Interventional Radiology for Delayed Post-Pancreatectomy Hemorrhage: A Case Report and Review of the Literature
Ruchika Patra, Sidra Baig, Dakshin Meenashi Sundaram, Riten Bhadreshkumar Patel, Anushka Mehta, Uzoh Chidimma Judith, Pooja Patel, Sajjal Mahmood, Harshini Malisetty, Prachi Dawer

TL;DR
This case report describes a fatal delayed post-pancreatectomy hemorrhage managed with interventional radiology, emphasizing the importance of early recognition and multidisciplinary care.
Contribution
The paper presents a rare case of delayed PPH treated with embolization, highlighting the role of interventional radiology in managing this complication.
Findings
Sentinel bleeding was an early sign of catastrophic delayed PPH.
Transcatheter arterial embolization achieved immediate angiographic success but could not prevent mortality.
Interventional radiology offers a less invasive alternative to reoperation for managing PPH.
Abstract
Post-pancreatectomy hemorrhage (PPH) is a life-threatening complication of pancreatic surgery associated with high mortality. The International Study Group of Pancreatic Surgery (ISGPS) classifies PPH as early (<24 hours) or delayed (>24 hours), with delayed hemorrhage often resulting from vascular erosion, pseudoaneurysm formation, or anastomotic ulceration. We report a case of a 52-year-old male who underwent a classical pancreaticoduodenectomy (Whipple’s procedure) for periampullary adenocarcinoma. The early postoperative course was uneventful until postoperative day (POD) 6, when the patient developed a sentinel bleed, presenting as hematemesis and melena, followed approximately two hours later by hemodynamic instability (BP 80/50 mmHg). Laboratory evaluation revealed a sharp drop in hemoglobin from 11.2 g/dL to 6.4 g/dL, with normal coagulation parameters. Emergency digital…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
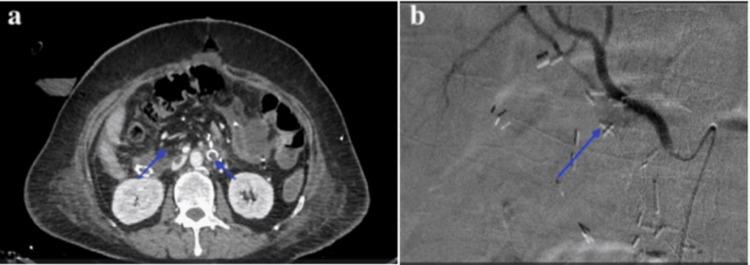 Figure 1
Figure 1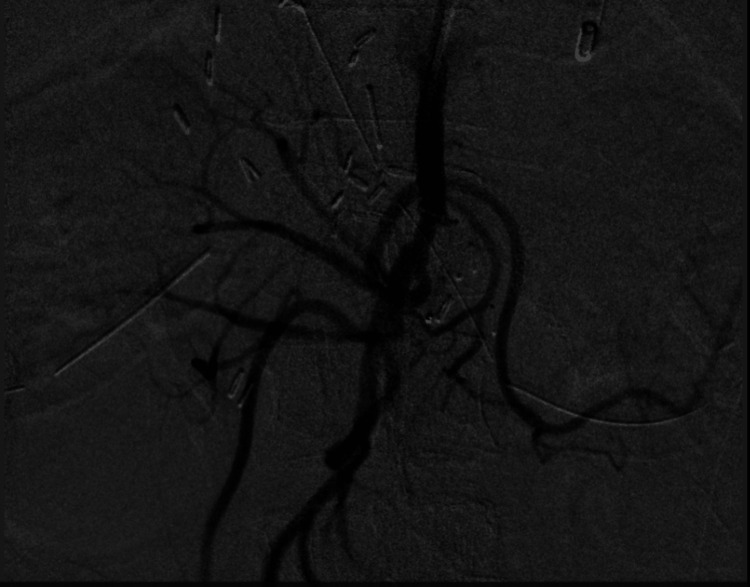 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Pancreatitis Pathology and Treatment · Renal cell carcinoma treatment
Introduction
Complications following pancreatic surgery, such as anastomotic leak, postoperative pancreatic fistula formation, hemorrhage, and delayed gastric emptying, remain major causes of postoperative morbidity and mortality. Among these, hemorrhage is particularly perilous, with reported mortality rates reaching up to 40-50% [1]. The International Study Group of Pancreatic Surgery (ISGPS) classifies post-pancreatectomy hemorrhage (PPH) into early (<24 hours, acute) and delayed (>24 hours, chronic) types, based on the timing of onset after surgery [1]. While early hemorrhage is usually attributed to technical factors or inadequate intraoperative hemostasis and often requires surgical re-exploration, delayed hemorrhage generally occurs due to vascular erosion secondary to intra-abdominal sepsis, pancreatic or biliary fistula, anastomotic ulceration, or the formation of an arterial pseudoaneurysm [2,3]. Common arterial sites prone to delayed PPH include the gastroduodenal artery stump (up to 60%), common hepatic artery (approximately 20-25%), splenic artery (10-15%), and superior mesenteric artery branches (less than 5%) [4,5]. With a mortality rate approaching 50%, delayed PPH remains one of the most severe and life-threatening complications following pancreaticoduodenectomy or distal pancreatectomy. In recent years, interventional radiology has emerged as a first-line, minimally invasive, and organ-preserving approach in the multidisciplinary management of delayed hemorrhage, reducing the need for high-risk surgical re-exploration and improving overall survival outcomes.
Case presentation
A 52-year-old male with a known history of type 2 diabetes mellitus and hypertension, well controlled on oral medications, presented with painless progressive jaundice, pruritus, and weight loss of two months’ duration. Contrast-enhanced computed tomography (CECT) of the abdomen revealed a periampullary mass measuring 2.8 × 2.3 cm without vascular invasion or distant metastasis. Endoscopic biopsy confirmed periampullary adenocarcinoma. The patient subsequently underwent a classical pancreaticoduodenectomy (Whipple’s procedure) with duct-to-mucosa pancreaticojejunostomy, hepaticojejunostomy, and gastrojejunostomy reconstruction.
The surgery was uneventful, and the patient was managed postoperatively in the ICU for 48 hours before transfer to the surgical ward. The patient received standard postoperative care, including broad-spectrum antibiotics, thromboprophylaxis, glycemic control, and early enteral nutrition. The surgical drain initially yielded 80-100 mL of serous fluid daily. Drain fluid amylase on postoperative day (POD) 3 was 45 IU/L, not suggestive of a pancreatic fistula. No intra-abdominal collections were detected on ultrasound.
On POD 6, the patient experienced two episodes of hematemesis and passage of melena, followed by hypotension (BP 80/50 mmHg) and tachycardia (heart rate (HR) 120 bpm) within two hours of the initial bleed. Given the hemodynamic deterioration, this was considered a major GI hemorrhage, not a classical sentinel bleed, which is typically minor and self-limiting. The drain output on the same day became altered and blood-stained (approximately 250 mL) compared to previous serous output. Laboratory results showed a decline in hemoglobin from 12.1 g/dL preoperatively to 10.8 g/dL on POD 1, and to 6.4 g/dL on POD 6, while the coagulation profile and platelet count were within normal limits.
The patient was shifted to the ICU and received two units of packed red blood cells and one unit of fresh frozen plasma. Emergency CECT angiography demonstrated a pseudoaneurysm arising from the stump of the gastroduodenal artery (GDA) with active contrast extravasation into the peripancreatic region (Figure 1a). Right common femoral artery access was obtained, and selective celiac and common hepatic artery angiography confirmed the pseudoaneurysm at the GDA stump (Figure 1b). Super-selective catheterization was performed using a 2.7 Fr microcatheter, and the pseudoaneurysm was embolized with platinum microcoils (2 mm × 6 cm) and polyvinyl alcohol (PVA) particles (300-500 μm).
(a) Axial contrast-enhanced CT image showing a pseudoaneurysm (yellow arrow) near the gastroduodenal artery stump with contrast extravasation. (b) Digital subtraction angiography (DSA) image confirming active contrast extravasation from the GDA stump pseudoaneurysm.
Post-embolization angiography demonstrated complete occlusion of the pseudoaneurysm with no residual contrast extravasation (Figure 2). Following embolization, the patient continued to receive vasopressor and ventilatory support in the ICU. Despite aggressive transfusion (a total of 4 units of packed red blood cells, 2 units of fresh frozen plasma, and 1 unit of platelets) and fluid resuscitation, the patient’s hemodynamic instability persisted. Repeat CECT 12 hours later showed no active bleeding or new collections. Given his critical condition, ongoing shock, and poor physiological reserve, re-exploratory surgery was deferred after multidisciplinary discussion. The patient unfortunately succumbed within 24 hours of embolization due to massive hemorrhage-related multi-organ failure.
Post-embolization angiogram showing successful occlusion of the bleeding vessel with coils and no further evidence of contrast extravasation.
Final histopathology confirmed moderately differentiated periampullary adenocarcinoma (pT2N1M0) with negative resection margins. There was no evidence of pancreaticojejunostomy leak or intra-abdominal sepsis before the bleeding event.
This case illustrates the catastrophic nature of delayed PPH, emphasizing that not all postoperative bleeds labeled as “sentinel” are minor. Prompt imaging, early angiography, and endovascular intervention remain critical to management. However, the prognosis remains guarded when massive hemorrhage and systemic instability coexist, even after technically successful embolization.
Discussion
PPH is a major surgical complication associated with considerable mortality and morbidity, particularly in its delayed form (DPH). Although uncommon, delayed PPH remains one of the leading causes of late postoperative deaths following pancreatic resections such as pancreaticoduodenectomy (Whipple’s procedure) and distal pancreatectomy. Recent single-center and multi-institutional studies report mortality rates of up to 40-50%, underscoring its clinical gravity [6,7].
In our case, a 52-year-old male (height 172 cm, weight 74 kg, BMI 25.0 kg/m²) developed a single episode of massive delayed hemorrhage on postoperative day 6, which was promptly managed with emergency endovascular embolization. There was no recurrent bleeding episode prior to the patient’s demise. Hence, the earlier mention of “recurrent” or “sequential” interventional procedures has been corrected to reflect the true course, a single angiography and embolization performed immediately after the bleed.
In contemporary practice, contrast-enhanced CT angiography (CECT-A) is recommended as the first-line diagnostic test in cases of sentinel or overt bleeding following pancreatic surgery, as it helps localize the site and etiology of bleeding with high sensitivity [8]. Catheter angiography is then used for definitive diagnosis and therapeutic intervention. In our case, CECT demonstrated a pseudoaneurysm of the GDA stump, confirmed by digital subtraction angiography (DSA), which was successfully treated with coil embolization.
The GDA stump remains the most common bleeding source (approximately 60% of cases), followed by the common hepatic artery, splenic artery, and superior mesenteric artery branches [9]. The etiology in delayed PPH often involves vascular erosion secondary to pancreatic fistula or intra-abdominal infection; however, in this case, there was no biochemical or imaging evidence of pancreaticojejunostomy leak or abscess formation. The drain output, which had previously been serous (80-100 mL/day), became altered and blood-stained on the day of the bleed,indicating secondary hemorrhagic contamination rather than persistent leakage.
Transcatheter arterial embolization (TAE) using coils, particles, or liquid embolics is now widely accepted as the first-line treatment for delayed PPH, achieving technical success rates exceeding 80% in several series [10-12]. However, mortality remains high due to the patient’s unstable physiological status and associated complications rather than failure of the procedure itself. Covered stent (stent-graft) placement may be considered in selected cases involving major vessels, such as the common hepatic artery, particularly when maintaining arterial perfusion is crucial [13,14].
A multidisciplinary hemorrhage team typically includes hepatopancreatobiliary (HPB) surgeons, interventional radiologists, anesthesiologists, and critical care specialists. Such coordinated teams enable rapid decision-making, expedite transfer for imaging or intervention, and optimize patient resuscitation and monitoring. Early activation of this team is now considered a best-practice model in high-volume pancreatic centers [15].
Our case reinforces several key lessons: (1) delayed PPH, although rare, can be catastrophic and may present abruptly without prior warning; (2) prompt CT angiography followed by timely endovascular management remains the cornerstone of diagnosis and treatment; and (3) despite technically successful embolization, patient outcome is highly dependent on pre-existing comorbidities, physiological reserve, and timing of intervention. Early recognition and a coordinated, multidisciplinary approach remain essential to improving survival in this life-threatening condition.
Conclusions
DPH is a rare but devastating complication, carrying high morbidity and mortality even with modern perioperative care. Our case underscores the critical importance of recognizing sentinel bleeding as an early warning sign, warranting urgent angiographic evaluation and interventional radiology (IR)-guided embolization. IR offers a minimally invasive and effective alternative to high-risk surgical re-exploration, with the dual advantage of diagnosis and therapy. However, outcomes remain poor when complicating factors such as pancreatic leak, infection, or sepsis are present, as these significantly increase the likelihood of rebleeding despite technically successful embolization.
This highlights the necessity of close postoperative surveillance, rapid referral, and a coordinated multidisciplinary approach involving surgeons, interventional radiologists, and intensive care specialists. Looking ahead, standardizing treatment protocols, developing rapid-response hemorrhage teams, and refining endovascular strategies, such as covered stent-graft placement, may further improve outcomes. Vigilance, early recognition, and timely intervention remain the cornerstone of DPH management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A systematic review of post-pancreatectomy haemorrhage management stratified according to ISGPS grading HPB (Oxford) Maccabe TA Robertson HF Skipworth J Rees J Roberts K Pathak S 111011182420223510135910.1016/j.hpb.2021.12.002 · doi ↗ · pubmed ↗
- 2Late complication in patients undergoing pancreatic resection with intraoperative radiation therapy: gastrointestinal bleeding with occlusion of the portal system J Gastroenterol Hepatol Shimizu Y Yasui K Fuwa N Arai Y Yamao K 123512402020051604857210.1111/j.1440-1746.2005.03913.x · doi ↗ · pubmed ↗
- 3Management of bleeding and leakage after pancreatic surgery Best Pract Res Clin Gastroenterol de Castro SM Busch OR Gouma DJ 8478641820041549428210.1016/j.bpg.2004.06.001 · doi ↗ · pubmed ↗
- 4Evaluation of the International Study Group of Pancreatic Surgery definition of post-pancreatectomy hemorrhage in a high-volume center Surgery Grützmann R Rückert F Hippe-Davies N Distler M Saeger HD 61262015120122208881910.1016/j.surg.2011.09.039 · doi ↗ · pubmed ↗
- 5Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections Ann Surg Yekebas EF Wolfram L Cataldegirmen G 26928024620071766750610.1097/01.sla.0000262953.77735.db PMC 1933568 · doi ↗ · pubmed ↗
- 6Diagnosis and management of postpancreatectomy hemorrhage: a single-center experience of consecutive 1,096 pancreatoduodenectomies Pancreatology Kobayashi K Inoue Y Omiya K 2352442320233676487410.1016/j.pan.2023.01.004 · doi ↗ · pubmed ↗
- 7Hemorrhage sites and mitigation strategies after pancreaticoduodenectomy JAMA Surg Preston WA Collins ML Gönen M 89189915920243877607610.1001/jamasurg.2024.1228 PMC 11112495 · doi ↗ · pubmed ↗
- 8Efficacy and safety of endovascular therapy for delayed hepatic artery post-pancreatectomy hemorrhage: development of extrahepatic collateral circulation and complications of post endovascular therapy CVIR Endovasc Nozawa Y Ymazoe S Masuda K 47520223606325210.1186/s 42155-022-00326-x PMC 9445144 · doi ↗ · pubmed ↗