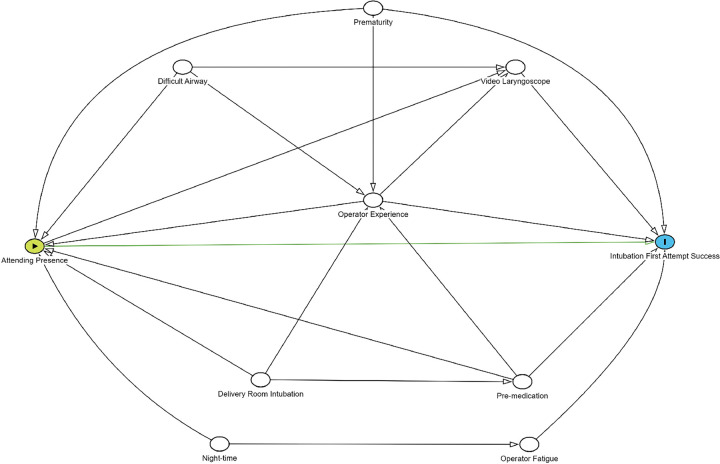 Figure 1
Figure 1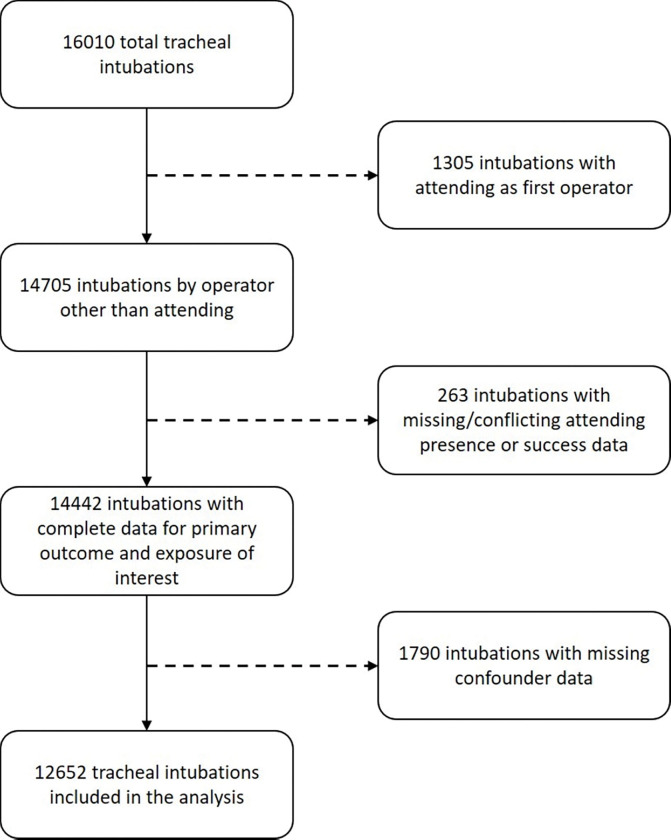 Figure 2
Figure 2- —National Health and Medical Research Council (NHMRC) Investigator
- —NHMRC Clinical Career Development Fellowship
- —NHMRC Leadership Level 1 Investigator
- —Victorian Government Operational Infrastructure Support Program (Melbourne, Australia)
- —Eunice Kennedy Shriver National Institute for Child Health and Development and Chiesi Inc, USA
- —NICHD
- —Arkansas Biosciences Institute, the National Center for Advancing Translational Sciences of the National Institutes of Health
- —New Scientist Development Award through the Arkansas Children’s Research Institute
- —Agency of Healthcare Research and Quality
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Neonatal Respiratory Health Research · Family and Patient Care in Intensive Care Units
INTRODUCTION
Neonatal endotracheal intubation is an important procedure required for the sickest infants. With advances in neonatal intensive care, fewer infants require intubation and therefore there are fewer opportunities for neonatal clinicians to gain proficiency (1). In adult emergency and critical care settings, first attempt endotracheal intubation success rates are approximately 80% (2, 3). In contrast, first attempt success rates for neonatal intubation are lower, around 50% overall. Experience of the operator (4, 5), premedication use (6, 7), nasal high flow therapy (8), and video laryngoscope use in inexperienced operators (9) are factors associated with increased success.
Severe desaturation and adverse events are common during neonatal intubation, and occur more often with repeated intubation events (10–12). The neonatal brain is particularly susceptible to physiological instability associated with attempts at intubation (13, 14). Thus, maximizing the chances of first attempt intubation success and maintaining patient stability during the procedure are of critical importance.
Greater operator experience increases first attempt intubation success and reduces adverse tracheal intubation associated events (TIAEs) (15, 16). Having an attending neonatologist present may provide immediate expertise, leadership, and oversight that could increase first attempt success and reduce adverse events. However, the impact of an attending neonatologist supervisor on these outcomes is unknown. The objectives of this study were to explore the factors associated with attending neonatologist presence at intubation, and to estimate the association between attending presence and first attempt intubation success and TIAEs. The hypothesis was that attending presence would be associated with an increased likelihood of first attempt intubation success, and a decreased likelihood of TIAEs.
METHODS
This study was a retrospective cohort study of prospectively collected data from 19 neonatal intensive care units (NICUs), across the USA, Canada, Australia, Germany and Austria, that contribute data to the National Emergency Airway Registry for Neonates (NEAR4NEOS), an international multicenter data registry of neonatal tracheal intubations. Each contributing site has individual approval or exemption to send data to the registry, and the Children’s Hospital of Philadelphia (CHOP) Institutional Review Board grants ethical approval for observational analyses of the database.
Data Collection
A standardized data collection form is used by each participating NICU to collect patient, provider, practice, and outcome data for all neonatal tracheal intubations. To maintain high levels of data integrity, every NICU developed and adhered to a specific compliance plan to ensure the accurate capture and entry of > 90% of intubations. Data from each site were entered into the secured, password-protected Research Electronic Data Capture (REDCap) system (17) hosted by the data coordinating center at CHOP.
Patient-related data captured included gestational age, age in days, and weight at birth and at the time of intubation, co-morbidities, premedication use, location of intubation, and indication for intubation. Provider-related data included the operator’s role and years of experience, and attending neonatologist presence at the intubation. Attending neonatologist is the term used for any practicing medical practitioner with specialist qualifications in neonatal critical care, and maybe referred to using different terms (for example, consultant) in different regions.
Practice data included the intubation device used, primary intubation or endotracheal tube exchange, and whether premedications were given. Outcome data included whether the intubation was successful, the number of attempts required, and whether there were any TIAEs. An attempt was defined as an airway maneuver that starts with the insertion of the device (i.e., laryngoscope) into the patient’s mouth and ends when the device is removed. First-attempt success was defined as successful intubation on the first attempt by the first airway provider. The NEAR4NEOS registry did not collect data regarding 24-hour on-site attending presence or the reasons for an attending being present at an intubation attempt.
Inclusion and Exclusion Criteria
All intubations that occurred between October 1st, 2014 and December 31st, 2022 were eligible for inclusion. Intubations where an attending was the initial intubation operator, were excluded from the analysis. Intubations that had conflicting or missing data for the primary outcome (first attempt success) or the exposure of interest (attending presence) were also excluded. Following the development of a Directed Acyclic Graph(18) to identify confounding variables to include in statistical modelling, intubations with missing data for these covariates were also excluded.
Study Outcomes
The primary outcome was first attempt intubation success, defined as successful intubation on the first attempt by the first operator.
The secondary outcomes were severe and non-severe tracheal intubation adverse events (TIAEs), as defined by previously published operational descriptions (4), severe oxygen desaturation (defined as ≥ 20% absolute decrease in peripheral oxygen saturation (SpO_2_) from the highest SpO_2_ documented immediately before the first intubation attempt), and multiple attempts (defined as ≥ 3 attempts, given the previously demonstrated increased risk of TIAEs and severe oxygen desaturation at this threshold) at intubation (12).
Non-severe TIAEs included esophageal intubation with immediate recognition, mainstem intubation, lip trauma, pain or agitation requiring additional sedation delaying intubation, epistaxis, emesis without aspiration, and dysrhythmia including bradycardia with heart rate < 60 beats per minute. Severe TIAEs included direct airway injury, esophageal intubation with delayed recognition (defined as placement of the endotracheal tube into the esophagus or hypopharynx with a lapse of time and clinical deterioration, such as severe desaturation, before the misplaced tube was removed), emesis with aspiration, laryngospasm, pneumothorax, gum or dental trauma, hypotension requiring intervention, need for cardiac compressions and cardiac arrest.
Directed Acyclic Graph (DAG) Formulation and Covariate Selection
A Directed Acyclic Graph (DAG) was developed to identify confounders of the hypothesized causal relationship between attending presence and first attempt intubation success (Fig. 1). A DAG represents known, theorized and assumed causal relationships between variables, including the exposure, outcome and confounders (18).
A minimally sufficient adjustment set was identified to establish the smallest set of variables that, when controlled for, adequately adjusted for confounding, thus allowing for an unbiased estimate of the causal effect of the exposure on the outcome (19, 20). The minimally sufficient adjustment set identified comprised the following confounders: prematurity (< 37 weeks’ gestation) (21), a known history of difficult airway (as identified by the operator prior to intubation) (10), operator experience (4, 22), pre-medication prior to intubation (7), use of video laryngoscopy (9), and night-time intubations (23). The operator’s years of experience was used as an indirect measure of neonatal intubation experience, as physician training level, measured in postgraduate years, has previously been demonstrated to be associated with first attempt intubation success (16). Video laryngoscope use has been demonstrated to be associated with higher rates of first attempt intubation success, particularly in inexperienced operators.
Statistical Analysis
Summary descriptive statistics were used to describe the patient demographics, using median and interquartile range (IQR) for continuous variables, and using frequencies and percentages for categorical variables. Associations between attending neonatologist presence and patient, provider, and practice characteristics were assessed using Chi-square tests for categorical variables and Kruskal-Wallis tests for continuous variables.
Univariate logistic regression modelling was performed to estimate the unadjusted association between attending presence and each individual primary and secondary outcome, with estimates presented as odds ratios (OR) with 95% confidence intervals (CI). Multivariable modelling using generalized estimating equations with covariate selection guided by the DAG and site clustering accounted for by use of an exchangeable correlation structure, was then performed to estimate the adjusted causal effect of attending presence on each outcome, presented as adjusted odds ratios (aORs) with 95% CIs. During the statistical analysis, it was found there was insufficient power to model the effect of consultant presence on individual TIAEs. The decision was made to present the results of multivariate modelling for composites of adverse outcomes, specifically any non-severe and any severe TIAEs, whilst providing descriptive statistics for individual events.
Correlation between intubations occurring within the same institution due to variations in institution practices or patient demographics was also accounted for in the statistical analysis.
Pre-specified subgroup analyses for the primary outcome were performed with the inclusion in the multivariable model of an interaction term between attending presence and pre-specified subgroups separately: level of experience of the operator (0–2 years, 3–5 years, > 6 years), gestational age (< 28 weeks’ completed gestation, > 28 weeks but < 34 weeks’ completed gestation, > 34 weeks’ completed gestation), known history of difficult airway, and location of intubation (delivery room or NICU). Statistical analysis was performed using R programming language (version 4.3.2) (24).
RESULTS
Of 16010 tracheal intubations during the study period, 12652 were included in the analysis (Fig. 2). A total of 1305 intubations where an attending was the operator were excluded. Of the 1790 intubations that were excluded for missing data for identified confounder variables, 1145 were intubations performed by respiratory therapists or ‘other’ operators for which there were no data for years of experience recorded.
Of the 12652 included intubations, 8391 (66.3%) had an attending present. Patient, provider and practice characteristic data are summarized in Table 1. Intubation encounters with an attending neonatologist supervisor present were more likely to involve infants who were of greater weight and age, and who had a known history of difficult airway. Intubations with an attending neonatologist present were also more likely to use a video laryngoscope and occur in the delivery room and during the day.
First Attempt Success and Number of Attempts
Univariate analysis found attending neonatologist presence was positively associated with first attempt intubation success (OR 1.11, 95% CI 1.04 to 1.20). However, on multivariate analysis, when controlling for the confounders of prematurity, known history of difficult airway, operator experience, premedication and night-time intubations, attending presence was found to be negatively associated with first attempt intubation success (adjusted OR (aOR) 0.78, 95% CI 0.70 to 0.86).
Subgroup analysis (Table 2) found attending presence was consistently associated with decreased odds of first attempt success across all levels of operator experience; the strength of the association was greatest for operators with the most experience (aOR 0.67, 95% CI 0.50 to 0.91). Similarly, stratified analyses by gestational age, neonates with known history difficult airways, and location of intubation also consistently demonstrated a negative association between attending presence and first attempt success.
Multivariate analysis found attending presence was associated with increased odds of intubation requiring three or more attempts compared to successful intubation within two attempts (aOR 1.37, 95% CI 1.21 to 1.60).
Tracheal Intubation Associated Events (TIAEs) and Severe Desaturation
On multivariate analysis, attending presence was associated with increased odds of severe oxygen desaturation (aOR 1.12, 95% CI 1.02 to 1.24).
Due to the low incidence of many of the reported TIAEs in the study cohort, there was insufficient precision to provide meaningful effect estimates of attending presence on individual TIAEs. The incidence of these data has been presented in Table 3. When these individual events were aggregated into composite outcomes, multivariate analysis found attending presence to be associated with increased odds of both non-severe (aOR 1.29, 95% CI 1.09 to 1.52) and severe TIAEs (aOR 1.69 95% CI 1.16 to 2.47).
DISCUSSION
This multicenter retrospective observational study is the first to examine the association between attending neonatologist presence and first attempt intubation success rates and TIAEs in neonates. Attending neonatologist presence during endotracheal intubation was more likely for infants who were larger, older, had a known history of difficult airway, and those intubations that occurred in the delivery room, during the day and with video laryngoscopy. However, these associations were only demonstrated on bivariate analysis without consideration of potential confounders or the strength of these associations, and should be interpreted with caution.
On univariate analysis attending presence was associated with increased likelihood of first attempt intubation success. However, in contrast to our hypothesis, after adjusting for potential confounders attending neonatologist presence was associated with lower first attempt intubation success overall. This association remained across all operator experience and gestational age subgroups. The study also demonstrated an association between attending presence and more episodes of severe desaturation during intubation, non-severe and severe TIAEs (when individual adverse events were aggregated into composite outcomes), as well as a higher number of intubation attempts.
There are several potential explanations for our findings. It is likely there were unmeasured confounders which were not adjusted for, meaning that there was greater illness severity for the group where an attending neonatologist was present, and subsequently lower likelihood of first attempt intubation success as well as greater risk of adverse events. These data suggest that clinical teams may already be risk stratifying to ensure an attending is present at intubations anticipated to be more challenging or risky in their NICU. This is supported by a survey of NEAR4NEOS sites conducted following the present study that found NICUs typically have attendings present for intubations involving infants that are extremely premature, have a known difficult airway, have underlying congenital anomalies conferring a greater risk of clinical instability during intubation (for example congenital heart disease or congenital diaphragmatic hernia) and emergent intubations. Some units reported having guidelines or protocols for attending presence at neonatal intubation.
In addition, with senior presence to escalate subsequent intubation attempts, there may be a greater tolerance for patient instability such as severe oxygen desaturation and multiple intubation attempts, or attendings may terminate intubation attempts earlier leading to lack of success. The psychological effects of an attending on junior and supporting staff are intangible and may increase performance anxiety and operator stress leading to lower first attempt success. The reasons for an attending being present are not collected in the registry, nor the timepoint at which the attending neonatologist was present during the intubation. We would recommend that these parameters are collected in the future.
Inexperienced operators have been demonstrated to have the lowest rates of first attempt intubation success, as low as 23%, while also having higher rates of TIAEs (4, 16). TIAEs are relatively common in neonates owing to their airway anatomy and relatively minimal physiological reserve (11, 15). The results of our study suggest that attending neonatologists were likely appropriately present for anticipated high risk intubations. However, attending neonatologist supervision may not mitigate the risks associated with neonatal intubation.
Attending neonatologist coverage across NICUs varies significantly, as does individual attending coaching skill. Research examining the impacts of increased attending coverage on clinical outcomes is also varied in its findings (25–27). This study does not delineate the specific aspects of attending presence that contribute to the observed decrease in first attempt success. Future studies are warranted to explore these dynamics in greater detail. It may be that the presence of an attending neonatologist alone is insufficient to influence first attempt intubation success, but instead should facilitate a strategy of matching the operator to the intubation and adjuncts that may increase the chance of success such as video laryngoscopy, premedications and potentially nasal high flow use.
A strength of this study was the use of a DAG for identification of confounders to include as covariates in our statistical modelling. In observational studies exploring casual effects, unnecessarily adjusting for confounders or variables that are not true confounders, can introduce bias leading to erroneous effect estimates (18–20). The use of a DAG in our study reduces the risk of such bias.
This study has a number of limitations. The observational nature of the study makes it susceptible to unmeasured confounders not identified by the DAG, introducing the risk of bias to causal effect estimates. As data were not collected on changes in practice that may have occurred during the study period, these practice changes could not be accounted for. Attending presence may have altered the completeness of data and led to a selection bias. Years of experience is likely an imprecise measure of neonatal intubation experience, as it does not take into account factors such as variability in terms of numbers of intubations performed, recency of experience, or institutional and regional differences leading to differences in exposure to neonatal intubations. Intubations were excluded if they were missing data for confounding variables, potentially introducing a degree of selection bias.
The modelling of the relationship between attending presence and composite adverse outcomes combined events of heterogeneous significance. This may make the interpretation of the clinical significance of these associations challenging, and thus should be interpreted with caution.
Further research may help to delineate the most effective strategies for supporting intubations where an attending neonatologist is supervising, to optimise coaching, team performance and subsequent procedural success.
CONCLUSION
After adjustment for potential confounders and site clustering, attending presence was associated with a lower likelihood of first attempt intubation success, and increased odds of ≥ 3 intubation attempts and severe desaturation. These results suggest that attending neonatologists may appropriately be more often present in anticipated high-risk intubations, yet alternative strategies to improve intubation success and proficiency of trainees may be more important than attending presence alone. Furthermore, there may be unmeasured confounders that have not been accounted for as a source of bias. Further research is needed to examine operator-related factors that impact intubation success.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Downes KJ, Narendran V, Meinzen-Derr J, Mc Clanahan S, Akinbi HT. The lost art of intubation: assessing opportunities for residents to perform neonatal intubation. J Perinatol. 2012;32(12):927–32.22382858 10.1038/jp.2012.17 · doi ↗ · pubmed ↗
- 2Russotto V, Myatra SN, Laffey JG, Tassistro E, Antolini L, Bauer P, Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA. 2021;325(12):1164–72.33755076 10.1001/jama.2021.1727 PMC 7988368 · doi ↗ · pubmed ↗
- 3Bernhard M, Becker TK, Gries A, Knapp J, Wenzel V. The First Shot Is Often the Best Shot: First-Pass Intubation Success in Emergency Airway Management. Anesth Analg. 2015;121(5):1389–93.26484464 10.1213/ANE.0000000000000891 · doi ↗ · pubmed ↗
- 4Foglia EE, Ades A, Sawyer T, Glass KM, Singh N, Jung P, Neonatal Intubation Practice and Outcomes: An International Registry Study. Pediatrics. 2019;143.
- 5Chen DY, Devsam B, Sett A, Perkins EJ, Johnson MD, Tingay DG. Factors that determine first intubation attempt success in high-risk neonates. Pediatr Res. 2024;95(3):729–35.37777605 10.1038/s 41390-023-02831-8PMC 10899101 · doi ↗ · pubmed ↗
- 6Krick J, Gray M, Umoren R, Lee G, Sawyer T. Premedication with paralysis improves intubation success and decreases adverse events in very low birth weight infants: a prospective cohort study. J Perinatol. 2018;38(6):681–6.29467520 10.1038/s 41372-018-0082-2 · doi ↗ · pubmed ↗
- 7Le CN, Garey DM, Leone TA, Goodmar JK, Rich W, Finer NN. Impact of premedication on neonatal intubations by pediatric and neonatal trainees. J Perinatol. 2014;34(6):458–60.24577435 10.1038/jp.2014.32 · doi ↗ · pubmed ↗
- 8Hodgson KA, Owen LS, Kamlin COF, Roberts CT, Newman SE, Francis KL, Nasal High-Flow Therapy during Neonatal Endotracheal Intubation. N Engl J Med. 2022;386(17):1627–37.35476651 10.1056/NEJ Moa 2116735 · doi ↗ · pubmed ↗