True Digital Artery Aneurysm: A Case Report
Hiroki Nakabori, Hideyasu Ueda, Kenji Iino

TL;DR
A rare case of a true aneurysm in a finger artery was successfully treated with surgery, showing good recovery and no complications.
Contribution
This case report adds to the limited literature on true digital artery aneurysms and highlights effective treatment with ligation and excision.
Findings
A 7-mm true aneurysm in the digital artery was successfully excised with ligation.
Postoperative recovery was uneventful with no recurrence after one year.
Sufficient collateral circulation allowed for effective treatment without complications.
Abstract
True aneurysms of the digital artery are extremely rare, and only several dozen cases have been reported worldwide. A 29-year-old man presented with a pulsatile, tender nodule in his left index finger. Angiography revealed a 7-mm saccular aneurysm of the proper palmar digital artery with well-developed distal collaterals. Under local anesthesia, the aneurysm was excised following proximal and distal ligation. It was histopathologically confirmed as a true aneurysm. Postoperatively, symptoms resolved without ischemic or neurological complications and without recurrence after 1 year. Thus, simple ligation and excision are effective when collateral circulation is sufficient.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
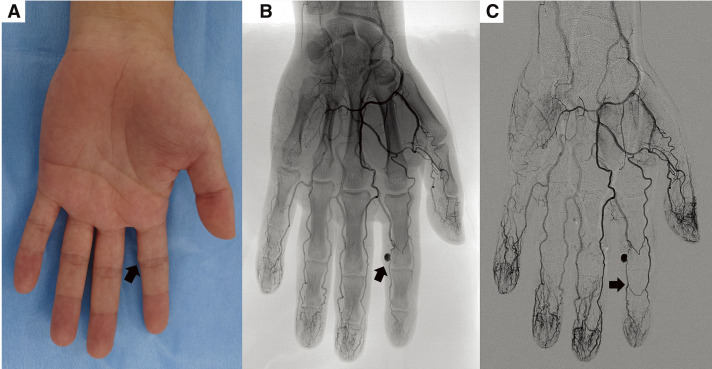 Fig. 1
Fig. 1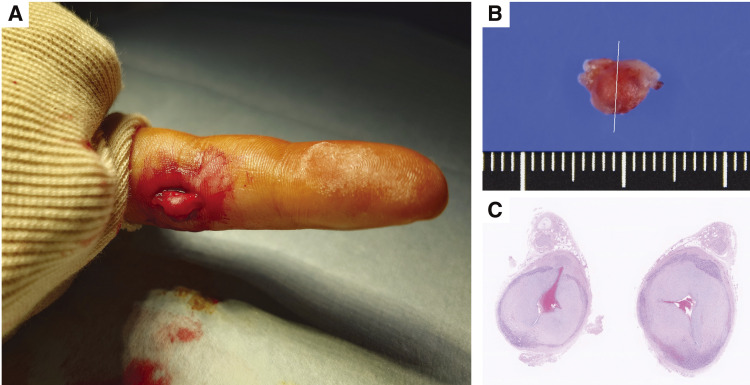 Fig. 2
Fig. 2| Author | Year | Age | Gender | Type | Symptoms | Imaging | Injury | Location | Surgical indications | Repair | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Berrettoni | 1990 | 67 | M | Mycotic | Painful mass, swelling, 1-week history | US | Infective endocarditis | Index finger | Relieve the pain | E + reconstruction with arterial graft | No sequelae |
| Bouvet | 2018 | 39 | M | Mycotic | Painful mass | MRI | Previous penetrating trauma and an infected collection | Thumb | Relieve the pain | E + PA | No sequelae |
| Baruch | 1977 | 21 | M | False | Painful mass, hard | X-ray | Glass laceration | Thumb | Relieve the pain | E + L | NR |
| Hentz | 1978 | 19 | M | False | Painful mass, pulsatile mass, following partial amputation of the right index finger | No imaging | Digital amputation | Middle finger | Relieve the pain | E + L + complete amputation of digital stump | No sequelae |
| Suzuki | 1980 | 69 | M | False | Motion limitation, hypoesthesia, ischemic skin changes | Angiography | Machinist, penetrating injury | Thumb | Improve motion limitation | E + L | No sequelae |
| Sanchez | 1982 | 26 | M | False | Tender, pulsatile mass | Angiography | Penetrating injury | Ring finger | Relieve the tenderness | E + PA | No sequelae |
| Hall | 1986 | 24 | M | False | Painful mass, throbbing, 5 days post-injury | Angiography | Penetrating injury | Little finger | Relieve the pain | Repair | No sequelae |
| Gracia | 1987 | 70 | M | False | Numbness, pulsatile mass, 3 weeks following a knife injury | NR | Penetrating injury | Middle finger | Improve numbness | E + L | No sequelae |
| Ho | 1987 | NR | NR | False | NR | NR | Puncture wound | Thumb | NR | E + L | No sequelae |
| Ho | 1987 | NR | NR | False | NR | NR | Penetrating injury | Little finger | NR | E + L | No sequelae |
| Tyler | 1988 | 57 | F | False | Painful, pulsatile mass, median nerve compression, intermittent cyanosis | Angiography | Opened tins by banging the palm of her hand on the opener for several years | First CPDA | Relieve the pain | E + vein graft | No sequelae |
| Brunelli | 1988 | 27 | M | False | Tender, non-pulsatile mass | X-ray | Crush injury | Middle and ring finger | Relieve the tenderness | E + reconstruction with IVG | No sequelae |
| Montoya | 1991 | 23 | M | False | Painful, pulsatile mass, hypoesthesia, cyanotic, 18 days post-injury | No imaging | Manual worker, penetrating injury | Little finger | Relieve the pain | E + L | No sequelae |
| Shidayama | 1992 | 13 | F | False | Tender, pulsatile mass, 1-week post-injury | No imaging | Penetrating injury | Middle finger | Relieve the tenderness | E + L | No sequelae |
| Bianchi | 1993 | 70 | M | False | Non-pulsatile mass, gradually enlarging for 15 years following penetrating trauma | Angiography | Penetrating injury | Middle finger | NR | E + L | NR |
| Yajima | 1995 | 58 | F | False | Painful, pulsatile`mass | No imaging | Cut | CPDA | Relieve the pain | E + PA | No sequelae |
| Yasuda | 1996 | NR | M | False | NR | US | Softball catcher | Thumb | NR | NR | NR |
| Cromheecke | 1997 | 69 | M | False | Tender, pulsatile mass | Angiography | Screwdriver injury | Second CPDA | Relieve the tenderness | Conservative | No sequelae |
| Abouzahr | 1997 | 6 | M | False | Tender, pulsatile mass, violaceous, 10 days post-injury | MRA | Penetrating injury | Index finger | Relieve the tenderness | E + L | No sequelae |
| Simeonov | 1998 | 4 | M | False | Enlarging mass, bleeding | No imaging | Penetrating injury | Second CPDA | Rupture | E + L | NR |
| Khan | 1998 | 70 | M | False | Tender mass, swelling | No imaging | Penetrating injury | Middle finger | Relieve the tenderness | E + L | No sequelae |
| Ballas | 2006 | 40 | M | False | Non-pulsatile mass, fixed | MRA | Textile factory worker, hammer injury, partial factor 8 deficiency | Index finger | NR | E + L | No sequelae |
| Miyamoto | 2009 | 16 | M | False | Tender, enlarging mass, hypoesthesia, 1-year history | MRA | Baseball player | Thumb | Relieve the tenderness | E + PA | No sequelae |
| Lucchina | 2011 | 43 | M | False | Painful mass, 6 weeks post-injury | CTA | Scissor injury | First CPDA | Relieve the pain | E + reconstruction with superficial palmar branch of the radial artery | No sequelae |
| Chaudhry | 2011 | 54 | F | False | Tender, pulsatile mass, firm | US | Dog bite | Index finger | Relieve the tenderness | E + L | No sequelae |
| Plant | 2011 | 65 | F | False | Tender, non-pulsatile mass, fixed | US + angiogram | Penetrating injury | Thumb | Relieve the tenderness | E + PA | No sequelae |
| Taylor | 2012 | 60 | M | False | Painful, pulsatile mass, enlarging, reduced sensation in the radial nerve distribution of the thumb | MRA | Percutaneous trigger finger release | Thumb | Relieve the pain | E + L | No sequelae |
| Sayit | 2017 | 27 | M | False | Tender, pulsatile mass, hypoesthesia, skin atrophy, 1-month post-injury | MRI | Penetrating injury | First CPDA | Relieve the tenderness | E + PA | NR |
| Zhang | 2023 | 74 | F | False | Painful, pulsatile mass, 2 weeks post-injury | X-ray | Sharp incision injury | Index finger | Relieve the pain | E + L | No sequelae |
| Yamashiro | 2023 | 28 | M | False | Tender, non-pulsatile mass | US + MRI | Blunt trauma | Middle finger | Relieve the tenderness | E + L | No sequelae |
| Dukan | 2023 | 36 | M | False | Hypoesthesia, non-pulsatile mass | US | Sharp incision injury | Index finger | Improve hypoesthesia | E + L | No sequelae |
| Layman | 1982 | 38 | M | True | Tender mass, hypoesthesia, 2 years following injury | No imaging | Crush injury | Middle finger | Relieve the tenderness | E + L | NR |
| Dangles | 1984 | 46 | M | True | Painful mass | No imaging | US Navy officer, bowler | Thumb | Relieve the pain | E + L | NR |
| Turner | 1984 | 52 | F | True | Tender mass, hypoesthesia | No imaging | Canteen assistant | Ring finger | Relieve the tenderness | E + L | Complete pain relief, residual hypoesthesia |
| Ho | 1987 | NR | NR | True | NR | NR | Unknown | Index finger | NR | E + L | No sequelae |
| Ho | 1987 | NR | NR | True | NR | NR | Unknown | Little finger | NR | E + L | No sequelae |
| Ho | 1987 | NR | NR | True | NR | NR | Unknown | Index finger | NR | E + L | No sequelae |
| Ho | 1987 | NR | NR | True | NR | NR | Volleyball player | Ring finger | NR | E + PA | No sequelae |
| Trabulsy | 1992 | 21 | F | True | Painful, non-pulsatile mass, loss of sensation, reduced 2-point discrimination | No imaging | Telephone operator | Index finger | Relieve the pain | E + L | No sequelae + regained 2-point discrimination |
| Lanzetta | 1992 | 28 | F | True | Tender, pulsatile mass, digit 3 degrees cooler than the opposite hand | Angiography | Volleyball player | Middle finger (x3) + superficial palmar arch | Relieve the tenderness | Conservative | No sequelae |
| Itoh | 1992 | 8 month | M | True | Pulsatile mass, 1-month history of enlarging | US | Congenital | Third CPDA | NR | E + L | No sequelae |
| Adant | 1994 | 55 | M | True | Severe pain and numbness when trying to grasp objects, present for 1.5 years | No imaging | Metal worker, hemophilia | Thumb | Relieve the pain | E + L | No sequelae |
| Yajima | 1995 | 69 | F | True | Hypoesthesia, non-pulsatile mass | No imaging | Farming | CPDA | Improve hypoesthesia | E + L | No sequelae |
| Yajima | 1995 | 16 | M | True | Hypoesthesia, non-pulsatile mass | No imaging | Baseball | Thumb | Improve hypoesthesia | E + L | No sequelae |
| Yoshii | 2000 | 29 | M | True | Tender, non-pulsatile mass, numbness on ulnar side of finger | MRI | Golfer | Ring finger | Relieve the tenderness | E + L | No sequelae |
| Taniguchi | 2002 | 47 | M | True | Tender mass | No imaging | Radiographer | Thumb | Relieve the tenderness | E + L | No sequelae |
| Strauch | 2004 | 32 | F | True | Tender, pulsatile mass, blue swelling | Angiography | No cause identified | Little finger | Relieve the tenderness | E + reconstruction with IVG | No sequelae |
| Tanaka | 2005 | 2 | F | True | Pulsatile mass, swelling | Angiography | Congenital | Middle finger | NR | E + reconstruction with IVG | No sequelae |
| Lee | 2006 | 44 | F | True | Tender, non-pulsatile mass | No imaging | Poor fitting wedding ring | Ring finger | Relieve the tenderness | E + L | No sequelae |
| Quintella | 2019 | 60 | M | True | Tender, pulsatile mass | MRA | No cause identified | Middle finger | Relieve the tenderness | E + L | No sequelae |
| Dean | 2019 | 13 month | M | True | Enlarging, pulsatile mass | Angiography | Congenital | Second CPDA | NR | E + L | No sequelae |
| Vinnicombe | 2019 | 44 | M | True | Swelling | MRA | Musician, golfer | Second CPDA | NR | E + L | No sequelae |
| Sheikh | 2020 | 64 | M | True | Pulsatile mass | US + angiography | Electrician | Fourth CPDA | Prevention of thrombosis or rupture | E + PA | No sequelae |
| Likhitha | 2023 | 22 | F | True | Tender, pulsatile mass | MRA | No cause identified | Little finger | Relieve the tenderness | E + L | No sequelae |
| Gunawardena | 2025 | 77 | F | True | Tender, pulsatile mass | US + CTA | No cause identified | First CPDA | Relieve the tenderness | E + PA | No sequelae |
| Nakabori | 2025 | 29 | M | True | Tender, pulsatile mass | US + angiography | No cause identified | Index finger | Relieve the tenderness | E + L | No sequelae |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Aortic aneurysm repair treatments · Intracranial Aneurysms: Treatment and Complications
Introduction
Peripheral arterial aneurysms are rare and even rarer in the upper extremity than in the lower extremity, accounting for <1% of all peripheral aneurysms.^1)^ Among these aneurysms, digital artery aneurysms are exceedingly rare, with only several dozen cases reported globally. Here, we present a case of a true digital artery aneurysm in a young adult.
Case Report
A 29-year-old man presented with discomfort and tenderness in his left index finger. Approximately 1 month earlier, he had noticed a mildly tender, pulsatile nodule at the proximal interphalangeal joint and consulted a local physician (Fig. 1A). Ultrasonography revealed a structure continuous with the artery, suggestive of an aneurysm, and he was referred to our department. He worked as a freight train operator and was right-handed, with no history of trauma, comorbidities, surgery, or medication use. He denied recurrent irritation of the affected finger. Angiography revealed a 7-mm saccular aneurysm in the proper palmar digital artery at the distal end of the proximal phalanx of his left index finger. No arteriovenous fistula was present, and the distal collateral circulation was well developed (Figs. 1B and 1C). He was diagnosed with a true digital artery aneurysm and opted for surgery. Under local anesthesia, a 3-cm incision was made over the aneurysm, which was then exposed (Fig. 2A). Before transection, the inflow and outflow arteries were isolated and doubly ligated with 3-0 silk sutures, and the aneurysm was then resected (Fig. 2B).
Preoperative photograph and angiography of the left hand. (A) A 7-mm pulsatile mass (arrow) on the ulnar side of the left index finger at the proximal interphalangeal joint. The lesion was elastic, mobile, and mildly tender. (B) Angiogram showing a 7-mm saccular aneurysm of the proper palmar digital artery at the distal portion of the proximal phalanx (arrow), without arteriovenous fistula. (C) Digital subtraction angiogram revealing a well-developed collateral circulation distal to the aneurysm (arrow).
Intraoperative and pathological photographs. (A) Intraoperative view showing dissection of the aneurysm with isolation of the inflow and outflow arteries. (B) Resected specimen measuring 8 × 6 × 4 mm. (C) Histopathological examination showing marked intimal thickening, consistent with a true aneurysm.
Histopathological examination revealed marked intimal thickening with disruption of the internal and external elastic laminae of the aneurysmal wall. The adventitia showed histiocytic and lymphocytic infiltration with neovascularization, consistent with reactive change. No malignant features were observed, confirming a true aneurysm (Fig. 2C). Discomfort and tenderness resolved completely after surgery. No ischemic or neurological complications occurred, and the patient remained recurrence-free at 1 year.
Discussion
Peripheral arterial aneurysms are very rare, with upper extremity lesions accounting for <1% of all cases,^1)^ and digital artery aneurysms are even rarer. In a systematic review of MEDLINE and Embase, Sheikh et al. identified 21 true aneurysms, 26 pseudoaneurysms, and 2 mycotic aneurysms.^2)^ We subsequently performed a MEDLINE search of reports published thereafter and identified an additional 7 cases. As of 2025, there are 25 reported cases of true aneurysm, 29 pseudoaneurysms, and 2 mycotic aneurysms. These cases were incorporated into an updated comparative summary (Table 1).^2–10)^ True aneurysms most often presented with compressive symptoms, while pseudoaneurysms were more frequently associated with ischemia and embolic complications. As shown in Table 1,^2–10)^ the presenting symptoms of true aneurysms included severe pain (2/25, 8.0%), tenderness (11/25, 44.0%), and hypoesthesia (4/25, 16.0%), whereas pseudoaneurysms most often presented with severe pain (9/29, 31.0%), tenderness (11/29, 37.9%), and hypoesthesia (5/29, 17.2%), suggesting a stronger association with ischemic or embolic events. In the present case, the patient’s chief complaints of mild tenderness and a pulsatile mass were more indicative of a true aneurysm. True aneurysms are most often attributed to chronic mechanical irritation or blunt trauma, often of occupational origin (e.g., metalwork, radiography, and golfing). Other causes include congenital anomalies, inflammatory disorders, atherosclerosis, and idiopathic factors.^2,3,8)^ Digital artery aneurysms may mimic epidermoid cysts, arteriovenous fistulas, foreign-body granulomas, ganglion cysts, or schwannomas, and intraoperative diagnosis is not unusual.^9)^ Bouvet et al. proposed a diagnostic algorithm for hand aneurysms and recommended ultrasonography for palpable lesions, angiography for acute ischemia, and computed tomography or magnetic resonance angiography in the absence of ischemic signs.^10)^ No cases of rupture have been reported, and no consensus on treatment indications has been established. However, in digital artery aneurysms, it is often difficult to distinguish between true and pseudoaneurysms preoperatively. Because pseudoaneurysms carry a higher risk of ischemia, excision is frequently chosen for both symptom relief (pain, numbness, pulsatile mass, cold sensation, cyanosis) and diagnostic confirmation. Treatment options include ligation and excision alone, excision with primary repair, or reconstruction using vein or arterial grafts. When the collateral circulation is sufficient, simple excision with ligation is generally adequate; however, preoperative imaging or digital Allen’s test should be conducted to confirm collateral development.^2,3,8)^ When the collateral circulation is insufficient, treatment options include conservative management, simple ligation and excision with the risk of ischemic complications or even amputation, or technically demanding microvascular reconstruction. Although conservative management has rarely been reported, surgical treatment is generally considered the realistic option. In such cases, thorough preparation is necessary, including consultation with a plastic surgeon experienced in microvascular reconstruction. In this case, angiography confirmed the adequacy of the collateral circulation, allowing successful resection with simple ligation. The patient’s symptoms resolved, and no recurrence was observed at 1 year.
Conclusion
We encountered a rare case of a true digital artery aneurysm. In cases where the collateral circulation is sufficient, simple ligation and excision are safe and effective.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shaban Y, Elkbuli A, Geraghty F, et al. True brachial artery aneurysm: a case report and review of literature. Ann Med Surg (Lond) 2020; 56: 23–7.32577227 10.1016/j.amsu.2020.06.011PMC 7300230 · doi ↗ · pubmed ↗
- 2Sheikh Z, Selvakumar S, Goon P. True aneurysm of the digital artery: a case report and systematic literature review. J Surg Case Rep 2020; 2020: rjz 400.32104566 10.1093/jscr/rjz 400PMC 7033485 · doi ↗ · pubmed ↗
- 3Likhitha Reddy C. True digital artery aneurysm - a clinical vignette. World J Plast Surg 2023; 12: 72–4.37220586 10.52547/wjps.12.1.72PMC 10200081 · doi ↗ · pubmed ↗
- 4Zhang L, Coutinho M. A case of digital pseudoaneurysm following sharp injury to a digit. Eplasty 2023; 23: e 2.36741349 PMC 9869392 · pubmed ↗
- 5Yamashiro T, Hachisu Y, Azuma R. Mixed lesion of traumatic pseudoaneurysm and pyogenic granuloma on a digit. Case Reports Plast Surg Hand Surg 2023; 10: 2228887.37397126 10.1080/23320885.2023.2228887 PMC 10312018 · doi ↗ · pubmed ↗
- 6Dukan R, Lacroix M, Bertin E, et al. Acute digit ischemia due to a ruptured digital collateral artery aneurysm in a patient of hemophilia: a case report. J Orthop Case Rep 2023; 13: 70–4.10.13107/jocr.2023.v 13.i 11.4010 PMC 1066423238025357 · doi ↗ · pubmed ↗
- 7Gunawardena T. Spontaneous aneurysm of a common digital artery: a rare entity. J Vasc Bras 2025; 24: e 20240083.39981419 10.1590/1677-5449.202400832 PMC 11841619 · doi ↗ · pubmed ↗
- 8Vinnicombe Z, Little M, Nicola A, et al. A rare case of digital artery aneurysm. JPRAS Open 2019; 20: 87–91.32158875 10.1016/j.jpra.2019.03.002PMC 7061589 · doi ↗ · pubmed ↗