A Preliminary Investigation of Brain Cannabinoid Receptor Type 1 (CB1R) Availability in Men with Opioid Use Disorder
ANAHITA BASSIR NIA, Ardavan Mohammad Aghaei, Jeremy Weleff, Julia Shi, Angelina Contreras, Mackenzie Griffin, Oluwole Jegede, Brian Pittman, Ilan Harpaz-Rotem, Ansel Hillmer, Deepak D’Souza

TL;DR
This study found that men with opioid use disorder have lower brain CB1R availability compared to healthy controls, suggesting a potential role for the endocannabinoid system in treatment.
Contribution
The study is the first to report reduced CB1R availability in men with opioid use disorder using high-resolution imaging.
Findings
CB1R availability was 15% lower in OUD subjects compared to healthy controls (p = 0.04).
Lower CB1R availability was observed in several corticolimbic brain regions in OUD subjects.
No associations were found between CB1R availability and treatment type, stress, or medication use in OUD subjects.
Abstract
The endocannabinoid (eCB) system has been proposed as a potential target for developing new medications for opioid use disorder (OUD). However, the status of the eCB system, specifically brain cannabinoid receptor type 1 (CB1R) in OUD, is unknown. In this study, CB1R availability was measured in males with OUD on stable opioid agonist treatment (OAT) (n = 10) versus healthy controls (HC) (n = 18), using High-Resolution Research Tomography (HRRT) and the CB1R-specific radiotracer, [11C]OMAR. The average volume of distribution (VT) across 13 regions was compared between the OUD and HC groups. Average VT was 15% lower in OUD vs. HC subjects (p = 0.04). Lower VT in OUD compared to HC was also observed in several corticolimbic areas. Within OUD no effects on CB1R availability were observed for treatment medication (methadone vs. buprenorphine), current stress levels, or antidepressant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
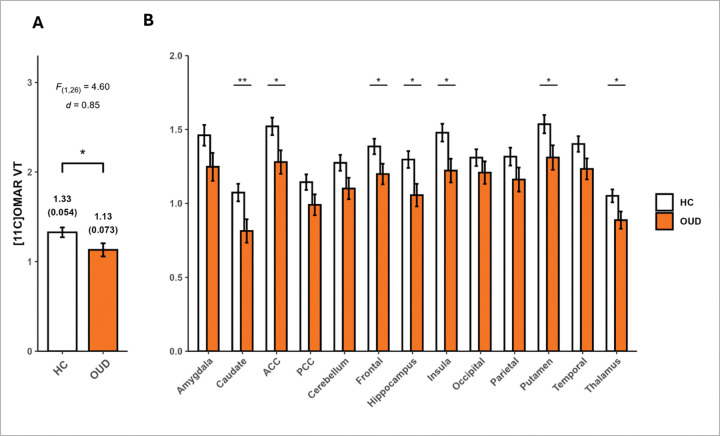 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCannabis and Cannabinoid Research · Neurotransmitter Receptor Influence on Behavior · Forensic Toxicology and Drug Analysis
Introduction
An alarmingly high number of Americans continue to die from opioid overdose every day in the United States (1, 2). The National Survey on Drug Use and Health (NSDUH) reported that 9.9 million people misused opioids in 2018 in the US, and more than 117,000 individuals started using high-potency opioids for the first time (3). Despite widespread preventive and therapeutic efforts, the rates of drug overdose have increased fourfold over the past two decades, with opioids being involved in more than 68% of them (3). The current state-of-the-art treatment for opioid use disorder (OUD) primarily involves modulation of the opioid receptor system through Opioid Agonist Treatment (OAT) with medications such as methadone and buprenorphine, or opioid antagonist treatment with naltrexone (4, 5). However, OAT faces challenges with high rates of opioid relapse and treatment discontinuation among patients (6–10). More than 50% of individuals enrolled in these programs continue to use illicit opioids despite being in treatment, making effective OUD treatment challenging (11–13). There is a need to look for novel approaches that target systems beyond the existing FDA-approved opioid receptor-modulating medications for OUD. Increasing evidence suggests that the endocannabinoid (eCB) system could be a promising target (14–18).
The eCB system closely interacts with the endogenous opioid (opioidergic) system. Cannabinoid Receptor Type 1 (CB1R) and Mu Opioid Receptors (MOR) are both Gi/o-coupled receptors and are colocalized in several brain areas implicated in the pathophysiology of OUD (19–24). Furthermore, the eCB and opioidergic systems share similar functions in regulating stress and pain, and their agonistic activation yields similar results, including antinociception, sedation, hypotension, motor depression, and drug reward and reinforcement (25–27). Consequently, there is growing interest in exploring the role of the eCB system in OUD treatment (28, 29).
Preclinical studies have shown region-specific reductions in CB1R density, G-protein binding capacity, or mRNA levels in the cerebral cortex (30), hippocampus (31, 32), basolateral amygdala (32), and cerebellum (32), although not in all regions (32, 33). In addition, chronic morphine exposure in these preclinical models was associated with higher mRNA levels of Fatty-acid Amide Hydrolase (FAAH) and Monoacylglycerol Lipase (MAGL) (31), the two main eCB degrading enzymes, and lower levels of the principal endocannabinoid 2-Arachidonoylglycerol (2-AG) in several brain areas (34, 35). Consistent with preclinical findings, a recent PET imaging study using the FAAH-specific ligand showed that individuals with OUD have higher whole-brain FAAH levels (36). However, the status of CB1R in individuals with OUD has not yet been investigated.
The availability of reliable CB1R-specific radiotracers makes it possible to measure CB1R availability in vivo in humans. [^11^C]OMAR, a CB1R antagonist, has been successfully and reliably used in numerous studies to investigate CB1R availability in humans (37–42). The goal of this study was to measure CB1R in vivo in men with OUD on OAT, using [^11^C]OMAR tracer.
Subjects and Methods
Approvals:
This study was approved by the Yale University Institutional Review Board, the Yale Magnetic Resonance Research Center, and the Yale New Haven Hospital Radiation Drug Research Committee. All participants received detailed explanations, and written informed consent was obtained from each subject.
Subjects:
Males with a diagnosis of OUD who were not using cannabis or other drugs were recruited. Participants were interviewed using the Structured Clinical Interview for DSM-5 (SCID-5), and individuals with concurrent major psychiatric disorders were excluded. Subjects were required to be under OAT with a stable dose of methadone or buprenorphine for at least one month, which was confirmed by contacting their OAT treatment centers or providers. Participants were excluded if they reported past-month use of any substances, including cannabis, and if they had a positive urine toxicology for any substance, except prescribed methadone or buprenorphine. Consistent with definitions from the Centers for Disease Control and Prevention and other studies, individuals who reported risky alcohol use (i.e., alcohol use exceeding 14 standard drinks per week) or heavy nicotine use (i.e., nicotine or tobacco use equivalent to one or more packs of cigarettes per day (PPD)) were excluded (43–45). Other exclusion criteria included claustrophobia, ferromagnetic metal in the body, a heart pacemaker, abnormal coagulation tests, and poor arterial access. To mitigate the potential effects of acute opioid intoxication and withdrawal, all PET scans were scheduled between 9 and 11 a.m., and participants were instructed to take their daily OAT dose only after completing the PET scan. Opioid craving and withdrawal symptoms were measured in the morning before the PET scan, and the PET scan was rescheduled if they had moderate or severe withdrawal symptoms. Male healthy controls (HC) with no psychiatric diagnosis based on SCID-5 and no substance use disorder (except nicotine) served as the comparison group.
Measurements:
Nicotine dependence was assessed using the Fagerström Test for Nicotine Dependence (FTND), and perceived stress was evaluated using the Perceived Stress Scale (PSS). Opioid withdrawal symptoms were measured using the Clinical Opiate Withdrawal Scale (COWS) (cutoff score for moderate withdrawal symptoms > 7), and the intensity of opioid craving was measured using a Visual Analogue Scale (VAS), ranging from 0 to 100 (cutoff score for moderate craving > 30). The time since the last illicit opioid and cannabis use was recorded using the Drug History Questionnaire (DHQ), and the duration current OAT episode and current OAT dose was collected by the Methadone Questionnaire (MQ).
Imaging:
MR Imaging:
Structural magnetic resonance imaging (3D MPRAGE) was conducted for participants using a Siemens 3-T Trio system (Siemens Medical Solutions, Malvern, Pennsylvania) with a circularly polarized head coil to exclude individuals with gross anatomical abnormalities and anatomically delineate regions of interest for PET analyses. The dimensions and voxel size of MR images were 256 × 256 × 176 and 0.98 × 0.98 × 1.0 mm3, respectively.
PET Imaging:
CB1R availability was measured using [^11^C]OMAR (46). PET data were acquired using a High-Resolution Research Tomograph (HRRT). Before PET scanning, two IV lines and an arterial catheter were placed. [^11^C]OMAR was prepared with high molar activity by previously described methods adapted to the TRACERlab FXC Pro automated synthesis module (GE Healthcare, Milwaukee, WI) (46). Image acquisition begun with a 6-minute transmission scan acquired for attenuation correction. Emission data acquisition was started with a bolus injection of up to 740 MBq [^11^C]OMAR and continued for at least 120 minutes. The head motion was continually tracked during the acquisition of PET data with a Vicra marker-based tracking system (NDI Systems, Waterloo, Ontario). Since no reference region existed for [^11^C]OMAR, arterial blood samples were collected contralaterally from the radiotracer administration arm during the PET scan to measure the plasma input function and High-Performance Liquid Chromatography (HPLC) analysis of radioactive metabolites. Radioactivity in plasma was measured with a gamma counter. The column-switching HPLC analysis method was used to assess radioactive metabolites and unchanged parent compounds (47). The measured input function was the product of the radioactivity concentration in plasma and the unchanged parent fraction.
Image Processing and Analysis:
To ensure blind data processing and analysis, a pseudo-randomized subject identifier devoid of diagnostic and demographic information was created and assigned to each participant upon uploading data into our database. Image analysts only saw this subject identifier during pre-processing and analyses. List mode data was reconstructed using MOLAR (48), with attenuation, normalization, and motion corrections. Early PET image data were registered to the subject’s T1-weighted MR image. The T1-weighted MR image was non-linearly registered to MNI space for the region of interest (ROI) identification using the Anatomical Automatic Labeling (AAL) atlas (49). Predetermined ROIs included the following thirteen regions: amygdala, caudate, cerebellum, anterior cingulate (AC), posterior cingulate (PC), frontal, hippocampus, insula, occipital cortex, parietal cortex, putamen, temporal, and thalamus. The nucleus accumbens and ventral tegmental area were not included due to challenges in imaging with the [^11^C]OMAR radiotracer given their small size, anatomical location, and the tracer’s characteristics. Since OUD is associated with significantly lower gray matter volumes (50–52), this was accounted for with partial volume correction (53), as previously implemented (54, 55). [^11^C]OMAR VT was estimated using the metabolite-corrected arterial plasma input function with multilinear 1 analysis (MA1; t*=30 min) (56), which has good test-retest reproducibility with mean absolute deviations of 7.3–10.0%.
Statistical Analysis:
All data were summarized descriptively, and normality was assessed using normal probability plots and Kolmogorov–Smirnov test statistics. Consistent with prior PET imaging studies employing the [^11C]OMAR radiotracer in psychiatric populations (41, 42, 57), the primary outcome was defined as the average CB1R availability, calculated as the mean value across regions of interest. The primary effect of interest was the main effect of group, testing for overall differences in CB1R availability between groups.
For the primary analysis, composite VT levels were compared between healthy controls (HC) and individuals with opioid use disorder (OUD) using independent, two-sided t-tests. Given the small sample size, additional exploratory analyses were performed to examine region-specific differences in binding between groups using independent t-tests. For these analyses, both unadjusted and false discovery rate (FDR)–corrected p-values are reported.
Further exploratory analyses employed linear mixed models (LMMs) to evaluate the main and interaction effects of potential covariates within the OUD group, including OAT medication, antidepressant use, FTND, and PSS scores. All analyses were conducted using SAS software, version 9.4 (SAS Institute Inc., Cary, NC).
Results
A total of 10 male individuals with OUD and 18 male HC participants were studied (Table 1). No significant differences were found in sociodemographic characteristics. On the scan day, craving (4.0 ± 9.7 [SD]) and withdrawal (0.8 ± 1.5) scores were low among participants with OUD. As per the inclusion criteria, participants did not have concurrent active major psychiatric or substance use disorders. One subject had current symptoms of depression due to chronic dysthymia. Subjects with OUD reported more nicotine use (Table 1) and treatment with antidepressant medications for a history of depression and other psychiatric disorders (supplemental Table 1).
CB1R availability in individuals with OUD compared to HC.
Lower global (composite across regions) CB1R availability was observed in participants with OUD compared to HC (group effect: F(1,26) = 4.6, p= 0.04, difference = −14.7%, d= 0.85) (Figure 1a). The exploratory analyses showed a significant group-by-region interaction (F(12,312)= 2.42, p= 0.005), where group differences were observed in some but not all regions. Specifically, group effects were observed in several corticolimbic areas, including AC (−15.87%, F(1,312)= 5.91, p= 0.016, d=0.96), caudate (−24.21%, F(1,312)= 6.85, p= 0.009, d=1.03), frontal (−13.49%, F(1,312)= 4.60, p= 0.033, d=0.84), hippocampus (−18.57%, F(1,312)= 6.34, p= 0.012, d=0.99), insula (−17.34%, F(1,312)= 6.56, p= 0.011, d=1.01), putamen (−14.71%, F(1,312)= 4.76, p= 0.030, d=0.86), and thalamus (−15.63%, F(1,312)= 5.06, p= 0.025, d=0.89) (Table 2 and Figure 1b). In addition to these group differences, there was a highly significant group by region interaction, which was substantially driven by a greater overall region effect within HC (F_(12,312)= 71.7, p<.0001), compared to OUD (F(12, 312)_= 39.5, p<.0001). That is, although both effects are highly significant, the F-statistic for HC is >80% higher than that for OUD. Pair-wise comparisons between regions within each group are not of primary interest and thus not reported. Supplementary Table S2 summarizes the result of a similar LMM model with age added as a covariate.
Exploratory analysis of the impact of potential covariates on CB1R availability in OUD.
• Methadone vs. buprenorphine treatment:
There were no significant differences (F(1,8) = 0.52, p = 0.49) in overall CB1R availability between those receiving methadone (n = 7; mean dose: 80.7, SD: 32.2 mg) and those receiving buprenorphine (n = 3; mean dose: 22.7, SD: 3.2 mg) (Table S3). No associations were observed between OAT dose and CB1R availability.
• Current stress level:
No significant associations existed between current stress levels in the OUD group, as measured using PSS, and CB1R availability (Spearman’s r= 0.07, p=0.84).
• Nicotine use:
Among individuals with any nicotine use (n=6), no associations were observed between FTND scores and CB1R availability (Spearman’s r=0.09, p=0.87).
• Antidepressant medications:
Among individuals with OUD, there were no significant differences in overall CB1R availability between those taking (1.11 ± 0.042) and those not taking (1.19 ± 0.064) antidepressant medication (F(1,8) = 1.23, p = 0.30) (Table S4).
Discussion
To our knowledge, this is the first study to measure CB1R availability in individuals with OUD in vivo. Males with OUD (on stable OAT) showed 15% lower global CB1R availability compared to healthy male individuals. This finding aligns with several (30–32), but not all (32, 33), animal studies showing lower CB1R density or mRNA levels in several brain regions.
The findings of lower CB1R availability are intriguing in light of higher FAAH levels reported in individuals with OUD (36). Higher FAAH activity is associated with lower AEA levels (57). The lower CB1R availability observed in our study, combined with high FAAH activity in individuals with OUD reported elsewhere (36), suggests a lower eCB tone in males with OUD.
There is substantial evidence of extensive overlap between the eCB and opioid systems that may explain why exposure to opioids could lead to lower CB1R levels. When administered acutely, cannabinoids and CB1R agonists increase endogenous opioid release (endorphin and enkephalin) (58, 59), and MOR expression (60, 61). Similarly, acute administration of opioids alters eCB levels (62, 63), and CB1R expression (61, 64, 65), and functionality (61). Moreover, the colocalization of CB1R and MOR in several brain areas is the basis of functional interactions (19, 20). Increasing evidence suggests that there is bidirectional modulation of the rewarding and reinforcing properties of opioids and cannabinoids (22). Preclinical studies of chronic opioid exposure have shown region-specific reductions in CB1R density, G-protein binding capacity, or mRNA levels in the cerebral cortex (30), hippocampus (31, 32), basolateral amygdala (32), and cerebellum (32), in addition to higher levels of FAAH and MAGL mRNA (31), and lower levels of 2-AG in several brain regions (34, 35).
The low CB1R availability in individuals with OUD suggests that the eCB system could potentially serve as a new target in OUD treatment (27, 66–68). Preclinical studies demonstrated that eCB modulation reduces the reinforcing effects of opioids (15, 69), opioid-seeking behaviors (70, 71), and opioid withdrawal symptoms (72). Similarly, human studies reported that targeting the eCB system is effective in attenuating opioid craving (73). Moreover, positive effects of cannabinoids or eCB modulators in the treatment of OUD comorbidities such as chronic pain have been reported (74–81). Some but not all observational studies suggest that cannabinoids may have opioid-sparing effects (82), while experimental studies suggest mixed results (83). Although research on the effects of cannabis or its principal active constituent, delta-9-tetrahydrocannabinol (THC), on OUD treatment remains inconclusive (84), new investigational eCB modulators, such as FAAH and MAGlipase inhibitors, are now available to target the eCB system (85). Current evidence shows promising therapeutic effects of FAAH inhibitors in nicotine and cannabis dependence (86, 87). A significant advantage of these compounds is their ability to modulate the eCB function regionally, causing minimal, if any, CB1R downregulation that is typically induced by direct CB1R agonists such as THC (41). Moreover, FAAH inhibitors have low abuse liability, which is a significant benefit compared to cannabis or THC (88). Further studies are required to investigate the potential therapeutic effects of eCB modulators in treating OUD.
The involvement of the eCB system in stress regulation and reward processing has been extensively reported (18, 89–94). Moreover, low CB1R availability was reported in other substance use disorders, including cannabis use disorder (41), alcohol use disorder (95), and tobacco use disorder (96). It remains unclear whether this reduced CB1R availability is drug-specific or reflects broader deficits in reward processing and heightened stress reactivity in addiction, regardless of substance type. Further investigations are also required to determine if lower CB1R in individuals with OUD precedes the development of OUD, or is a consequence of long-term opioid use, and to investigate other factors potentially involved in these alterations. Future research should consider comparing the CB1R availability in individuals with OUD who are not on OAT to assess if similar low CB1R availability exists in individuals with OUD regardless of OAT. Moreover, measuring CB1R availability before and after opioid abstinence periods would illuminate the impact of active opioid use on CB1R. Furthermore, assessing CB1R availability in individuals prescribed opioids without OUD could differentiate the general effects of opioid use on CB1R from those specifically associated with OUD.
This study has certain limitations that should be considered when interpreting the results. Only male participants with OUD were recruited in this study. Existing literature indicates sex differences in the eCB system both at baseline and in the context of other psychiatric disorders (97–106). Thus, future studies should explore the eCB status in females to better understand these potential sex differences. The limited sample size reduces overall statistical power, and specifically limits estimating potential covariate effects– future studies with larger samples and a comparable number of participants receiving methadone or buprenorphine treatment are necessary to replicate these preliminary findings. While there were no significant group differences in age, the OUD group was older, with a few participants over 65. Additionally, our sample was unbalanced regarding nicotine dependence. A larger study with a balanced age and nicotine dependence distribution is necessary to parse out the effect of opioid exposure from potential confounders. Furthermore, only OUD participants who were stable on OAT were included to minimize the effects of opioid withdrawal and intoxication on CB1R availability. Further research is necessary to determine if individuals with OUD who are not receiving OAT exhibit similar low CB1R availability. Lastly, our study excluded individuals using other substances, including cannabis. This decision was critical for the interpretability of the data, given strong evidence that cannabis use is associated with lower availability of CB1R (41). However, excluding other substance use may limit the generalizability of our results to the broader population of OUD individuals with co-occurring use of other substances. Future studies should consider including individuals with OUD and concurrent substance use disorders to enhance the generalizability of the findings.
In summary, our results provide preliminary evidence of lower global CB1R availability (composite across regions) in males with OUD in OAT treatment. Future studies are required to determine the clinical implications of low CB1R in males with OUD, and the possibility of targeting the eCB system in treating OUD.
Supplementary Material
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wide-ranging online data for epidemiologic research (WONDER). Atlanta GC, National Center for Health Statistics; 2017. Available at http://wonder.cdc.gov.
- 2National Center for Health Statistics (2025): U.S. Overdose Deaths Decrease in 2023, First Time Since 2018. National Center for Health Statistics,.
- 3U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (2020): National Survey on Drug Use and Health 2019 (NSDUH-2019-DS 0001).
- 4Kampman K, Jarvis M (2015): American Society of Addiction Medicine (ASAM) National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. J Addict Med. 9:358–367.26406300 10.1097/ADM.0000000000000166 PMC 4605275 · doi ↗ · pubmed ↗
- 5The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update. J Addict Med. 14:1–91.
- 6Nosyk B, Marsh DC, Sun H, Schechter MT, Anis AH (2010): Trends in methadone maintenance treatment participation, retention, and compliance to dosing guidelines in British Columbia, Canada: 1996–2006. J Subst Abuse Treat. 39:22–31.20418051 10.1016/j.jsat.2010.03.008 · doi ↗ · pubmed ↗
- 7Lo A, Kerr T, Hayashi K, Milloy MJ, Nosova E, Liu Y, (2018): Factors associated with methadone maintenance therapy discontinuation among people who inject drugs. J Subst Abuse Treat. 94:41–46.30243416 10.1016/j.jsat.2018.08.009PMC 6375706 · doi ↗ · pubmed ↗
- 8Hser YI, Saxon AJ, Huang D, Hasson A, Thomas C, Hillhouse M, (2014): Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial. Addiction. 109:79–87.23961726 10.1111/add.12333 PMC 3947022 · doi ↗ · pubmed ↗