Usefulness of Four-Point Dermal-Injection Lymphatic Scintigraphy for Lower-Limb Lymphedema
Yoshiyuki Kitamura, Takuro Isoda, Sando Motohiro, Masaoki Kusunoki, Hideki Kadota, Shingo Baba, Kousei Ishigami

TL;DR
This study shows that a four-point injection method for lymphatic imaging is effective in assessing the severity of lower-limb lymphedema.
Contribution
The study introduces and validates a four-point dermal-injection lymphatic scintigraphy method for evaluating lower-limb lymphedema.
Findings
The absence of certain lymphatic vessel regions and dermal backflow correlates with lymphedema severity.
The number of depicted lymphatic vessels and dermal backflow appearance can distinguish moderate from severe lymphedema.
LyS4 demonstrated high diagnostic accuracy for specific lymphatic vessel appearances.
Abstract
Objective: Lymphatic scintigraphy using radioisotope agents is a good method for evaluating the lymph flow status of patients with lower-limb lymphedema. To depict wide regions of lower-limb lymphatic vessels, at our institution, we administer radioisotopes at four locations in each limb when lymphatic scintigraphy images are to be obtained. Herein, we evaluated the correlation of lymphatic scintigraphy with lymphedema staging and investigated the usefulness of this four-point dermal-injection lymphatic scintigraphy (LyS4). Materials and methods: The 52 lower limbs of 26 patients (23 females, three males, aged 20-85 years, median 65 years) underwent a LyS4 examination of their lower limbs. The stage of lower-limb lymphedema was diagnosed by plastic surgeons at our institution using the International Society of Lymphology (ISL) staging system. The patients' ISL stages were stage 0…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1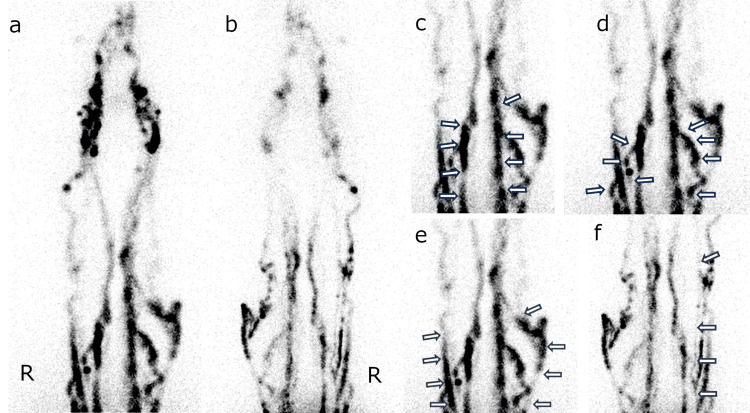 Figure 2
Figure 2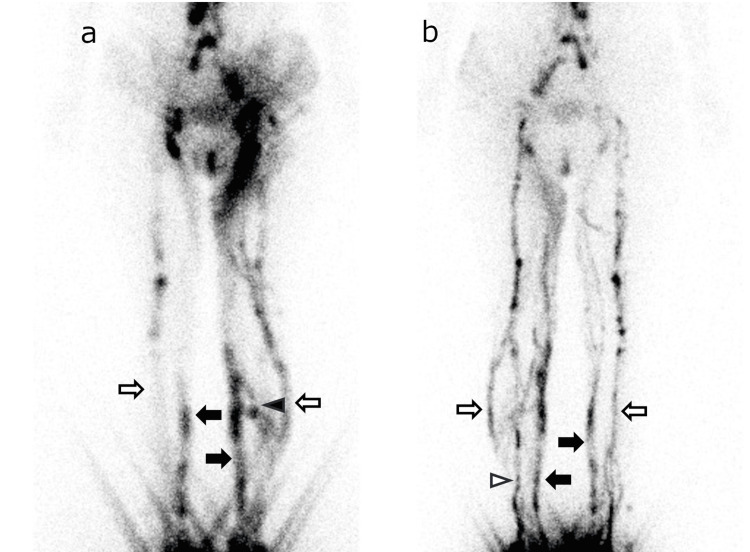 Figure 3
Figure 3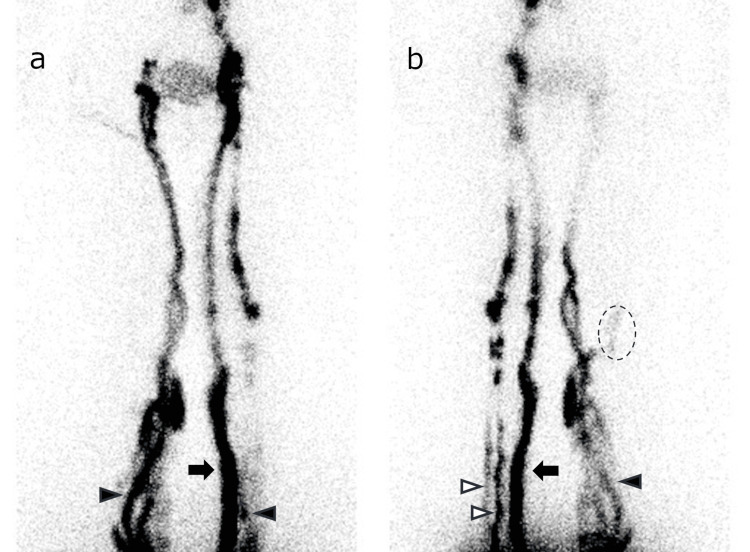 Figure 4
Figure 4| Male | Female | |
| n (total 26) | 3 (11.5%) | 23 (88.5%) |
| Limbs | 6 (11.5%) | 46 (88.5%) |
| Age (yrs) | 69-72 (median 70) | 20–85 (median 60) |
| ISL Stage | ||
| 0 | 2 (3.8%) | 18 (34.6%) |
| 1 | 4 (7.7%) | 3 (5.8%) |
| 2early | 0 | 15 (28.8%) |
| 2late | 0 | 10 (19.2%) |
| 3 | 0 | 0 |
| item | ISL stage | p-value* | ||
| 0 | 1–2 | |||
| AM | (+) | 16 | 14 | <0.05 |
| (−) | 4 | 18 | ||
| AL | (+) | 13 | 12 | 0.08 |
| (−) | 7 | 20 | ||
| PM | (+) | 12 | 7 | <0.05 |
| (−) | 8 | 25 | ||
| PL | (+) | 11 | 9 | 0.09 |
| (−) | 9 | 23 | ||
| DB | (+) | 3 | 24 | <0.01 |
| (−) | 17 | 8 | ||
| n | 0–1 | 1 | 21 | <0.01 |
| 2–4 | 19 | 11 | ||
| item | ISL stage | p-value* | ||
| 0–1 | 2 | |||
| AM | (+) | 18 | 12 | 0.16 |
| (−) | 8 | 14 | ||
| AL | (+) | 16 | 9 | 0.10 |
| (−) | 10 | 17 | ||
| PM | (+) | 13 | 6 | 0.08 |
| (−) | 13 | 20 | ||
| PL | (+) | 13 | 7 | 0.15 |
| (−) | 13 | 19 | ||
| DB | (+) | 8 | 19 | <0.01 |
| (−) | 18 | 7 | ||
| n | 0–1 | 5 | 17 | <0.01 |
| 2–4 | 21 | 9 | ||
| item | Sens | Spec | PPV | NPV | Acc |
| AM (−) | 0.56 | 0.80 | 0.82 | 0.53 | 0.65 |
| AL (−) | 0.63 | 0.65 | 0.74 | 0.52 | 0.63 |
| PM (−) | 0.78 | 0.60 | 0.76 | 0.63 | 0.71 |
| PL (−) | 0.72 | 0.55 | 0.72 | 0.55 | 0.65 |
| DB (+) | 0.75 | 0.85 | 0.89 | 0.68 | 0.79 |
| n ≤1 | 0.66 | 0.95 | 0.95 | 0.63 | 0.77 |
| item | Sens | Spec | PPV | NPV | Acc |
| AM (−) | 0.54 | 0.69 | 0.64 | 0.60 | 0.62 |
| AL (−) | 0.65 | 0.62 | 0.63 | 0.64 | 0.63 |
| PM (−) | 0.77 | 0.50 | 0.61 | 0.68 | 0.63 |
| PL (−) | 0.73 | 0.50 | 0.59 | 0.65 | 0.62 |
| DB (+) | 0.73 | 0.69 | 0.70 | 0.72 | 0.71 |
| n ≤1 | 0.65 | 0.81 | 0.77 | 0.70 | 0.73 |
| Method | LyS4 | Ordinal LyS [ | US [ | MR [ | LA [ | ICG [ |
| Complexity | Simple | Simple | Difficult | Simple | Difficult | Simple |
| Depiction of lymphatic vessels | Good | Limited | Limited | Good | Good | Limited |
| Invasiveness | Slight | Slight | None | Slight | High | Slight |
| Radiation exposure | Expose | Expose | None | None | Expose | None |
| Other limitation | Be aware of the risk of an allergy to contrast media. Patients with MR contraindications cannot be tested. | Be aware of the risk of an allergy to contrast media. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic System and Diseases · Diagnosis and Treatment of Venous Diseases · Systemic Sclerosis and Related Diseases
Introduction
Lymphedema is a progressive and chronic accumulation of protein-rich lymph fluid in the interstitial space due to a disruption of lymph nodes and lymphatic vessels [1]. Overall, 140-250 million people are estimated to be affected by lymphedema worldwide [1-3]. The diagnosis of lymphedema is difficult, but patients' clinical symptoms and clinical history are of primary importance [1]. The International Society of Lymphology (ISL) proposed the staging system of lymphedema. The ISL system can be used to determine the stage of lymphedema based primarily on the findings of a noninvasive examination when a treatment plan is being considered. This method does not include anatomical features or genetic abnormalities and has room for improvement, but at present it is the only agreed-upon assessment method for pre-treatment evaluation of lymphedema [4].
The use of several imaging modalities to evaluate a patient's lymph flow status has been suggested, including ultrasonography [5], lymphangiography [6,7], lymphatic scintigraphy [8], contrast-enhanced magnetic resonance imaging (contrast-enhanced MR) [9], and indocyanine green (ICG) fluorescence lymphangiography [10]. Among the reports concerning the use of lymphatic scintigraphy for evaluating lower-limb lymphedema, a study by Maegawa et al. classified lymphatic scintigraphy findings in lymphedema cases into five categories; the study also described these findings' relationships with indications for treatment [11]. A correlation between lymphangiography findings and edema staging was reported by Pecking et al. [12]. However, the injection point at radioisotope administration was only the first interdigital web in both the Maegawa et al. and Pecking et al. studies, which depicts a limited region of lymphatic vessels. Our institution also performed lymphoscintigraphy using a single injection previously. This is not a proper verification, but a retrospective review of 56 limbs examined using the single-injection method in past lymphoscintigraphy exams of our institution revealed that lymphatic vessels were detected in nearly all examinations (52/56, 92.9%) in the anterior lower leg region, whereas few cases were observed in the posterior region (6/56, 10.7%).
Shinaoka et al. used ICG fluorescent lymphangiography to depict four lymphatic vessel regions, i.e., anteromedial (AM), anterolateral (AL), posteromedial (PM), and posterolateral (PL) regions. They administered ICG at four locations in each limb and tracked the lymphatic vessels; their analyses revealed that the results correlated with lymphedema staging [13]. Based on that study, we decided to obtain lymphatic scintigraphy images by administering radioisotopes at four locations in each limb. We conducted the present study to evaluate the relationship between lymphatic scintigraphy findings and lymphedema staging and investigate the usefulness of this four-point dermal-injection lymphatic scintigraphy (LyS4) method.
This article was previously presented at the #60 The Japanese Society of Nuclear Medicine, Kyushu Regional Meeting on February 1, 2025.
Materials and methods
Patients
The patients who underwent a LyS4 examination of their lower limbs at Kyushu University Hospital during the period from March 2024 to March 2025 were included in this study. We excluded patients with a history of surgical treatment of a lower limb. The stage of lower-limb lymphedema was diagnosed by our institution's plastic surgeons, using the ISL staging system [4]. This study was a retrospective study and was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the institutional review board of Kyushu University (assignment no. 25054).
A final total of 26 patients (52 limbs) were enrolled. The patients were 23 females and three males aged 20-85 years (median 65 years).
Four-point dermal-injection lymphatic scintigraphy of lower limbs
In the patients' LyS4 examinations, technetium-99m human serum albumin diethylenetriamine pentaacetic acid (^99m^Tc-HSA-DTPA) was injected. The four dermal-injection points were the first interdigital web, slightly below the area of the lateral malleolus, slightly below the area of the medial malleolus, and the lateral side of the feet near the fifth digit of both feet (Figure 1), referring to the above-cited Shinaoka et al. study [13]. These injection points were confirmed by a plastic surgeon and marked on the patient's skin before the injection. The injection dose at each point was 70-80 MBq.
The injection points in the LyS4 examination.a–c: The injection points in the LyS4 examination. Technetium-99m human serum albumin diethylenetriamine pentaacetic acid (99mTc-HSA-DTPA) is injected at the first interdigital web (a: arrow), slightly below the area of the lateral malleolus (b: arrow), the lateral side of the feet near the fifth digit (b: arrowhead) and slightly below the area of the medial malleolus (c: arrow) and of both feet before the image acquisition.LyS4: four-point dermal injection lymphatic scintigraphy
A SPECT/CT system (NM/CT 870 CZT, GE HealthCare, Waukesha, WI, USA) and a wide-energy high-resolution (WEHR) collimator were used to acquire whole-body images at 10, 20, 30, 40, 50 and 60 min after the injection of ^99m^Tc-HSA-DTPA. The whole-body imaging protocol consisted of spot images of the whole-body dorsal/ventral view in a matrix of 256×1024 pixels. The whole-body scan was obtained at a 22.0 cm/min table feed rate. SPECT images of each lower limb were obtained with acquisitions in 60 views (10 sec/view) with matrix of 128×128 pixels. CT scans were also performed, with a 5-mm section thickness (130 keV, 30 mAs).
Image evaluation
All whole-body images were referred for image evaluation by two radiologists. As part of the image evaluation, the positive or negative appearance of lymphatic vessels in the four regions (AM, AL, PM, and PL) was determined without considering the degree of accumulation in the lymphatic vessels. If the two radiologists had different judgments, the decision was made by consensus after discussion (Figure 2). Dermal backflow (DB) was considered positive if extra accumulation outside of the lymphatic vessels was observed in the limb. The LyS4 result items, such as the appearance of AM, AL, PM, PL, DB, and the number of the appeared lymphatic vessel regions, were evaluated. The images and patient information used in this study were approved by the IRB as data collected within the observation period. All figures in this manuscript were original data courtesy of our institution.
Representative LyS4 images.The anterior (a, c, d, e) and posterior (b, f) planar images 60 min after radioisotope injection. The four lymphatic vessel regions are depicted: posteromedial (PM; c, arrow), anteromedial (AM; d, arrow), anterolateral (AL; e, arrow), posterolateral (PL; f, arrow). The posterolateral lymphatic vessels of the left limb are not depicted in this image.LyS4: four-point dermal injection lymphatic scintigraphy, AL: anterolateral, AM: anteromedial, PL: posterolateral, PM: posteromedial
Statistical analysis
The χ^2^-test was used to determine the correlation between the patients' LyS4 result items and their ISL stages. Probability (p)-values <0.05 were considered significant. All of the statistical analyses were performed using the software program JMP pro 17 (SAS Institute, Cary, NC, USA). Also, the diagnostic performance of the LyS4 for distinguishing lymphedema from a normal limb and for distinguishing moderate lymphedema (ISL stage 0 or 1) from severe lymphedema (ISL stage 2early or 2late).
Results
The patients' ISL stages of each limb were stage 0 (n=20), stage 1 (n=7), and stage 2 (n=25). The stage 2 cases include 15 early-phase (2early) and 10 late-phase (2late). No patient was stage 3 (Table 1).
Tables 2, 3 present the correlations between the image evaluation results (i.e., AM, AL, PM, PL, DB, and the number of lymphatic vessels depicted) and the ISL stage. Our analyses revealed that the absence of AM or PM accumulation and the appearance of DB can be used to distinguish lymphedema, with statistical significance. Another significant finding was that two or more lymphatic vessels were depicted if the limb had no symptoms (Table 2). Regarding the differentiation of moderate lymphedema from severe lymphedema, we obtained two significant findings: the patients with severe lymphedema showed the appearance of DB or had 0 or 1 as the number of lymphatic vessels depicted (Table 3).
The diagnostic performance of the LyS4 parameters was summarized in Tables 4, 5. Relatively high accuracy for distinguishing lymphedema from a normal limb was observed for the appearance of PM (0.71), DB (0.79), and the number of lymphatic vessels depicted (0.77) (Table 4). Notably, the specificity of the number of lymphatic vessels depicted was high at 0.95. The appearance of DB and the number of lymphatic vessels depicted showed relatively high accuracy for distinguishing moderate lymphedema from severe lymphedema.
Discussion
We described the new lymphatic scintigraphy method, LyS4, determined the correlations of LyS4 parameters with the ISL stage of lower limbs, and evaluated the diagnostic ability of this method. The results of our analyses demonstrated that the appearance of AM, PM, and DB and the number of lymphatic vessels depicted are significant factors that can be used to distinguish ISL stage 0 from ISL stage 1. In addition, the appearance of DB and the number of lymphatic vessels depicted are significant factors for distinguishing ISL stages 0 and 1 from ISL stage 2. Regarding the diagnostic performance of LyS4, the accuracy values distinguishing ISL stage 0 from ISL stages 1 and 2 were as follows: the appearance of DB (0.79) and the number of lymphatic vessels depicted (0.77); the corresponding accuracy values for distinguishing ISL stages 0 and 1 from ISL stage 2 were 0.71 and 0.73, respectively. In these results, the absence of PM visualization may indicate the presence of stage 1 or higher lymphedema. Furthermore, the number of lymphatic vessels specifically visualized by LyS4 is useful for distinguishing the presence or absence of lymphedema and may also provide information regarding its severity. The PM visualization and the number of lymphatic vessels are specific findings obtained by the LyS4, which is less likely to be obtained by the single-injection methods, highlighting the potential utility of LyS4.
In the Maegawa et al. study of ICG fluorescence lymphangiography, the accuracy of the appearance of DB for distinguishing ISL stage 0 from ISL stage ≥1 was 0.80, and the accuracy for distinguishing ISL stages 0 and 1 from ISL stage ≥2 was 0.78 [11]. These data are similar to those obtained in the present study.
Using the original staging system as a reference for scintigraphy results, Pecking et al. reported that the accuracy for distinguishing ISL stage 0 from ISL stage ≥1 was 0.88, and the accuracy for distinguishing ISL stages 0 and 1 from ISL stage ≥2 was 0.96 [12]. Those results are very good, but that study involved a single-point injection examination. In addition, the speed of lymphatic transportation, which may depend on individual decisions, should be taken into account.
The LyS4 method can delineate lymphatic vessels in all areas of the lower limbs, especially deeper lymphatic vessels that are relatively difficult to delineate with ICG fluorescence lymphangiography (Figures 3, 4). Detailed lymphatic flow information is expected to provide additional information that will be more useful in determining treatment strategies for lymphedema, the indications for lymphatic venous anastomosis, and the selection of the surgical site.
Anterior and posterior LyS4 images of a female in her 30s with ISL stage 1 lymphedema of the left limb. Anterior (a) and posterior (b) LyS4 images of a female in her 30s with ISL stage 1 lymphedema of the left limb. These images were acquired 60 min after injection. All four lymphatic vessels appeared with DB at the proximal thigh in the left limb. The right limb, which was diagnosed as normal, showed PM and AL, but AM and PL were not detected (white arrow: AL, black arrow: PM, white arrow head: AM, black arrow head: PL)LyS4: four-point dermal injection lymphatic scintigraphy, ISL: International Society of Lymphology, AL: anterolateral, AM: anteromedial, DB: dermal backflow, PL: posterolateral, PM: posteromedial
Anterior and posterior LyS4 images of a female in her 40s with the late-phase of ISL stage 2 lymphedema of the right limb.Anterior (a) and posterior (b) LyS4 images of a female in her 40s with the late-phase of ISL stage 2 lymphedema of the right limb. These images were acquired 60 min after injection. Only AM appeared in the right limb with DB at the distal lower leg. In the left limb, which was diagnosed as the normal limb, AM, PM and AL were detected with no DB (white arrow: AL, black arrow: PM, white arrow head: AM, black arrow head: PL, dotted circle: DB).LyS4: four-point dermal injection lymphatic scintigraphy, ISL: International Society of Lymphology, AL: anterolateral, AM: anteromedial, DB: dermal backflow, PL: posterolateral, PM: posteromedial
Our present findings demonstrate that LyS4 provides more information about lymphatic vessels than conventional single-point lymphatic scintigraphy while maintaining adequate evaluation performance. Several types of examination are available for evaluating lymphatic vessels in lymphedema of the lower extremities (Table 6). The LyS4 examination is superior to ultrasonography and ICG fluorescence lymphangiography for revealing details of lymphatic vessels. It is also superior to lymphangiography in its relative simplicity. At the point of radiation exposure, contrast-enhanced lymphatic MR produces no radiation exposure; however, it is difficult to perform in patients for whom MR is contraindicated or who are allergic to MR contrast media. These patients can undergo LyS4 with no limitation. Therefore, although there is a slight radiation exposure, LyS4 is unique in that it provides objectively good lymphatic vessel delineation.
We did not use any parameters from SPECT/CT images as a criterion for evaluation in this study. This is because the imaging range of SPECT/CT was not standardized in the patient population, making it difficult to create evaluation parameters. We agree that SPECT/CT is useful for the evaluation of lymphatic vessels as Pecking et al. reported [12]. An evaluation method that incorporates SPECT/CT imaging is a topic for a future study. We also did not address treatment decision-making or the prognostic value of LyS4 findings. We believe that the LyS4 method is useful for determining treatment strategies and predicting treatment efficacy, but further case collections and follow-ups are needed to verify this.
The proximal lymphatic system in the pelvis, abdomen, and chest was not mentioned in this study. In this study, the appearance of the lymph nodes was weaker than lymphatic vessels in almost all cases. We think that this is because we take images limited to 60 minutes after injection, which results to make weak uptake. Although not shown in the images presented in this report, visualization of the cisterna lactea, thoracic duct, and left venous angle was good, and images comparable to those obtained with the one-point method appear to have been acquired.
There are several limitations of this study. First, the number of patients in this study was small. We believe the LyS4 is a suitable method for evaluating lymphoedema; however, the number of cases is limited due to its novelty. Second, this study is a retrospective design; therefore, a prospective or multicenter evaluation would be beneficial. Third, the ISL stage 3 cases were not observed. This is because our institution rarely encounters severely progressed lymphoedema patients. We think the usefulness of LyS4 can be argued based on its potential to aid in treatment decision-making during early edema stages, even without including the ISL stage 3 case. However, this issue could potentially be resolved through multicenter research. The third point is that SPECT images of LyS4 were not used as diagnostic parameters in this study. Parameters with SPECT images may be useful for diagnosis with anatomical information compared to planar images; however, the timing of the SPECT examination is controversial. Furthermore, as noted in the Introduction, lymphoscintigraphy using a single injection provides poor visualization of posterior lymphatic vessels, making LyS4 potentially more useful in this regard. However, no reports have verified this point and necessitating precise validation.
Conclusions
For the evaluation of lower-limb lymphedema, the LyS4 method, i.e., four-point dermal-injection lymphatic scintigraphy, is a relatively simple method that provides clear images of lymphatic vessels. To confirm the severity of lower-limb lymphedema, the number of lymphatic vessels depicted and the depiction of dermal backflow by LyS4 may be one of the viewpoints. LyS4 is expected to contribute to decisions about the treatment strategies for lymphedema of the lower extremities and assessments of the efficacy of treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lymphedema: a comprehensive review Ann Plast Surg Shimony A Tidhar D 22860200810.1097/SAP.0b 013e 318165 f 1f 518216521 · doi ↗ · pubmed ↗
- 2The third circulation: radionuclide lymphoscintigraphy in the evaluation of lymphedema J Nucl Med Szuba A Shin WS Strauss HW Rockson S 4357442003 https://jnm.snmjournals.org/content/44/1/43.short 12515876 · pubmed ↗
- 3Surgical treatment and rehabilitation strategies for upper and lower extremity lymphedema: a comprehensive review Medicina (Kaunas) de Sire A Losco L Lippi L 58202210.3390/medicina 58070954 PMC 932442635888673 · doi ↗ · pubmed ↗
- 4The diagnosis and treatment of peripheral lymphedema: 2020 consensus document of the International Society of Lymphology Lymphology 31953202032521126 · pubmed ↗
- 5The diagnosis and treatment of peripheral lymphedema: 2023 consensus document of the International Society of Lymphology Lymphology 13315156202339207406 · pubmed ↗
- 6Lymphangiography in man; a method of outlining lymphatic trunks at operation Clin Sci Kinmonth JB 132011195214896514 · pubmed ↗
- 7Feasibility of ultrasound-guided intranodal lymphangiogram for thoracic duct embolization J Vasc Interv Radiol Nadolski GJ Itkin M 6136162320122244059010.1016/j.jvir.2012.01.078 · doi ↗ · pubmed ↗
- 8Pearls and pitfalls of radionuclide imaging of the lymphatic system. Part 2: evaluation of extremity lymphoedema Br J Radiol Scarsbrook AF Ganeshan A Bradley KM 2192268020071672841210.1259/bjr/68256780 · doi ↗ · pubmed ↗