The Indian regulatory framework and the surge of unproven stem cell therapies—a call for diagnosis
Vaishnav M

TL;DR
This paper examines India's regulatory issues regarding unproven stem cell therapies and suggests reforms to protect patients and promote scientific progress.
Contribution
The paper provides a critical analysis of India's stem cell regulatory framework and proposes actionable reforms to address the rise of unproven therapies.
Findings
India's stem cell regulatory framework suffers from ambiguous laws and poor implementation.
The lack of regulation has led to India becoming a hub for unproven stem cell tourism.
Proposed reforms include better funding, consolidated clinical regulation, and public engagement.
Abstract
Stem cell science lies at the heart of regenerative medicine; it is believed to have the potential to address several otherwise incurable diseases. However, even though stem cell interventions are at the experimental stage, they are advertised as a panacea for various human maladies. India, like other jurisdictions across the globe, has witnessed the mushrooming of ‘experts’ and ‘clinics’ selling (unproven) stem cell therapies to vulnerable and desperate patients. The unscrupulous activities in the stem cell industry endanger patients and hinder legitimate scientific progress. In light of the crisis of unproven stem cell therapies, I seek to comprehensively study the Indian regulatory framework on stem cells. The article identifies multiple issues in the framework—the inherent ambiguity in the governing laws, the unscientific functioning of the regulatory institutions, the poor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
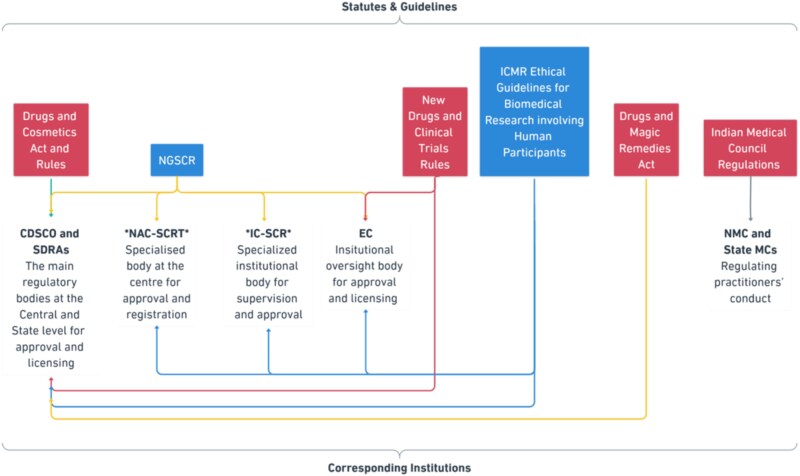 Figure 1
Figure 1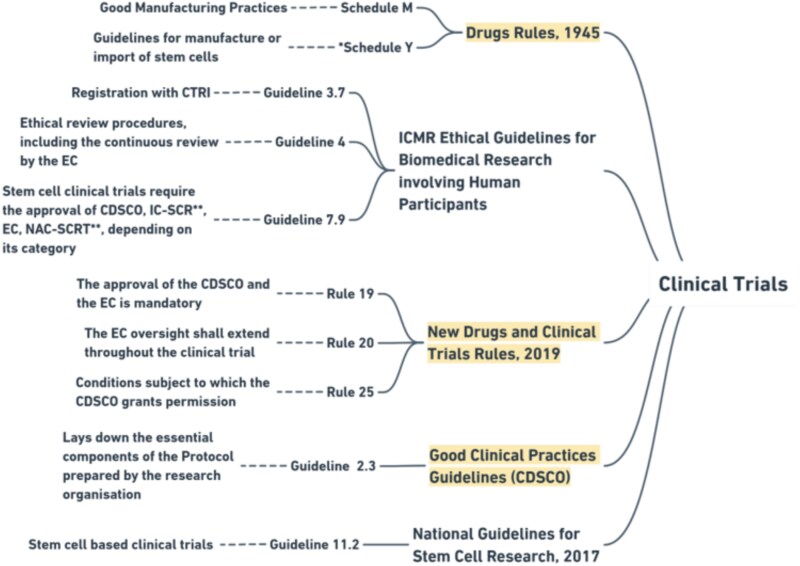 Figure 2
Figure 2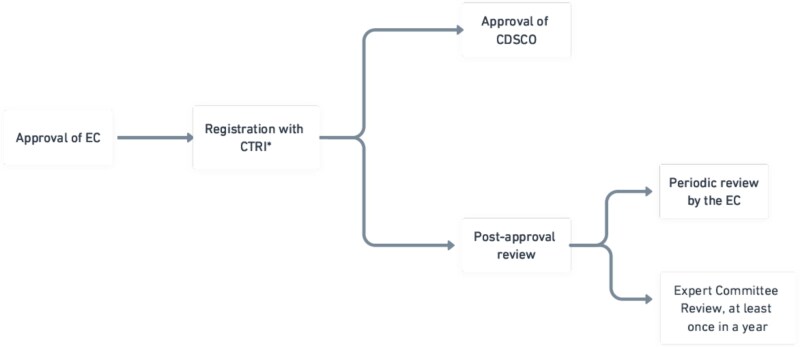 Figure 3
Figure 3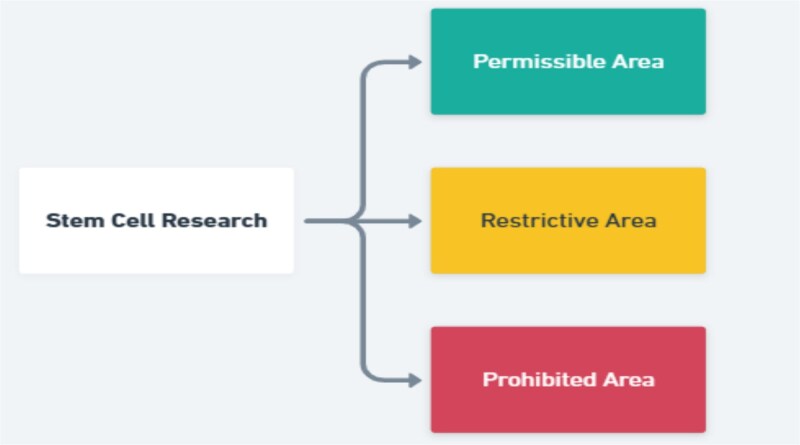 Figure 4
Figure 4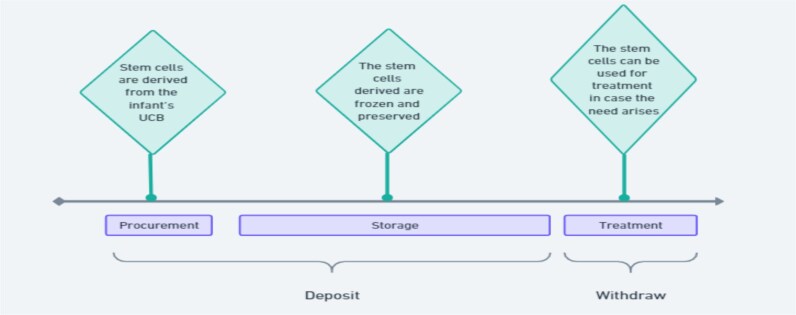 Figure 5
Figure 5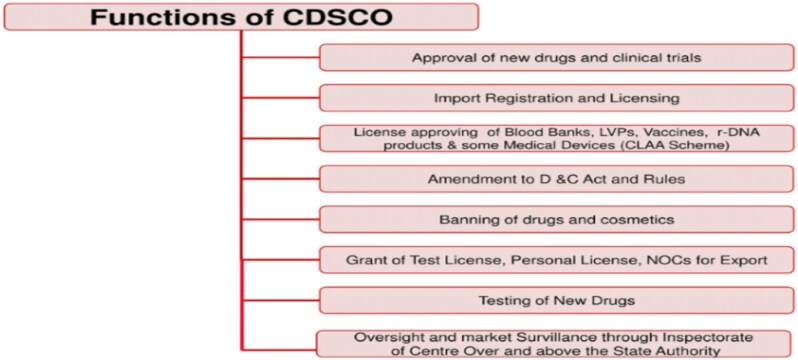 Figure 6
Figure 6|
|
|
|
|---|---|---|
| 1 | Orthopedic conditions and injuries | The clinical trial results are encouraging. However, with the available evidence, stem cell therapy is not recommended as the standard treatment. |
| 2 | Spinal cord injury (SCI) | While animal experiments and pre-clinical studies have shown positive results, the result of the clinical trial is not sufficient to confirm its effectiveness. Hence, not recommended for standard therapy. |
| 3 | Critical limb ischemia (CLI) | The existing studies and experts’ analysis do not support the use of stem cell therapy as the standard treatment. There is, however, a stem cell–based product, stempeucel®, that has been granted a market license by the CDSCO. It can be used only when the traditional treatment is not successful or possible. |
| 4 | Duchenne muscular dystrophy (DMD) | Due to technical limitations concerning the use of stem cells for this condition, studies do not support the use of stem cell therapy. One of the technical limitations is that stem cell therapy for DMD cannot be administered without genetically engineering stem cells to correct gene defects—a technique that is still under study. |
| 5 | Autism spectrum disorder (ASD) | Existing studies do not support the use of stem cell therapy for ASD, either as a replacement for or as an addition to the current therapies. |
| 6 | Lysosomal storage disorder (LSD) | The use of stem cell therapy is not recommended due to the limited number of clinical trials and weak evidence base. However, with proper supervision of experts, the use of HSCT is permitted in Hurler syndrome for children below the age of 2 years. |
| 7 | Amyotrophic lateral sclerosis or motor neuron disease (MND) | The existing studies do not support the usage of stem cell therapy as a standard treatment. |
| 8 | Stroke | Though there are a few clinical trials studying the use of stem cells for treating (ischemic) stroke, the available evidence is inadequate due to various reasons. Hence, the use of stem cell therapy is not recommended. |
| 9 | Multiple sclerosis (MS) | The existing studies do not support the use of stem cell therapy as an addition to or replacement of standard treatments. |
| 10 | Heart failure | The clinical trials have not yielded consistent results so far. Hence, stem cell therapy can be administered only within the framework of clinical trials, but not as standard treatment. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiomedical Ethics and Regulation · Pluripotent Stem Cells Research · Biotechnology and Related Fields
I. INTRODUCTION
With the advent of the 21st century, stem cell research has acquired considerable prominence and many countries across the globe have actively taken up this project.1 Starting from restoration of vision to curing diabetes, stem cell–based clinical trials have hit the headlines multiple times in the past months.2
A stem cell is a type of cell that can differentiate itself and regenerate into a large number of new cells.3 Stem cell science is witnessing ground-breaking academic inquiries,4 and it appears to offer promising therapeutic applications, thanks to its self-renewal capabilities.5 At the global level, the International Society for Stem Cell Research promotes ethical research in the field and issues guidelines and standards for stem cell clinical trials.6
While we have these international guidelines, the degree and nature of regulations vary widely from one country to another. For example, while stem cell research is more tightly regulated in India through licensing and approval procedures, the process is more relaxed in some countries like the USA.7 Today, India is seen as one among the promising destinations for cell therapy with further potential for growth.8 This prompts a review of the readiness of regulatory practice in India.
Indian law categorizes stem cell derivatives as a ‘new drug’ for the purposes of clinical applications.9 As a result, regulation of its research falls squarely under the broader framework of drug regulation. The incorporation of stem cells within the drug regulatory framework has been a slow process—it was only in 2018 that a proposal was made to categorize stem cells as drug and thereby bring it under the regulatory scanner.10 However, before this proposal materialized, the New Drugs and Clinical Trial Rules, 2019 was released, which introduced the category of ‘new drugs’, bringing in ‘cell- or stem cell–derived product’ in its ambit.11
Parallel to these legal developments, we have witnessed the rise of several government-funded research projects related to stem cells in the past decade.12 Unlike its European counterparts, India has adopted a relatively liberal stance towards embryonic stem cell research.13 It has witnessed an appreciable growth in stem cell research and clinical trials.14 Albeit, it appears that at a global level, the quality of India’s research output continues to be sub-par.15 It can be, among others, attributed to the absence of a robust regulatory framework, a problem that is the focal point of my analysis.16
The concern here is not just about protecting the research environment. The safety of patients who fall prey to the tall promises of unscrupulous actors in the stem cell industry is an equally grave, if not graver, concern.17 Considering the alarming nature of the matter, the paper calls for policy intervention to protect the interests of the patients and consumers.
The primary agenda of this paper is to advance a set of reforms India can adopt to optimize its regulatory practices. The first part of the article sets out the existing regulatory framework characterized by overlapping laws and guidelines and overburdened regulators. While the existing literature highlights several issues in the regulatory framework, the discussion has been quite generic from a legal scholarship viewpoint. Hence, this part seeks to firstly, take up a legal analysis of the laws underpinning the framework, and secondly, to link the specific legal inconsistencies to the practical effect of regulatory failure.
I engage with various primary documents to explain the regulation of different aspects of stem cell science—namely, clinical trials, therapies, use of human embryonic stem cells (hESCs), stem cell banking, and advertisements. To make up for the gap in the information, and to confirm some of the inferences, the responses received to the ‘Right to Information’ queries filed by the author has been relied upon.
The second part of the article discusses the systemic defects plaguing the regulatory mechanism. These systemic defects deter quality research and facilitate the proliferation of clinics offering unproven therapies under false and unscientific promises.
The reforms suggested in Section IV broadly cover the areas of funding, clinical regulation, and public engagement. While acknowledging the inherent difficulties, the article proposes enactment of a consolidating law to harmonize the regulation of stem cell research. Yet, a clear and fine piece of law alone might not suffice. Through this article, I re-emphasize the long-standing demand for restructuring the institutional framework involving the Central Drugs Standards Control Organization (CDSCO) and the State Drugs Regulatory Authorities (SDRAs) to ensure better coordination and uniformity in the practices. Further, it is necessary to facilitate structured state funding of research to ensure a holistic growth of stem cell science in India. It is important to allocate state funds to support projects in the interest of the public that are otherwise ignored by profit-driven private laboratories and organizations. As a final measure, I highlight the importance of sensitizing the public and empathetically engaging with the patients through support groups, to prevent exploitation and to support those in distress.
While the existing literature provides principled discussion on the issues foundational to the regulatory failure,18 it does not extensively and conclusively discuss the specific legal and policy changes that can be brought in a country like India. I attempt to highlight particular measures for reform, starting from statutory measures to direct public engagement. And in this process, I also attempt to close the chasm that exists between one part of literature that broadly calls for positive legal reforms19 and the other part highlighting the limitations of such measures.20
While many social scientists have highlighted the inadequacy of a new law, the article tries to convey that a clear, consolidated statute is necessary in the Indian scenario. But such a law and the surrounding institutional mechanism must account for the political, economic, and social forces. This inquiry aims to lay a groundwork for the legislature and the regulators in tackling the issue and possibly act as a legislative exemplar for other countries in a similar bio-legal context.
II. THE INDIAN REGULATORY FRAMEWORK ON STEM CELLS
Indian policymakers’ efforts to monitor stem cell research began at the dawn of the 21st century.21 In 2001, the Department of Biotechnology (DBT) issued guidelines in response to the rising number of instances of misuse of stem cell science for unapproved clinical applications.22 Later, in 2002, the Indian Council of Medical Research (ICMR) announced a policy in favor of stem cell research and therapeutic application.23 It was only in 2007 that both the DBT and the ICMR, the two principal policy-formulating institutions,24 came together to issue national-level guidelines.25 Since then, there have been quite a few regulatory developments like the establishment of the Cell Biology Based Therapeutic Drug Evaluation Committee (CBBTDEC) within the CDSCO in 2010, and the enactment of the specific clinical trial rules in 2019.26
Currently, stem cells are regulated through the drug regulatory framework, and hence, it comes under the ambit of Drugs & Cosmetics Act, 1940 (D&C Act).27 However, it is important to note that though the D&C Act is a Union legislation, there are certain constitutional limitations in the central drug regulatory framework. With respect to the purview of the federal and the state legislatures, the Indian Constitution lays down three lists—the Union List, where the Parliament can legislate upon, the State List, where the state legislatures exercise the sole authority, and finally, the Concurrent List, where both the Parliament and the State Legislature exercise authority.28 The matter of ‘public health’ (and hence drug regulation) comes under the purview of the state legislature.29 As a result, the state governments exercise considerable autonomy in setting the rules and enforcing standards.
While we have the Drugs Controller within the CDSCO as the central regulatory body under the D&C Act and the Drugs Rules, 1945,30 many of the core regulatory functions are exercised by the state-level SDRAs. In practice, while CDSCO regulates aspects regarding clinical trials and new drug approvals, functions related to regulation of manufacturing and distribution of drugs are carried out by SDRAs.31 And since the CDSCO and the SDRAs work independently of each other, the former does not exercise any vertical control over the latter. This federal angle of the Indian public health system is often ignored in scholarship on the stem cell regulatory framework.32 This has often led to broad calls for new laws, centralized registry, and more stringent measures, without acknowledging the power-sharing dynamics between the federal and regional regulators.
Before proceeding to the next section, it should be noted that the ‘Indian regulatory framework’ refers to the set of legislations and guidelines, and the corresponding institutions which govern stem cell research and allied activities in India. A high-level overview of the framework is provided in Fig. 1.
*The Regulatory Framework. The red box depicts statutes (enforceable), and the blue box depicts guidelines (unenforceable). CDSCO, Central Drugs Standards Control Organization; IC-SCR, Internal Committee for Stem Cell Research; EC, Ethics Committee; ICMR, Indian Council of Medical Research; MCI, Medical Council of India; NAC-SCRT, National Apex Committee for Stem Cell Research and Therapy; NGSCR, National Guidelines for Stem Cell Research. NAC-SCRT and IC-SCR are no longer active institutions.
The role of these institutions and statutory instruments or guidelines is distributed across various areas in stem cell research, namely, clinical trials, therapy, use of hESCs, stem cell banking, and advertisements of therapies/products. Unfortunately, the information available in the public domain is scarce and insufficient to draw a complete picture on the approval and licensing procedures.33 However, through additional information obtained via Right to Information (‘RTI’) queries, the subsequent sections aim to provide an overview of the framework.34
II.A. Clinical Trials
According to the World Health Organization (WHO), ‘clinical trials are a type of research that studies new tests and treatments and evaluates their effects on human health outcomes’.35 Stem cell–based clinical trials are necessary for the expansion of therapeutic application of stem cells, and this is an area of research that promises cure for serious diseases.36 With 117 clinical trials involving stem cell–based intervention registered in India,37 regulation of clinical trials occupies an important position within stem cell governance.
As evident from Figs 1 and 2, organizations conducting clinical research are required to adhere to a catena of laws and guidelines. Clinical trials are regulated by the central-level laws—most importantly, the Drugs Rules, 1945 (‘Drugs Rules’) and the New Drugs and Clinical Trial Rules, 2019 (‘CT Rules’). These rules mandate a multi-tier approval process for different types of clinical trials.38 According to the CT Rules, the approval of an institutional body called ‘Ethics Committee’ (EC) is the first step before conducting clinical trials.39 The institution conducting the trial has to constitute an EC and register it with the CDSCO.40 The EC reviews the proposals for clinical trials, periodically supervises the conduct of clinical trials after the approval, oversees compliance with the Good Clinical Practices (GCP) standards prescribed by the CDSCO, and reports to the CDSCO in case of adverse consequences.41 From a simple perspective, ECs act as institution-level nodes of CDSCO.
*The statutory framework governing clinical trials in India (the highlighted elements are the ones which are enforceable by respective agencies through direct or indirect means). This figure represents only a few important provisions among the relevant ones. *The New Drugs and Clinical Trials Rules, 2019 overrides the Schedule Y guidelines. *IC-SCR and NAC-SCRT are no longer active institutions.
*A brief representation of the clinical trial approval process. CTRI, Clinical Trials Registry—India.
Once the EC approves it, the organization has to make an application for grant of permission to the CDSCO through Form CT-04 under the CT Rules42 and/or43 Form 44 under the Drugs Rules.44 The CDSCO grants permission under Rule 22 of the CT Rules based on various factors mentioned in Rule 122DAC of the Drugs Rules, including the adherence to the GCP, and compliance with the approved protocol.
As evident now, the approval process features a certain degree of regulatory audit. In the first level, the EC is required to monitor the clinical trial site. In addition to this, the CDSCO can authorize officials to conduct on-site inspections even without prior notice.45 Also, according to a notice of the CDSCO in 2013, the zonal offices of the CDSCO are required to constitute an expert committee for the conduct of inspections of sites under their jurisdiction at least once a year.46 This ensures that the organization adheres to the required rules and regulations even after the permission is granted.
From Rule 122DA of the Drugs Rules, one can also understand that there are three phases to clinical trials, each of which requires separate permission from the EC and the CDSCO.47 In certain cases—ie when the clinical trial intended for academic purposes is based on an already approved drug formulation, and it only deals with any new indication or new route of administration or new dose or dosage form of that drug—the approval of the CDSCO is not required once the EC green flags it.48
Once approved by the EC and the CDSCO, the next step in line is to register the clinical trial with the national-level registry of clinical trials called the Clinical Trials Registry of India (CTRI), set up in 2007.49 Since 2018, it has been mandatory to register a clinical trial before the enrolment of the first patient.50 This step ensures that the details of clinical trials are publicly available, facilitating transparency and public awareness and preventing repetitive studies.51
Regarding stem cell–based trials, we also have the National Guidelines on Stem Cell Research, 2017 (NGSCR 2017), jointly released by the ICMR and the DBT.52 It covers a wide array of issues ranging from stem cell therapy to banking. The first version of the guidelines was released in 2007, titled the ‘Guidelines for Stem Cell Research and Therapy’.53 The subsequent versions were released in 2013 and 2017 but without the term ‘therapy’ in their titles.54 In addition to the NGSCR, ICMR released the ‘National Ethical Guidelines for Biomedical and Health Research Involving Human Participants’ in 2017, which sets out the measures that the organization or researcher needs to adhere to while conducting clinical trials on human subjects.55
While these guidelines provide details concerning the approval procedure, there is no binding mechanism to ensure adherence to these guidelines. On one hand, the DBT and the ICMR, which issued the guidelines, do not have any enforcement powers to mandate compliance.56 And, on the other hand, the NGSCR guidelines do not have any legislative backing57—that is, neither the Drugs Rules nor the CT Rules particularly require compliance with the NGSCR guidelines for stem cell–based clinical trials.
Specifically, the NGSCR 2017 mandates the approval of an ‘Institutional Committee on Stem Cell Research’ (IC-SCR), registered with the ‘National Apex Committee on Stem Cell Research and Therapy’ (NAC-SCRT).58 However, this two-tier arrangement of IC-SCR—NAC-SCRT was, dissolved in March 2024, citing difficulties in implementation.59 Before its dissolution, IC-SCR was to NAC-SCRT, like how EC is to CDSCO.60 The IC-SCR used to be an EC-like institutional level body associated with the evaluation of clinical trials. It was responsible for reviewing the research protocols, evaluating the compliance with the guidelines, and maintaining a record of the research activities of the institution.61 Since the NGSCR has not been updated since 2017, the IC-SCR and the NAC-SCRT still appear in the guidelines.
The NGSCR classifies stem cell research into three categories—permissible, restrictive, and prohibited.62 However, clinical trials, irrespective of the category they fall in, require the approval of the EC and the CDSCO.63 Previously, it was doubtful whether the approval of IC-SCR is mandatory in practice, as the Drugs Rules and the CT Rules are silent on the same, and the NGSCR Guidelines are not legally enforceable otherwise.64 With the dissolution of the IC-SCRs and the NAC-SCRT, this ambiguity no longer exists. Currently, clinical trials require the approval of EC and registration with the CDSCO.65
According to the NGSCR 2017, clinical trials using human stem cells are required to adhere to good manufacturing practices (GMPs) in Schedule M of the Drugs Rules,66 CDSCO’s GCP, and the ICMR Ethical Guidelines for Biomedical Research involving Human Participants67 in addition to other provisions of the CT Rules, the D&C Act, and the Drugs Rules.
While that is about the conduct of clinical trials, there are also stipulations regarding the qualification of the researchers. The medical professional undertaking the clinical research must be registered with the National Medical Council (NMC) and must have an NMC-approved postgraduate qualification specializing in the domain area of the clinical research.68
II.B. Stem Cell Therapy
II.B.1. Bone Marrow Transplantation
In India69 and in many other countries,70 the only recognized stem cell therapy is the bone marrow transplantation (BMT), also known as the hematopoietic stem cell transplantation (HSCT). The application of all other stem cell interventions is considered experimental and is restricted to clinical trials.71 The reason being that the safety and the therapeutic efficacy of other forms of stem cell therapy are still doubtful and unclear.72
While the BMT comes under the umbrella term of stem cell therapy, the NGSCR is considered inapplicable over it as BMT is now a ‘well-established’ and standard form of treatment.73 The ICMR released separate guidelines for BMT, termed the ‘National Guidelines for HSCT’ in 2021.74 The guidelines classify the application of BMT into four categories—‘standard of care’, ‘clinical option’, ‘developmental’, and ‘generally not recommended’.75
In the case of indications coming under the first category, the BMT is considered a standard option and is carried out without further oversight.76
For indications under the category of ‘clinical option’, the application of BMT is considered risky. The patients must be thoroughly briefed about the benefits and risks of the treatment, and the treatment must be carried out only in a specialized setting by well-experienced practitioners.
The third category is for cases where the application of the BMT is considered ‘developmental’ due to ambiguity regarding the role of HSCTs for certain indications. In such cases, the BMT must be preceded by the approval of the transplant protocol by a local ethics committee.
Apart from the above cases, there are also indications for which the BMT is not recommended, and such indications fall within the fourth category. These also include cases where further research is required to ascertain the efficacy of BMT. The guidelines call for more research into the application of BMT for indications under the third and fourth categories.77
II.B.2. (Unproven) Stem Cell Therapies Still under Research
Currently, clinical trials are being conducted across the globe with the hope of leveraging stem cell therapy for a host of chronic or grave diseases.78 Table 1 provides a list of conditions79 and comments regarding the potential stem cell treatments.
Categories of Stem Cell Research under the NGSCR 2017.
In essence, stem cell therapies other than BMT are still in the experimental stage. There is a need for further research to establish their safety and efficacy. According to the NGSCR 2017, the investigator ought to apply to the ICMR when the clinical trial appears to be promising in terms of a potential therapy.81 ICMR will examine the tenability of the claims in consultation with the experts.82
Clinicians administering unproven therapies outside the framework of clinical trials can be held liable for ‘misconduct’83 and shall face appropriate disciplinary actions under Chapter 8 of the IMC Regulations.84 In the event of any injury caused to the patient, they can be held liable under the Bharatiya Nyaya Sanhita, 2023,85 which is the principal Indian penal law and the Consumer Protection Act, 2019.86 Further, the laws prohibit clinicians and hospitals from advertising such treatments; more on this can be found later in this part.
II.C. Approach Toward the Usage of Human Embryonic Stem Cells
The use of hESC for stem cell research is a matter of ethical and legal debate in many jurisdictions.87 The hESC is a type of pluripotent stem cell, meaning that they have the innate ability to regenerate itself indefinitely into distinct cell types, including specialized cells. In other words, clinical applications involving hESCs can potentially treat several incurable degenerative diseases that were incurable otherwise.88
However, the clinical applications involving hESCs are considered controversial due to underlying ethical questions pertaining to the onset of personhood.89 The proponents of embryonic stem cell research argue that an embryo is not a person, and it is ethical to use embryos for the purpose of research and clinical applications.90 On the other hand, the opponents argue that an embryo is a part of the continuous development of a ‘person’ and that destroying embryos on the basis of potential benefits is unethical and immoral.91 However, it appears that the development of ‘induced pluripotent stem cells’ (iPSCs) has addressed some of the above concerns.92 iPSC is a type of stem cell that can be obtained from non-embryonic sources but can be reprogrammed to achieve the features of an embryonic stem cell.93 As a result, iPSC enables a researcher to avail the benefits of embryonic stem cells without destroying any embryo.
The Indian framework permits both the creation of embryos and the limited usage of surplus embryos for stem cell research.94 The Assisted Reproductive Technology (Regulation) Act, 2021 allows research on human gametes and embryos ‘within’ India, and such research has to comply with the guidelines issued by the ICMR.95 The NGSCR Guidelines issued by the ICMR and the DBT categorize areas of research as ‘permissible’, ‘restrictive’, and prohibited’ based on the source of the stem cells and a few other factors.96 The establishment of new hESC lines from spare embryos falls within the permissive category.97 On the other hand, the creation of human embryos in vitro, for the purpose of deriving hESC lines, is placed under the ‘restrictive category’, requiring the investigator to prove that the creation of embryos is necessary for conducting the said study.98 This approach, which may be qualified as progressive by some, differs from that of other countries, including many European countries.99 The Guidelines also conform to the universally accepted ‘rule of 14 days’—that is, human embryos cannot be used for derivation of stem cell lines if 14 days have passed after fertilization, or if a primitive streak has appeared on the embryo, whichever is earlier.100 This is categorized as a prohibited area of research.101
II.D. Stem Cell Banking
Stem cell banking is an emerging business in the stem cell industry; it can be plainly defined as ‘a procedure wherein the cells isolated from various sources are collected, proliferated, stored and preserved for their future use’.102 India permits only umbilical cord blood (UCB) banking—which is subjected to the approval and license of the CDSCO.103 The ICMR banned banking in all biological materials other than UCB in 2017 (see Figure 5 for the general model of functioning of the UCB banks).104
The 2011 amendment to the Drugs Rules brought UCB banking under its ambit.105 For setting up a UCB bank, the applicant has to file Form-27F under the Drugs Rules with the CDSCO106 and it subsequently grants the license on the basis of on-site inspection.107 UCB banking can be private or public. In public banking, people donate UCB for future use by any patient. In private banking, the donor deposits the cord blood in the bank, which can be retrieved in the future at their will for their own use.
Various private enterprises offer the storage of cord blood, promising future therapeutic use. Such advertisements can be misleading. According to the NGSCR, the therapeutic application of stem cells derived from the UCB shall be limited to HSCT-related indications set out in Annexure III. In other cases, the stem cells derived from UCB shall be used only for clinical trials.108
A simple web search on ‘stem cell banking’ will expose one to umpteen numbers of private ventures advertising the benefits of UCB banking and positing exaggerated and unverified claims of the potential of stem cells derived to cure ‘life-threatening’ diseases. The private players often market UCB through blanket statements that bely the actual utility of private stem cell banking,109 a practice that exploits the lack of sufficient awareness among the lay people.110
Based on complaints of such malpractices, the ICMR issued the ‘Guidelines for Umbilical Cord Blood Banking’ in 2023, which lays down the general standards that a bank must follow. It provides for measures to deal with use of misleading advertisements and publicity by the banks.111
II.E. Misleading Advertisements and Claims
It is not uncommon to see clinics and hospitals reaping exorbitant profits by offering stem cell treatment for certain diseases, under the guise of clinical trials.112 There have also been instances where misleading advertisements used the photographs or addresses of prominent scientists to justify their claims.113 Three principal statutes address the issue of illegal advertisements and the popularization of stem cell therapy,114 viz., the Drugs and Magic Remedies (The Objectionable Advertisements) Act,115 the Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations, 2002 (‘IMC Regulations’)116, and the Drugs Rules (specifically note, Schedule J).117 These legislations provide for a range of punishments varying from cancellation of license to imprisonment and are enforced by respective regulatory institutions.118
The DMR Act and the Drugs Rules empower the Directorate General of Health Services and the CDSCO to take steps in coordination with SDRAs against misleading advertisements.119 In the case of UCB banks, a complaint regarding misleading claims can be sent to the nearby zonal branch of the CDSCO.120 Additionally, regulation 6.1 of the IMC Regulations precludes clinicians from advertising themselves through any mode.121 The NMC and the Medical Councils (MCs) of the respective states have the power to revoke the license of the clinicians in case of violation of the Regulations.122 Further, it is possible to take steps under the Consumer Protection Act, 2019123 in case of misleading advertisements concerning stem cell products and therapy. Also, according to Rule 106 of the Drugs Rules, advertisements promising cure for or prevention of diseases mentioned in Schedule J of these Rules are prohibited.
The deterrent effect of this multifaceted regulatory mechanism against misleading advertisements and other forms of exploitation of potential consumers of ‘stem cell treatment’ is contingent upon the timely enforcement of these statutes and the proper exercise of the aggrieved party’s right to file a complaint.
III. A CRITICAL APPRAISAL OF THE INDIAN REGULATORY MECHANISM
The previous section provided a high-level overview of the Indian regulatory framework on stem cell research, clinical trials, and therapy. Given this background, the following section critically analyzes the extant framework.
Firstly, it is important to highlight the crisis of unproven stem cell therapies that we are facing. Since the 2000s, the popularity of untested stem cell interventions has surged over the years, across jurisdictions.124 By exploiting the vacuum in the Indian regulatory framework, practitioners and commercial enterprises have taken upon the (unconfirmed) promises of these therapies to lure the affluent and the growing middle class in India, and often times, the medical tourists from developed countries.125
Exploitative stem cell tourism has grown as a natural upshot of the proliferation of unscrupulous players. Stem cell tourism, a term that became popular over the past two decades, indicates the practice of patients travelling to avail unproven stem cell therapies based on online, direct-to-consumer advertisements.126 It involves desperate patients afflicted with serious conditions, who often seek affordable treatment in foreign countries, trying to exhaust all means available to them.127 The glimmer of unproven stem cell therapies touted as the all-round panacea by clinics has attracted a fairly large share of tourists to low- and middle-income countries like India, Thailand, Dominican Republic, and Mexico due to ease of travel and lower costs.128 Nevertheless, illegal stem clinics are also propping up in developed countries, including the USA, Japan, and Australia, by way of aggressive marketing.129
In India, the lax implementation, the consequent proliferation of illegal clinics, and the concerning trajectory of stem cell tourism lie in inadvertence and complacence than intentional relaxation of laws for attracting foreign investments.130 In other words, the growth of stem cell tourism in India lies in the face of loose regulations and lack of effective implementation of existing laws.131
Unscrupulous players in the industry have taken advantage of the overlapping, intricate, and porous regulations to further their business,132 a phenomenon that can be termed ‘regulatory arbitrage’. In a broad sense, regulatory arbitrage refers to the act of entities designing their transactions or activities in such a way as to take advantage of the gaps in the regulatory framework.133 For example, it is possible for a clinic to not comply with certain aspects of the ICMR guidelines on stem cell research and human-based clinical trials.134 They can argue that they are not part of any legal mandate set by the statutes.135 This has given profit-oriented clinics and practitioners the confidence to actively commercialize stem cell therapy and lure patients from India and abroad.136
This is not to suggest that the sky is all dark and cloudy here. In the early 2010s, we faced the fundamental problem of what Tiwari et al. describes as jurisdictional ambiguity—that is, the confusion over who possesses the authority to regulate stem cells and whether it is within the remit of the DCGI/CDSCO.137 However, with the amendments in the statutes over the subsequent decade, this ambiguity regarding DCGI’s/CDSCO’s jurisdiction over the issue has been resolved.138 Hence, it would be wrong to classify the legislature and the regulator as completely non-responsive. But, still, there are various factors on which the system has to improve.
Having set the context, I take up some of the critical issues that have led to the growth of unproven therapies in the upcoming paragraphs. It is not possible to regulate stem cell tourism without addressing these lacunae.139 Steps must be taken in this direction as the growth of stem cell tourism in the current manner is not only fatal140 to the vulnerable patients141 and to the reputation of India’s medical sector but is also at the cost of development of stem cell science.142
III.A. The Lack of Legislative Recognition for Critical Guidelines
The NGSCR issued by the ICMR and DBT does not have any legislative basis. Before 2019, one had to ensure compliance with the Schedule Y Guidelines to conduct a stem cell clinical trial.143 Now, instead of Schedule Y, stem cell trials are governed by the guidelines in the CT Rules. For example, Rule 25(vi) of the CT Rules mandates compliance with the GCP Guidelines.144
The point I am trying to make here is that, unlike the GCP guidelines, there is no provision in the statutes that mandates compliance with the NGSCR guidelines. No provision in the general law, ie, Drugs Rules and the specific law, ie, the CT Rules, demand obedience to the NGSCR guidelines as a prerequisite for stem cell trials. The implication is that violation of the NGSCR guidelines does not attract legal sanctions.145 It is also quite ironic that both the ICMR and the DBT, institutions responsible for promoting and facilitating biotechnology and biomedical research, do not have the power to enforce their guidelines and penalize the violators.146
It appears that practitioners have exploited this loophole in the past.147 One can see umpteen number of cases where stem cells are used commercially for unproven therapies, though the prescribed rule is that they cannot be used outside an approved clinical trial setting.148 This creates an ironic situation where, despite having ostensibly ‘strict guidelines’149 for the regulation of stem cell therapy, we are witnessing an unregulated sprouting of clinics promoting and providing stem cell therapies.150
The most pertinent example is the decision of the Delhi High Court in 2023 in *Dalip Kumar v Union of India.*151 Here, the Court had to permit a hospital to continue with the ongoing (unproven) stem cell therapy as part of the treatment for autism spectrum disorder (ASD) in two children, citing the potential hazards in abruptly ending the treatment. The Court went on to acknowledge that there was no law expressly banning the use of stem cell therapy for ASD.152
In the previous discussion on stem cell therapies, we saw that the ICMR clearly suggests against the use of stem cell therapy for ASD.153 Firstly, the question is how did the hospital initiate the stem cell therapy in express violation of the ICMR guidelines. Secondly, as understood from the Court’s reasoning, we lack a consolidated law that clearly delineates what is permissible and what is not permissible. These guidelines require statutory recognition to make it enforceable and thereby engender better compliance.154
III.B. The Systemic Procedural Ambiguity in the Approval and Oversight of Clinical Trials
Patra and Faulkner have pointed out the ‘increasing complexity of regulations’ as one of the factors that have enabled the players to circumvent scrutiny in India.155 But, from a legal prism, what makes these regulations complex? The answer lies in the often-incomplete information on the procedural aspects due to doubts on how the soft law interacts with the hard law.
For example, the D&C Act and Rules and the CT Rules lay down a definite application procedure for conducting clinical trials. Parallelly, the NGSCR Guidelines also lay down a procedure for the same. The former set of rules does not conflict with the latter guidelines, but the latter guidelines posit a few additional stipulations that the organization needs to adhere to. For instance, the NGSCR Guidelines stipulate that the clinical trials should comply with the ICMR Ethical Guidelines.156 However, the above compliance requirement is not mentioned in the provisions concerning clinical trials in the Drugs Rules and the CT Rules and can, therefore, cause confusion among the researchers.
Before the dissolution of the NAC-SCRT, there was a similar issue with regard to the requirement of approval from the IC-SCR. While the Drugs Rules and the CT Rules do not mandate approval from IC-SCR, let alone the constitution of a body called IC-SCR, the NGSCR Guidelines treated the same body as an important regulatory actor.157 With their dissolution, this issue has been solved—still, a large number of provisions in the NGSCR continue to deal with the oversight of IC-SCRs and the NAC-SCRT.
The above discussion indicates the absence of a clear and consistent regulatory environment, which is a prerequisite for a vibrant stem cell research ecosystem. As a result, an investigator going through the approval process would be faced with the dilemma of which stipulations to comply with. The ICMR Ethical Guidelines and the CT Rules were introduced in light of the under-regulation of clinical trials.158 However, despite being well intended, the regulatory framework appears nebulous in its current form.
This procedural ambiguity is harmful to the development of research activities. For example, the ambiguous network of rules, regulations, and guidelines on research approvals has disproportionately affected governmental and reputed research institutions while benefitting certain commercial private players, as highlighted by a member in the House of the People of the Indian Parliament.159
Additionally, the issue here is not just about the absence of any specialized provision or legislation for stem cell research. It is also about the long-term relevance of the NGSCR Guidelines if it is not mandatory in the first place. This regulatory uncertainty is one of the primary issues that needs to be addressed.
III.C. Lax Implementation of the Law Despite Blatant Violations
It appears that even enforceable aspects of the regulatory framework are under-implemented.160 Barring the ambiguities in the framework, a neutral and bare reading of the legislations and guidelines does give an impression of a fairly well-designed system in place.161 For example, there are multiple laws that penalize misleading and fraudulent advertisements.162 We have a set of legislations consisting of the IMC Regulations (2002), The Drugs and Magical Remedies (The Objectionable Advertisements) Act (1954), the Drugs and Cosmetics Act (1940) and Drugs Rules (1945), Bharatiya Nyaya Sanhita (2023), and Consumer Protections Act (2019), which enable a person to seek civil and criminal remedies.163
However, in praxis, it is doubtful whether the associated institutions effectively exercised the powers available under these legislations, with the regulatory framework yielding to various socio-political factors.164 For example, Nutech MediWorld, led by Dr Geeta Shroff, is a private player that continues to advertise regenerative therapies for ‘incurable conditions’,165 despite it having being brought to the center of various controversies and disputes before.166 After all, India is currently in a situation where we are doubtful whether even the public institutions, let alone the private players, are complying with the framework in place.167
III.D. The Inefficiency of the CDSCO due to Burdensome Separation of Duties
Another major drawback is the fragmented style of regulation in India. From the previous discussion, it is apparent that the framework involves multiple players functioning in overlapping areas, with no set workflow. This has not only led to uncertainty and confusion among clinicians but also created doubts regarding distribution of functions among the regulators themselves.168
Notably, parallel to vagueness in distribution of duties, there also exists ‘jurisdictional overload’. On one hand, the CDSCO is entrusted with a long list of functions. On the other hand, the CDSCO is not supported by sufficient resources.
As already noted, CDSCO is the primary actor whose jurisdiction extends over a wide aperture within the arena of stem cell research. However, CDSCO is a general regulatory body whose purview is not limited to stem cell research but extends to the whole catena of drugs and clinical trials in India.169 The broad functions of CDSCO, as provided on its website, are elucidated in Fig. 6. An institution like the CDSCO, which is entrusted with a wide range of matters within the field of drug regulation, is charged with the duty of regulating a highly niche field of biomedical research that is growing at an unprecedented rate.
The general model of stem cell banking in India.
Functions of the CDSCO as provided on their website.
Secondly, these broad and hefty functions of the CDSCO coincide with the fact that it is abysmally understaffed and low in resources.170 The 59th Report of the Department-Related Parliamentary Standing Committee on CDSCO highlighted the poor enforcement of the rules due to low capacity, including the disproportionately low number of inspectors to monitor the system.171
Further, the coordination between the CDSCO and the MoHFW is lacking. The most striking example that evidences this is the 2016 ban imposed by the Central Government on fixed dose combinations—an instance when the Government imposed a ban disregarding the prior approvals of the DCGCI (CDSCO).172 All these go on to show that the current institutional arrangement is not equipped well to handle the rapidly changing stem cell market.
IV. What Can be Done to Improve the Situation?
The previous part dealt with the inherent shortfalls and fault lines in the Indian regulatory mechanism. The subsequent discussion posits tangible reforms which can plausibly address the maladies of the Indian framework.
IV.A. Consolidation of Laws for Clarity and Uniformity
IV.A.1. Why Do we Need a Special Consolidating Law?
The first step to clear and effective implementation of the law is to ensure that the law is accessible, known, and clear. In the case of stem cell regulation, we already saw that the rules are spread out across legislations with little harmony; this makes enforcement and inducing compliance incredibly difficult. The legal problem here is clearly evident from the dilemma faced by the Courts when faced with a dispute over the legality of the treatment—that is, there is no clear law that clarifies which kind of therapeutic application is permitted173 and no policy direction on which and what licenses are required for delivering stem cell therapies and what action to take in the case of unlicensed clinics.174
To close this gap, the paper advances enactment of a special consolidating legislation to lay down a clear licensing and approval procedure, a distinct categorization of embryonic research, and a clear separation of the roles of the involved institutions. It might indeed appear ironical when I suggest a single law as a solution to the above-discussed complex problem. Here, it is to be noted that such a consolidating law is just a primary step forward toward better regulation of stem cell research. As pointed out by Dr Amit Prasad, the generic argument for a new law to solve the issue of unscrupulous stem cell therapy ignores the nuances of the patients’ needs and the larger socio-political context.175 There is a need for a more studied and careful approach to regulating stem cell therapy, keeping in mind the dynamics of patient welfare and support, which is emphasized toward the latter half of this part on reforms.
However, to start with, what we require for better regulation is clarity in the laws—which is necessary not only for the regulators to enforce it but also for the players to comply with it. In the Indian context, we are lacking greatly on that count. Our existing laws also do not conceive a clear demarcation of powers between the state-level SDRAs and the federal-level CDSCO, leading to ambiguity in the regulatory approach. There is also no standard procedure for taking care of the aggrieved patients who might not just be seeking a remedy against the malpractice but also looking for alternative healthcare support. Hence, there is a need for specific legal mechanisms and safeguards176 for addressing this issue, which is not feasible to introduce as amendments to the existing drug law.
Enacting a law on this matter is significant for another reason too. Regulation of stem cell research involves morally and ethically contested issues of creation and use of embryos. Therefore, the legal and ethical sides to the issue need to be debated in the Parliament by the representatives of the people to synthesize and develop a policy vision for undergirding the regulatory framework.177
Finally, one might be skeptical toward a suggestion for such a specific law when there is no counterpart for it in other advanced jurisdictions like the USA, the UK, or Japan. In the case of the USA, like in India, the regulation of stem cell therapy is handled by the drug regulator, the Food and Drug Administration. The network of laws in the USA creates a gradation of different levels of regulation depending on the level of manipulation of cells and other factors.178 The regulators in the USA have also been quite prompt in responding to the unscrupulous players and proactively communicating with the public,179 thanks to their strength and capacity in comparison to their Indian counterpart.180
In the case of the UK, they have the Human Tissue Act, 2004 and the Human Embryology and Fertilisation Act, 2008, which cover non-embryonic and embryonic stem cell research, respectively.181 In the case of Japan, they have the Act on the Safety of Regenerative Medicine, 2014, which deals with stem cell research on a comprehensive scale, starting from research to care and therapeutic application.182
The catch here is that the specific legal context in these jurisdictions does not demand a special law for stem cell research but rather incremental amendments to these to adapt to the developments and improvise governance.183 Similarly, the need for a special law has to be situated within the bio-legal context of India,184 which has been explained in length in the previous paragraphs and sections. What we require is a law that the courts and the regulator can undoubtedly rely on when faced with a complex situation involving various nuances.
IV.A.2. What Does Such a Law Entail?
To analyze the characteristics of such a Stem Cell Regulation Act or SCR Act, it is convenient to divide the process into two stages—the stage of law-making and the stage of policy implementation. The stage of law-making involves designing policies and schemes and giving effect to the same through legislation or legislative amendments.
Since ‘public health’ is the legislative forte of the state, constitutional constraints are applicable in enacting a full-fledged SCR Act.185 However, from the existing regulatory practice, regulation of clinical trials and new drug approvals still comes under the central purview.186 Hence, a national-level SCR Act may still be enacted to govern stem cell–based clinical trials.
So, the SCR Act shall:
Clearly define stem cells and their derivatives.Adopt a risk-based classification of SCPDs, say based on the level of manipulation.187Categorize embryonic stem cell research as given in the NGSCR 2017.Lay down a specific procedure for application for clinical trials, including a flexible yet definite list of standards or guidelines that need to be adhered to. Ideally, the NGSCR 2017, and the ICMR Guidelines on Biomedical Research involving Human Subjects shall be given statutory recognition through these provisions.Set up a protective net for the safety and welfare of human subjects in these trials through a rights-based approach through patient disclosure and consent protocols.188 If the patient is opting for an unproven therapy in a clinical trial setting, then higher standard of voluntary free informed consent and associated protocols must be set.189 Note that patients undergoing experiential therapies in a clinical trial setting should not be charged any amount for ‘treatment’ but is rather voluntary.190 In case of injury or death, there should be a provision for interim compensation on an immediate basis.191Provide a reasonable timeline for the completion of the licensing and approval procedures.Provide for periodic inspections of the clinical trial site.192 Inspections are highly important, and their significance can be understood if one looks into the USA. Despite having a proactive regulator, one of the factors that has enabled the unscrupulous players to slide through the regulations has been the rarity of FDA inspections.193 Also, establish a ‘stem cell research fund’ to enable a harmonized and effective system for supporting research.194In the case of proven or approved stem cell therapies, specify the minimum qualifications of the clinicians administering stem cell therapy such that they have reasonable experience and training in clinical stem cell science.195Specify the procedure for approval and licensing of stem cell banks, along with the list of standards and guidelines that need to be complied with.Lay down the penalties for violation of the law, with imprisonment in cases where the health of the patient/trial subject is endangered. For example, in the UK Clinical Trials Regulation, it is a criminal offense to conduct clinical trials in violation of the regulations or unscrupulously sell experimental medicinal products without authorization.196
Before finalizing the procedure, the penalties and other details in the SCR Act, the government should exhaustively study the current stem cell research environment in India. Questions and matters on stem cell research in India have been raised by the Members of the Parliament an umpteen number of times before, and it has become a recurrent matter of debate in the Parliament.197 Yet, it is surprising that no Parliamentary study has been conducted so far to evaluate the concerns and identify the issues plaguing the weak regulatory mechanism—this could be a reason why there is no sufficient data regarding the proliferation of unproven therapies and why this issue is still behind the shadows, away from the ken of the mass. Before framing the law, a comprehensive expert study is critical to gather sufficient data and understand the dynamics of the stem cell research system—it is often the poor understanding of the system being regulated that leads to failure of the laws.198
In the field of biotechnology, there is increasing support for complementing hard laws with soft laws to ensure greater flexibility in dealing with the rapid developments.199 As already suggested above, the Act can lay down a general framework while mandating compliance with the specific guidelines of the ICMR, which can be amended and updated easily from time to time. The ICMR can also notify best practices that need not be enforced through hard law. Rather, it can incentivize compliance with them by ensuring benefits in the form of funding or other resources.200
While law-making is an important stage to be carried out with conviction, the subsequent stage of policy implementation is a harder task demanding astute judgment and continuous evaluation. In the case of lack of effective enforcement, NGOs and public-policy think tanks play a crucial role in pressurizing the Government. Further, the judiciary plays an important role here. The courts have used tools like ‘continuing mandamus’ to direct the agencies to effectively discharge their public duties and cater to the socio-economic rights of the people.201 The courts may also call for ‘performance audits’ to review whether the laws and regulations are effective and ably implemented.202 Accordingly, the legislature is expected to introduce amendments that address the lacunae in the regulatory framework.
IV.B. Setting Things Right with Regards to the Institutions
Irrespective of a clear and definite law, things can go wrong if the implementing institutions are ineffective.203 As already discussed, the CDSCO is currently an overburdened institution with an ambiguous radius of duties and functions. According to the 59th report of the Department Related Committee on Health and Family Welfare, the CDSCO is extremely understaffed and low in resources.204 A comprehensive study funded by the Thakur Foundation in 2019 identified grave issues with the functioning of the CDSCO and the state-level drug regulators in India, revealing a crumbling system with overworked staffs, dysfunctional testing laboratories, and poor record-keeping.205 In such a condition, monitoring the enforcement of standards and regularly inspecting the clinical trial sites would remain a distant reality.
Another issue that was discussed above was the lack of proper coordination between the Institutions. We saw the friction in the functioning between the technical role of CDSCO and the receptiveness of the MoHFW. Further, though we have a special sub-division on stem cell–based products within the Biologics division of CDSCO, it is unclear how it participates in the framing of the rules and guidelines. There is a need to establish a stem cell–specific regulatory division with its own workforce within the CDSCO to monitor stem cell–based clinical trials and conduct periodic inspections on the stem cell based clinical trial sites, with a special emphasis on those involving hESCs due to ethical concerns.
The coordination between the CDSCO and the SDRAs is also a grave concern. The SDRAs command regulatory purview when it comes to monitoring the manufacturing process and sale of SCPDS. There is a need to ensure that the practices regarding regulation of manufacture and sale is uniform across the states. In fact, the D&C Act had already envisioned the Drugs and Consultative Committee (DCC) to engender uniformity in the administration of drugs throughout India.206 However, the DCC to date still faces imminent challenges in ensuring uniformity.207 To ensure uniformity, there is a need for better coordination between CDSCO and SDRAs and between SDRAs themselves. This requires clear and unhindered channel of communication, something which is lacking currently.208
In short, there is an imminent need to restructure the CDSCO to ensure better coordination between the constituent bodies. We need to ensure that technical-policy framing or advisory committees like DTAB are staffed with members of apposite expertise and experience that convenes regularly and is updated with the dynamic research atmosphere. There is also a need to bring the ICMR, the premiere research institute on the matter, into the picture. The regulated players may often try to relegate themselves to lower degree of classification by exploiting the outdated classification in the law.209 To avoid this, it is necessary for CDSCO to collaborate with the ICMR on the latest developments in science and update the regulations promptly.
Further, a special regulatory division on stem cells should ensure that the rules regarding clinical trials are followed diligently. Since the function of such a division is to ensure ground-level enforcement of the rules, it should have a localized structure, with such divisions being instituted in the state-level drug regulatory authorities as well. For this localized structure to work, the coordination between the CDSCO and the SDRAs is crucial. While it is not constitutionally permissible to create a vertical hierarchy between the CDSCO and the SDRAs, smoother coordination can be facilitated through regular consultation and policy-framing sessions. In fact, not imposing a top–down control might be more favorable since the presence and prevalence of stem cell technology widely varies from one state to another.
Similarly, inspections mainly come under the purview of the SDRAs and the SCR Act being a central legislation would not able to compel the SDRAs to conduct inspections. However, it can enable the CDSCO to lay down non-binding guidelines and standards for inspections. Through consultative meetings between CDSCO and SDRAs, the state inspectors can be trained to follow the uniform guidelines and standards for inspection.210
Another issue at play is the regulation of the medical profession. Tiwari et al. has pointed out that enforcement of professional guidelines governing the medical practitioners is an important facet of stem cell regulation.211 What is important is that the State MCs should have the capacity to monitor and take disciplinary actions in instances where the practitioner is found to violate the regulations.212 From the patients’ perspective, it is believed that an interim compensation mechanism, suggested above, would provide an immediate reprieve in cases of untoward consequences. Again, for this, the dispute resolution infrastructure involving the consumer fora and civil and criminal courts need to be strengthened.
Talks and discussions on restructuring the institutional framework has been active for some time in light of several issues on drug regulation coming into the light.213 With the growing burden of protecting the people from unproven stem cell therapies and saving the researchers from inconsistent procedures, the call for reforms is the loudest now.
IV.C. Establishing a Dedicated Funding Mechanism
On the face of it, the question of better funding might appear out of place in a discussion on regulation. However, the issues of who is responsible for funding and how and on what basis research is funded are all questions that are central to ensuring ‘clarity’ in the institutional framework. A clear and well-defined program is closely connected with the previously discussed need for a set workflow for institutions with clear separation of functions. In addition to the regulatory benefits, a formal funding plan with a defined vision is helpful in incentivizing basic research as well as public welfare targeted research, thereby allowing private entities to take up advanced research.214
In India, the government funds stem cell research through institutions like the ICMR, the DBT, and the Department of Science and Technology (DST).215 However, there does not appear to be a defined and consistent funding strategy for stem cell research. The funding has remained noticeably inconsistent over the years—in 2019, the total funds released by ICMR under stem cell research for fellowships and ad hoc projects were Rs 4,36,19,531/−; this amount was reduced by 84% in the following year.216 However, in 2021, the total funds released for the same purpose were Rs. 3,08,34,008/−.217 Parallel to this, the DBT released Rs. 7345.58 Lakh for projects related to stem cells and other areas of regenerative medicine.218 There appears to be no reason why the ICMR and the DBT need to fund stem cell research separately; such an unexplainable divide only fuels the ‘bureaucratic competition’, which was already pointed out by another scholar.219
Reportedly, in 2005, the DBT’s stem cell task force asked the government to set up special funds for facilitating research.220 This proposal for ‘priority fund’ was welcomed by several stakeholders, despite the fact that it did not materialize.221 There must be a well-defined model for funding, and there are several global best practices worth closer scrutiny.
The European Union’s (EU’s) ‘Horizon Europe’ is a pertinent model worth discussing. It is a funding program exclusively for scientific research for the period 2021–2027 & the ambit of the program includes stem cell research.222 There are also clear rules as to the funding of different types and categories of stem cell research. For example, funding is not available for research that involves creation of embryos for the sole purpose of stem cell procurement.223 Whether a research project is to be funded or not is decided based on multiple levels of ethical review.224
The establishment of such a mechanism with due emphasis on stem cell research can institutionalize the funding. Further, restricting funding based on compliance with the set standards can incentivize adherence to the soft law and the changing research norms that otherwise might be difficult to enforce through rigid hard laws. A just funding mechanism will also contribute toward democratizing stem cell–based clinical trials that are highly resource intensive and dominated by elite players.225 Ultimately, the question is not about investing more. Economists argue that every ‘Rupee’ of state spending costs the Indian taxpayers roughly three times.226 The utility of a funding strategy, hence, lies in reducing wastage and repetition while ensuring certainty.
IV.D. Empathetically Engaging with the Public
As hinted in the previous section on the special law, enacting a new legislation is just the first step in improving the situation. To address the deeper nuances of the issue, one has to see it from the patients’ and clinicians’ perspective as well. While the regulatory vacuum engendered the growth of clinics providing unproven therapies,227 the prevalence of stem cell therapies and the people’s trust in them have been entrenched by various social, political, and technical forces. As pointed out by Dr Rohini Kandhari in her ethnographic study, stem cell therapy has become part of the standard treatment in various ways through the process of ‘normalization’.228 Stem cell therapy being touted as the inevitable resort (for certain diseases), its promotion by even the established and trusted players, and the apparently ‘simple’ and ‘harmless’ procedure (in comparison with the proven surgical alternatives) have shaped the consumer choice and the integration of stem cell therapy into mainstream medical treatments.229
It can be safely posited that the appeal of unproven stem cell therapy with the consumers is mainly based on the information obtained from various personal sources,230 including that of social media.231 There are also studies that indicate that a large share of the population is unaware about the potential risks and side-effects of unproven therapies.232 The incomplete, misleading, and exaggerated information on which people base their decision is the elephant in the room that needs to be addressed. This also includes opinions of practitioners who might be informally approached and might have to advise such patients without much context or expertise.233
With the aim of bringing clarity to the stakeholders, the ICMR has released (jointly with the DBT) the NGSCR Guidelines and published the report titled ‘Evidence Based Status of Stem Cell Therapy for Human Diseases’.234 These documents, however, are out of a layperson’s reach. The NGSCR is a technical document and is meant for medical professionals engaged in stem cell research. On the other hand, though the report on the status of stem cell therapy was released keeping in mind the public and the patients, it has not received the due attention within the public.
India needs public education campaigns to address the ‘false hope’ on unproven therapies that patients nurture and clinics exploit. The objective of this sensitization drive shall be to remedy the distorted picture of stem cell therapies; it shall aim to convey to the public that the stem cell therapy suggested to them by professionals or close relatives can be just experimental, and not a standard treatment. Ultimately, the public must also be convinced to accept this reality over the rosy picture presented to them by some well-respected and established practitioners.235
Further, there must be an effective mode of communication and outreach—the above suggested outreach program can be implemented through advertisements and campaigns using social media platforms.236 The influence and authenticity of the well-known experts in the field can also be leveraged to convince the public. The information must be presented in an accessible form so that it is digestible to all sections of the society, including the marginalized groups. This is particularly important as there have been instances where people experiencing poverty have helplessly subjected themselves to clinical trials under the guise of free treatments or for monetary returns.237 As a preliminary measure, we can consider adopting the practice in Japan—where the Ministry of Health, Labour and Welfare publicly lists the clinics violating the law, thus not only providing prospective patients and other stakeholders with the information but also deterring the clinics from non-compliance.238 Ultimately, sensitization drives ought to go in tandem with the effective enforcement of the law that prohibits the promotion and advertisement of unproven therapies.
While the above steps may be beneficial in educating the patients and clearing the misconceptions and misperceptions around stem cell therapies, it only addresses one side of the issue and the limitations of such an ‘information-centric’ approach have already been pointed out by the literature.239 To realize the other side of the issue, one needs to understand the psychology of the patients. As posited by Dr Insoo Hyun, patients who exhaust the standard options may opt for (unproven) stem cell therapies just out of ‘therapeutic hope’—though it may not be rationally justifiable, they may still tend to delve on this option as a possible yet remote solution.240
In other words, public awareness campaigns alone may not be enough to prevent the unscrupulous clinics from exploiting the vulnerable patients. In fact, as Dr Hyun suggests, such public campaigns without any steps to improve the condition of such ailing patients may negatively affect their mentality.241 This is where the physicians need to pitch in. They need to informally and empathetically engage with the patients and provide the necessary emotional support to ameliorate their distress.242 This engagement can be facilitated by patient support organizations that have played an appreciable role in representing and supporting them. Carloyn Heitmeyer has previously cited the example of the Spinal Cord Consumers Group (SCCG) in India as a patient-activist group.243 The SCCG, as a community of ‘consumers’, helps the patients by lending emotional support and by educating the ‘consumers’ of the options available to them through collaboration with practitioners. Such a model not only protects patients, or rather consumers, from exploitative players, but also facilitates clinical trials by supporting patients who are willing to take part in experimental studies. The aim of such programs is to empathetically engage with the patients and not to merely classify them as vulnerable people. Further, civil society groups and patient support groups play an important role in supporting the patients, monetarily or otherwise, in pursuing their complaint before the consumer dispute for and the state medical councils.244
While Heitmeyer views this type of collaboration as an alternative to broader regulation by the state,245 I suggest that this can be placed well within the larger framework of formal regulations. That is, while state-led regulations can focus on the general function of combatting unscrupulous players, patient-led activist organizations can focus on the specific function of providing support and information to the patients and bringing them in level with the industry players. Hence, a robust patient-activist system should complement the public outreach measures to address the issue of exploitation of patients.246
V. CONCLUSION
India is a promising player in the global arena of stem cell research. If it is to contribute systematically into the field, then it is imminent that the regulatory framework is reformed. After analyzing the regulatory mechanism from the perspective of research, clinical trials, and therapy, it is evident that there is a need to rejig the current system for better regulatory clarity and effectiveness. The issues range from the inherent irony between restrictive guidelines and lax implementation, to the jurisdictional ambiguity and institutional overload. The ramifications of these issues are already before us in the form of misleading advertisements on stem cell therapy, proliferation of clinics without license, unethical unprofessionalism hidden under the unenforceability of guidelines, and an inequitable field for budding stem cell researchers.247 With the ambiguity in the regulatory framework, which even otherwise is brimming with hectic paper works, the current environment of stem cell research appears very intimidating for nascent players.248
It is in this context that the article throws light upon a few steps that can be taken to improve the Indian regulatory mechanism. One of the suggested measures is the introduction of a long-term funding strategy. Like the EU’s Horizon Europe, it can be a plan that covers funding of scientific research generally. However, India may also consider targeting more specific areas like regenerative medicine. In either of these cases, the plan must incentivize compliance with the guidelines and best practices, along with denying funds in instances of aberrations.
Enactment of the SCR Act is another suggestion. Clear expression of the rules in a consolidated format that gives mandates compliance to a specific list of standards and guidelines would go a long way in bringing the much-needed clarity and consistency in the legal system. Along with this, there is an imminent need to restructure the institutional framework—starting from a stem cell–specific regulatory division to better coordination between the central and state regulators, a functional set of institutions is critical to the uniform enforcement of laws. Equally important is the need to improve the capacity of our regulators. The CDSCO at the drug-regulatory level and the State MCs at the profession-regulatory level require greater manpower and resources and an institutional vision to properly deliver their functions. Further, the dispute resolution infrastructure, consisting of the civil and criminal courts and most importantly, consumer fora, must be strengthened to ensure that there are speedy adjudication and award of remedies.
The article also re-emphasizes the need for sensitizing the public and engaging with the patients through civil society groups and patient support groups. As mentioned before, the issue of people falling prey to unproven stem cell therapies is a cauldron of several socio-political factors. A robust regulatory framework may still fail when the public is uninformed and misdirected. From a long-term perspective, basic awareness measures might be insufficient. We need empathetic practitioners who can explain the therapeutic possibilities to a desperate patient for whom stem cell therapy might be a glimmer of hope. Hence, this process requires concerted efforts from a large number of players, from practitioners and public figures to State mechanisms. The caption that underlies all these reforms is that these are to be seen as integrated measures and not as isolated steps. The impact of these reforms is interconnected with each other. Hence, strategic implementation of the reforms is crucial to achieve the desired results.
Ultimately, this inquiry is timely. The ICMR-DBT Guidelines that are followed today are around eight years old. In the realm of science, specifically stem cell science, it is safe to adjudge it as outdated. Hence, the policy-makers must evaluate the existing scenario and ensure that imminent reforms, as suggested in this article, are taken into consideration.